Key points
- Initial signs of symptoms of Ebola disease are nonspecific and can be confused with other more common infectious diseases like malaria, typhoid fever, meningococcemia, and other bacterial infections.
- Patients with Ebola disease generally have an abrupt onset of fever and symptoms 8 to 10 days after exposure.
- After 4-5 days of illness, patients may develop gastrointestinal symptoms like severe watery diarrhea, nausea, vomiting, and abdominal pain.
- Bleeding is not universally present in people with Ebola disease.
Disease presentation
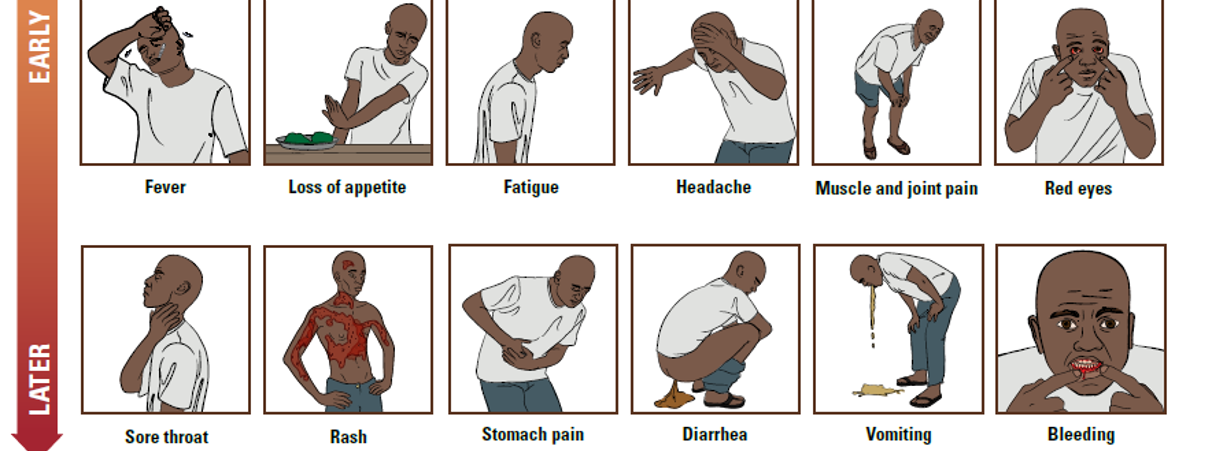
Early stage of disease/"dry" symptoms
Patients with Ebola disease generally have an abrupt onset of fever and symptoms 8-10 days after exposure. These "dry" initial signs and symptoms are nonspecific and may include:
- Elevated body temperature or subjective fever
- Chills
- Myalgia
- Fatigue
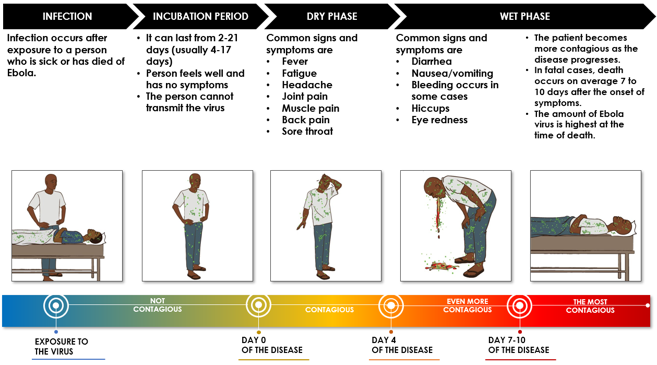
Mid-late stage of disease/"wet" symptoms
Four to 5 days after symptom onset, patients can progress to gastrointestinal symptoms, or "wet" symptoms, which can include:
- Severe watery diarrhea
- Nausea
- Vomiting
- Abdominal pain
Other symptoms may develop, including chest pain, shortness of breath, headache, or confusion. Patients often have eye irritation and redness. Hiccups have been reported. Seizures may occur, and cerebral edema has been reported. Pregnant women may experience spontaneous miscarriages.
Bleeding is not universally present. However, it can manifest later in the course of disease as petechiae, ecchymosis or oozing from venipuncture sites, mucosal hemorrhage, or blood in stool or vomitus. In general, unexplained bleeding is reported in 40% of patients.
By days 5 to 7, patients may develop a mixture of flat and raised red lesions on the skin that can peel or flake off. These lesions are found on the neck, trunk, and arms.
The most common signs and symptoms reported during the 2014–2016 West Africa outbreak include fever (87%), fatigue (76%), vomiting (68%), diarrhea (66%), and loss of appetite (65%).
Patients with fatal disease usually develop more severe clinical signs early during infection and die of complications typically between days 6 and 16. Complications include multiorgan failure and septic shock. In non-fatal cases, patients may have fever for several days and improve, typically around day 6. Patients who survive can have a prolonged convalescence.
Diagnostic laboratory findings
Laboratory findings may include:
- Leukopenia, frequently with lymphopenia, followed later by elevated neutrophils and a left shift
- Decreased platelet counts in the 50,000-100,000 range
- Elevated amylase, reflecting pancreatic involvement (inflammation/infection)
- Elevated hepatic transaminases with aspartate aminotransferase (AST) exceeding alanine aminotransferase (ALT); these values may peak at more than 1,000 IU/L
- Proteinuria
- Prolonged prothrombin (PT) and partial thromboplastin times (PTT) and elevated fibrin degradation products consistent with disseminated intravascular coagulation
If you suspect Ebola disease in a patient
Alternate differentials
Healthcare providers should conduct an initial screening to determine if a patient has relevant exposure history and clinical signs consistent with a viral hemorrhagic fever (VHF) like Ebola. After an initial screening, if a healthcare provider suspects a patient may have a VHF or other high-consequence disease, they should immediately follow infection prevention guidance and contact their health department for testing recommendations.