Toxins and Health Impacts
The collapse of the Twin Towers created massive dust clouds that filled the air and left hundreds of highly populated city blocks covered with ash, debris, and harmful particles.
In Lower Manhattan, the plane crashes—which resulted in the collapse of the Twin Towers—created massive dust clouds that filled the air and left hundreds of highly populated city blocks covered with ash, debris, and harmful particles, including asbestos, silica, metals, concrete, and glass. Fires within the debris pile and the collapse of 7 WTC burned through the end of December 2001 with continued flare-ups in 2002, releasing carcinogenic combustion by-products. These contaminants remained in Lower Manhattan and parts of Brooklyn for an undetermined amount of time after 9/11. Responders, local workers, residents, students, and others had potential for acute exposures in the early days and continuing exposure from residual materials—indoors and outside—as well as exposure to toxic gases, smoke, vapors, and combustion by-products from continuing fires.
New York City Police Aviation Unit Detective Gregory Semendinger photographed the spread of the dust cloud from his vantage point above Lower Manhattan on 9/11.
Learn more about his experience.
Officials declared the plane crash in Somerset County near Shanksville, Pennsylvania a crime scene; the crash created hazardous conditions—including fiery hot spots and smoke—for workers and volunteers. At the Pentagon in Arlington, Virginia, responders, cleanup crews, and construction workers were potentially exposed to smoke, jet fuel, heat from the fire, hazardous chemicals, and harmful debris.

Pentagon After Attack September 11, 2001.
Photograph courtesy of the National Archive and Records Administration, DM-SD-02-03902.

Lower Manhattan After South Tower Collapse, September 11, 2001.
Photograph courtesy of New York City Police Detective Gregory Semendinger.

The Hughes family lived one block east of the World Trade Center towers. This photo was taken from a window in their home on September 12, 2001.
Photograph by Thomas Hughes.
Photograph courtesy of Catherine McVay Hughes.

Photograph taken by Allan Tannenbaum on July 28, 2006 depicting Kelly Coangelo, lower Manhattan resident, holding a baggie of dust from her apartment and the cheesecloth she used to filter her air conditioner. The World Trade Center site is visible outside her apartment window.
Photograph on loan from The National September 11 Memorial & Museum.
Exposure to 9/11 Agents
Analysis of hazards revealed numerous agents and experiences that could cause physical and psychological harm. Responders, recovery workers, and survivors were exposed to these at varying degrees.
In July 2018, the Administrator of the WTC Health Program released the Development of the Inventory of 9/11 Agents. This document defines the term “9/11 agent” and provides an inventory of chemical, physical, biological, and other hazards recognized as 9/11 agents by the WTC Health Program. The document references scientific, peer-reviewed literature of over 350 hazards that may have been present at the disaster areas and related sites designated in the James Zadroga 9/11 Health and Compensation Act (2010). It also includes hazards not identified in a published, peer-reviewed exposure assessment study, but which are reasonably assumed to have been present at any of the sites.
Exposure to some of these hazards has been linked to aggravating, contributing to, or causing various short- and long-term health conditions covered by the WTC Health Program, such as:
- Acute traumatic injuries (like burns, sprains, and fractures);
- Aerodigestive (airway and digestive) disorders (like asthma, GERD, and sleep apnea);
- Many types of cancers;
- Mental and behavioral health conditions (like PTSD, depression, and substance abuse); and
- Musculoskeletal disorders (like carpal tunnel syndrome and low back pain).
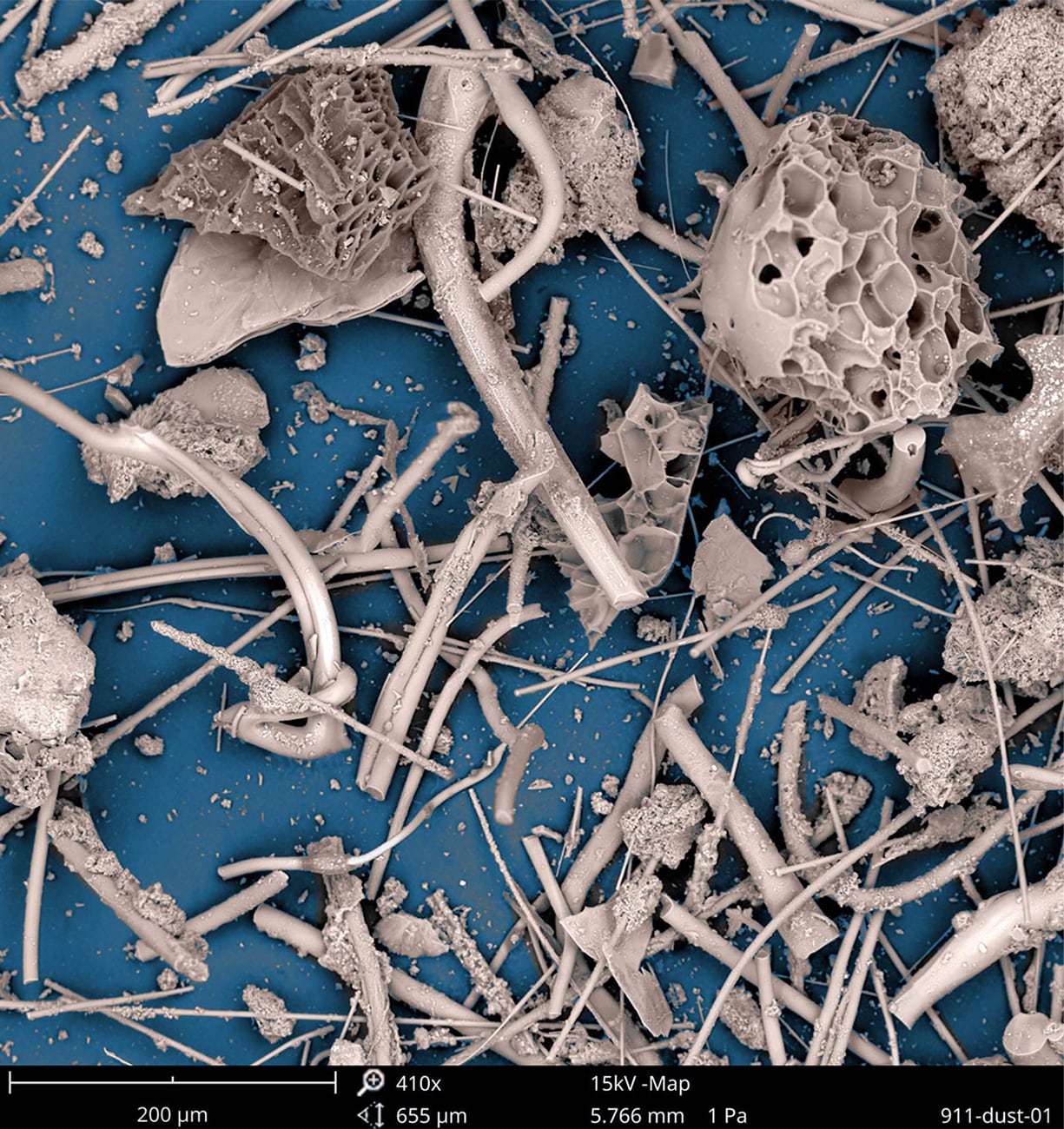
Photograph courtesy of NIOSH’s Health Effects Laboratory Division (HELD) and WTC Health Program.
Learn more about these photos.

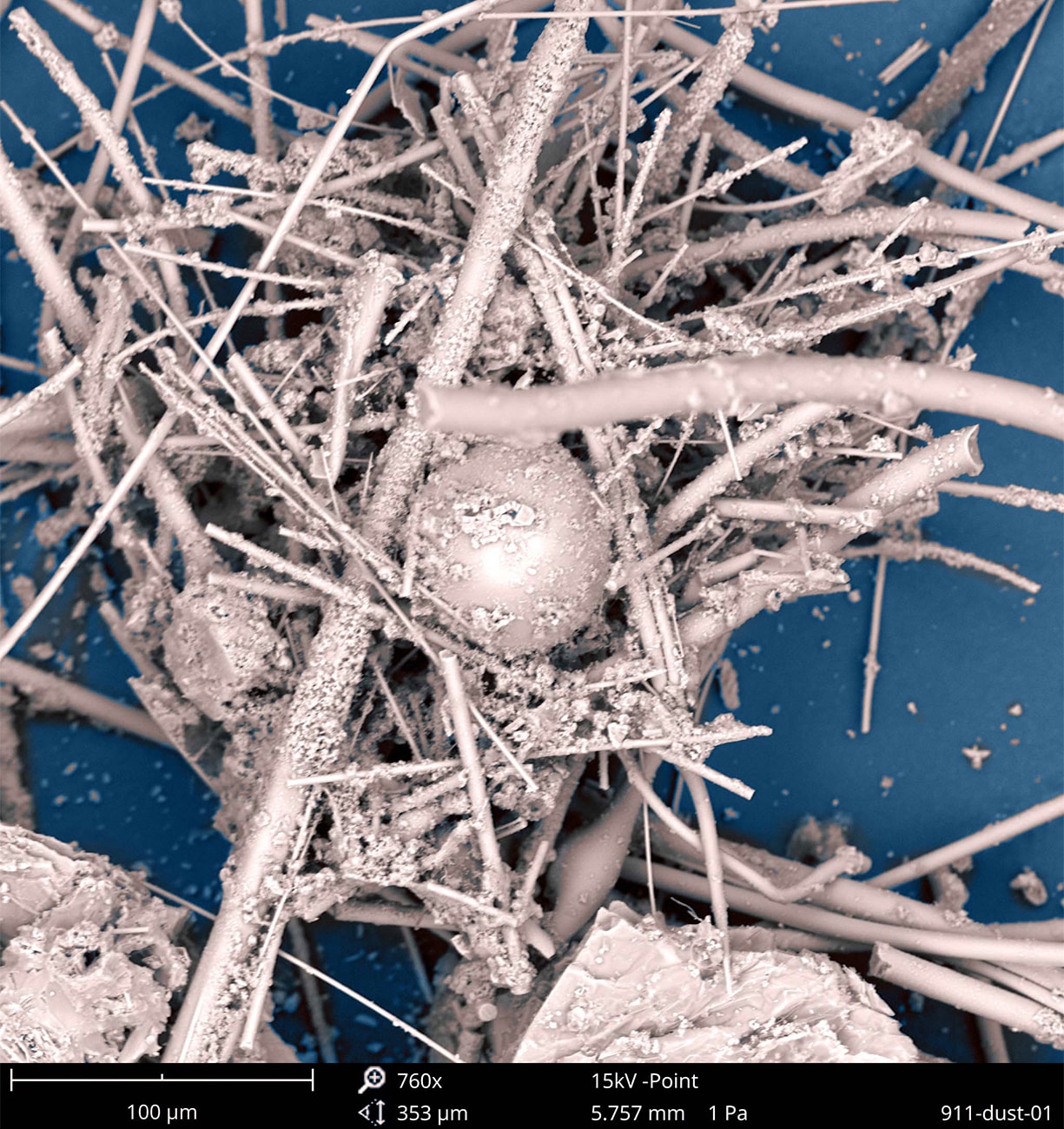
Photograph courtesy of NIOSH’s Health Effects Laboratory Division (HELD) and WTC Health Program.
Learn more about these photos.
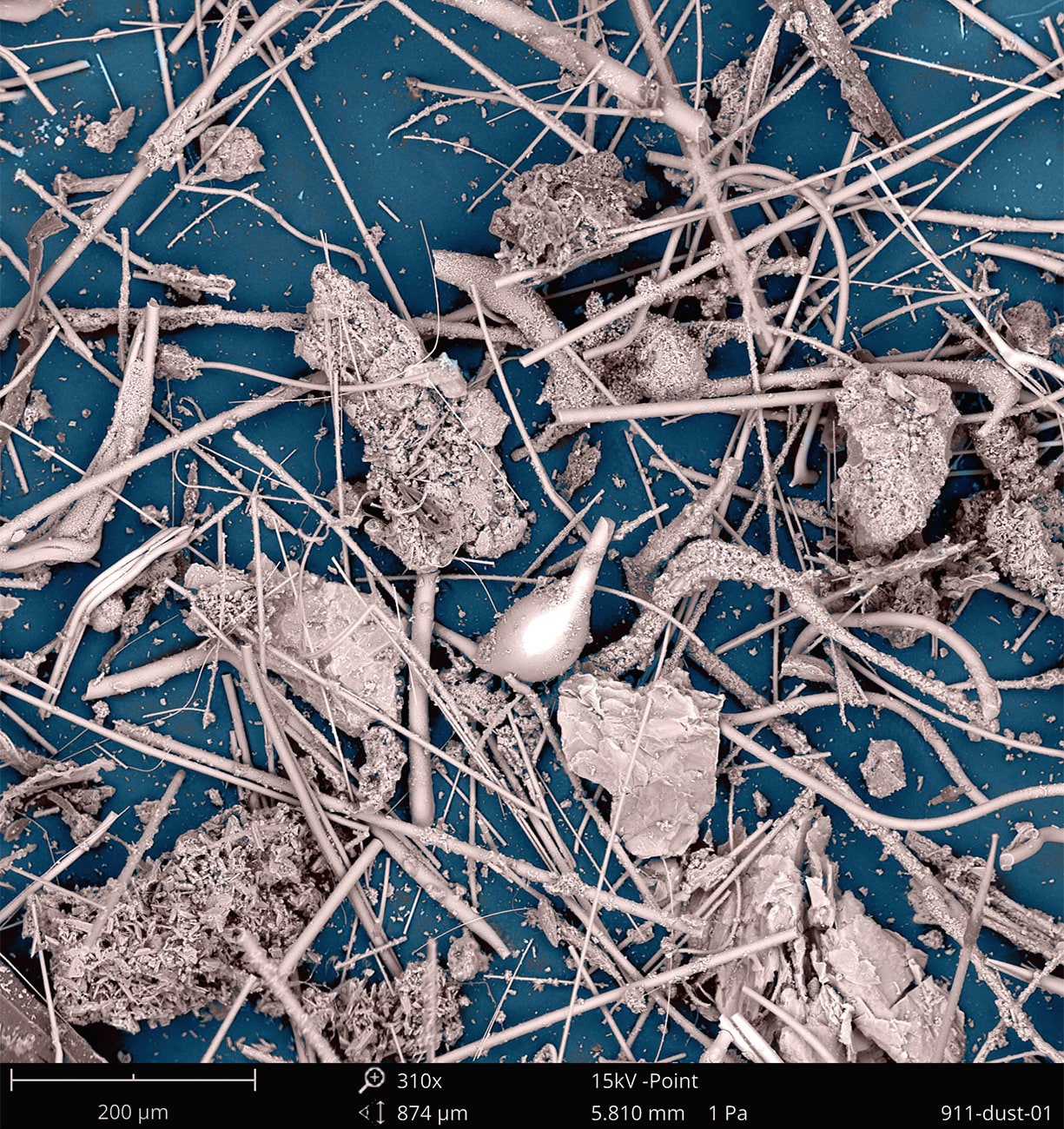
Photograph courtesy of NIOSH’s Health Effects Laboratory Division (HELD) and WTC Health Program.
Learn more about these photos.
Photograph courtesy of NIOSH’s Health Effects Laboratory Division (HELD) and WTC Health Program.
Learn more about these photos.
Health Impacts
An estimated 400,000 people were exposed to toxic contaminants, risk of physical injury, and physically and emotionally stressful conditions in the days, weeks, and months following the attacks. Responders who worked on the rescue, recovery, and relief efforts reported a range of illnesses soon after the attacks. Survivors who lived, worked, and attended school in Lower Manhattan, some who remained throughout and some who returned to their lives in the disaster area, started reporting illnesses as well.

Cartoon reproduction created and provided by Ali Shapiro, former Stuyvesant High School Student.
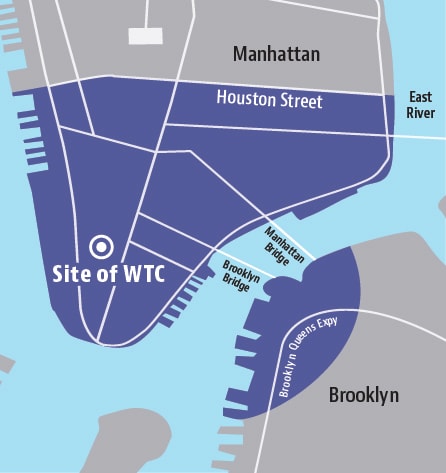
New York City Disaster Area Map
According to the James Zadroga 9/11 Health and Compensation Act, as amended (2010), the term ‘New York City Disaster Area’ (NYCDA) means the area within New York City that is the area of Manhattan that is south of Houston Street; and any block in Brooklyn that is wholly or partially contained within a 1.5-mile radius of the former World Trade Center site. The NYCDA is used to determine WTC Survivor eligibility. The WTC Responder eligibility area varies from the NYCDA and includes the area in Lower Manhattan south of Canal Street and WTC-related locations not shown in this map, such as New York Offices of the Chief Medical Examiner, certain barge loading piers, the Staten Island Landfill, Pentagon site, and Shanksville, PA site. Some eligible responder duties, such as vehicle maintenance, may have been performed outside these areas.

Photograph courtesy of the WTC Health Program.
Early Responses
On October 11, 2001, a Town Hall was held in Lower Manhattan featuring speakers representing the Fire Department of the City of New York (FDNY), local medical schools, and occupational safety and health centers. It was the first public forum where responders, residents, and others publicly aired their health concerns. Clinicians and scientists called attention to the newly described WTC cough in firefighters. They called for investigations and interventions, stating there was potential for adverse health effects in responders and among the broader affected communities. Many more events would follow, with mounting community calls for widespread 9/11 health effects to be assessed and addressed. In the months immediately after the attacks, New York City (NYC) provided limited funds to cover treatment for some responders who were NYC employees. Later, philanthropic funds helped to expand treatment for other responders.
As a result of continued advocacy, in 2002, FDNY and the Mount Sinai School of Medicine – now the Icahn School of Medicine at Mount Sinai (MSSM) —received federal funding for a one-time health screening of responders.
With a national focus on the heroism of firefighters, police, and other responders, the affected survivor community at large was initially overlooked. Following the attacks, many residents remained downtown as they were publicly told the air was safe to breathe. Many others who lived, worked, or attended school in the area were encouraged to quickly return to their homes, schools, and workplaces. Their health was placed at risk.
In 2002, medical providers at Bellevue Hospital began to document new onset cough, wheeze, and shortness of breath among downtown residents. Local tenant and community organizations, including a coalition under the banner of the Beyond Ground Zero (BGZ) Network, advocated for recognition of community health needs. Bellevue Hospital partnered with BGZ to set up a pilot clinic to treat affected community members. Initially unfunded, this program gained support from the American Red Cross in 2005. On the anniversary of 9/11 in 2006, NYC announced local funding for the WTC Environmental Health Center (WTC EHC) at Bellevue Hospital (part of NYC Health + Hospitals [H+H]).
In 2004, after much stakeholder lobbying, Congress provided funds through the National Institute for Occupational Safety and Health (NIOSH) to deliver periodic medical monitoring to responders. Recipients included FDNY, MSSM, New York University (NYU), Queens College, Rutgers University, and the State University of New York at Stonybrook (SUNY). The collaborative efforts of clinicians and scientists at these institutions revealed the persistence of many health problems that led to additional Congressional funds to cover treatment costs in 2006. Collectively, these institutions became the WTC Medical Monitoring and Treatment Program, administered by NIOSH. To provide services for responders outside the NY-NJ metropolitan area, NIOSH contracted with Logistics Health Incorporated (LHI) to create a National Responder Program.
In 2008, Congress expanded its 9/11-related funding to provide services to survivors, in addition to the responders. As a result, the NYC Health and Hospitals WTC EHC program obtained its first federal funds from NIOSH in 2008 and continued to screen and provide medical care for survivors—residents, local workers, students, and others—harmed by the 9/11 terror attacks.
These predecessor programs became part of the congressionally established “WTC Health Program” with the passage of the James Zadroga 9/11 Health and Compensation Act of 2010.

Photograph courtesy of the Prints and Photographs Division, Library of Congress, Washington D.C.
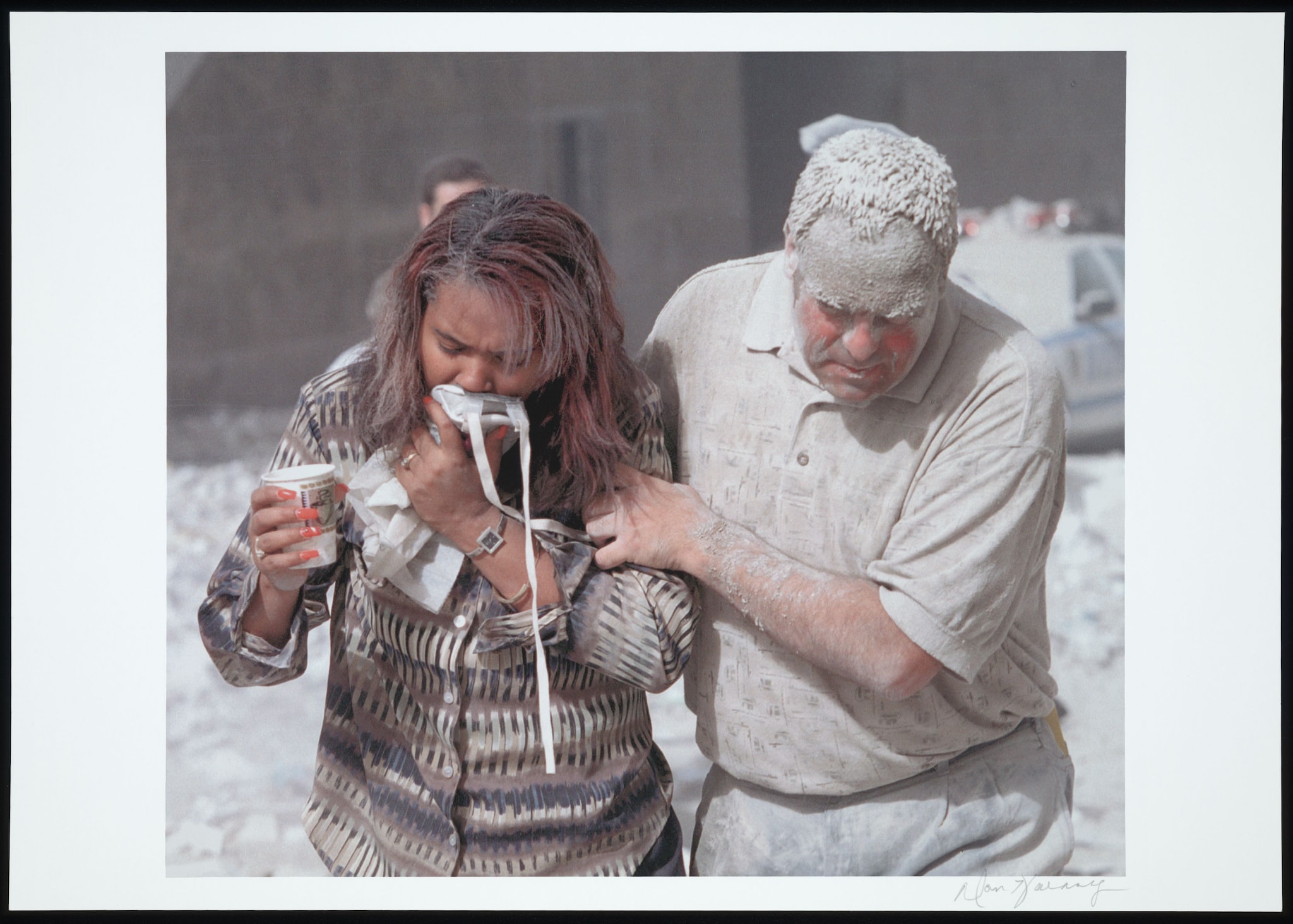
Two people covered in dust evacuate from Ground Zero.
Photograph by Don Halasy.
Photograph courtesy of the Prints and Photographs Division, Library of Congress, Washington D.C.

Two men carry an injured woman down a street littered with paper, ashes, and dust from the Twin Towers’ collapse.
Photograph by Don Halasy.
Photograph courtesy of the Prints and Photographs Division, Library of Congress, Washington D.C.
Page Last Reviewed: October 23, 2023 | Page Last Updated: July 30, 2024