Attention Deficit Hyperactivity Disorder Among Children Aged 5–17 Years in the United States, 1998–2009
- Key findings
- The percentage of children ever diagnosed with ADHD increased from 1998 through 2009 among both boys and girls.
- ADHD prevalence varied by race and ethnicity, but differences between most groups narrowed from 1998 through 2009.
- From 1998 through 2009, ADHD prevalence increased for children with family income less than 100% of the poverty level and for those with family income between 100% and 199% of the poverty level.
- ADHD prevalence rose in the Midwest and South regions of the United States from 1998 through 2009.
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 70, August 2011
PDF Version (428 KB)
Lara J. Akinbami, M.D.; Xiang Liu, M.Sc.; Patricia N. Pastor, Ph.D.; and Cynthia A. Reuben, M.A.
Key findings
Data from the National Health Interview Survey, 1998–2009
- The percentage of children ever diagnosed with attention deficit hyperactivity disorder (ADHD) increased from 7% to 9% from 1998–2000 through 2007–2009.
- ADHD prevalence trends varied by race and ethnicity. Differences between groups narrowed from 1998 through 2009; however, Mexican children had consistently lower ADHD prevalence than other racial or ethnic groups.
- From 1998 through 2009, ADHD prevalence increased to 10% for children with family income less than 100% of the poverty level and to 11% for those with family income between 100% and 199% of the poverty level.
- From 1998 through 2009, ADHD prevalence rose to 10% in the Midwest and South regions of the United States.
Attention deficit hyperactivity disorder (ADHD) is one of the most common mental health disorders of childhood (1). The symptoms of ADHD (inattention, impulsive behavior, and hyperactivity) begin in childhood and often persist into adulthood. These symptoms frequently lead to functional impairment in academic, family, and social settings (2,3). The causes and risk factors for ADHD are unknown, but genetic factors likely play a role (4). Diagnosis of ADHD involves several steps, including a medical exam; a checklist for rating ADHD symptoms based on reports from parents, teachers, and sometimes the child; and an evaluation for coexisting conditions (5). Recent national surveys have documented an increase in the prevalence of ADHD during the past decade (6,7). This report presents recent trends in prevalence and differences between population subgroups of children aged 5–17 years.
Keywords: race, ethnicity, poverty status, National Health Interview Survey
The percentage of children ever diagnosed with ADHD increased from 1998 through 2009 among both boys and girls.
- For the 2007–2009 period, an annual average of 9.0% of children aged 5–17 years had ever been diagnosed with ADHD—an increase from 6.9% in 1998–2000 (Figure 1).
- From 1998 through 2009, ADHD prevalence was higher among boys than girls: For boys, ADHD prevalence increased from 9.9% in 1998–2000 to 12.3% in 2007–2009, and for girls, from 3.6% to 5.5% during the same period.

NOTE: Access data table for Figure 1 [PDF 87 KB].
SOURCES: CDC/NCHS, Health Data Interactive and National Health Interview Survey.
ADHD prevalence varied by race and ethnicity, but differences between most groups narrowed from 1998 through 2009.
- ADHD prevalence increased from 1998–2000 to 2007–2009 for non-Hispanic white children (from 8.2% to 10.6%) and for non-Hispanic black children (from 5.1% to 9.5%) (Figure 2).
- In 1998–2000, non-Hispanic white children had higher ADHD prevalence compared with all other race groups, and Mexican children had the lowest prevalence.
- In 2007–2009, ADHD prevalence was similar among non-Hispanic white, non-Hispanic black, and Puerto Rican children. ADHD was lower among Mexican children compared with children in the three other racial and ethnic groups.

NOTE: Access data table for Figure 2 [PDF – 87 KB].
SOURCES: CDC/NCHS, Health Data Interactive and National Health Interview Survey.
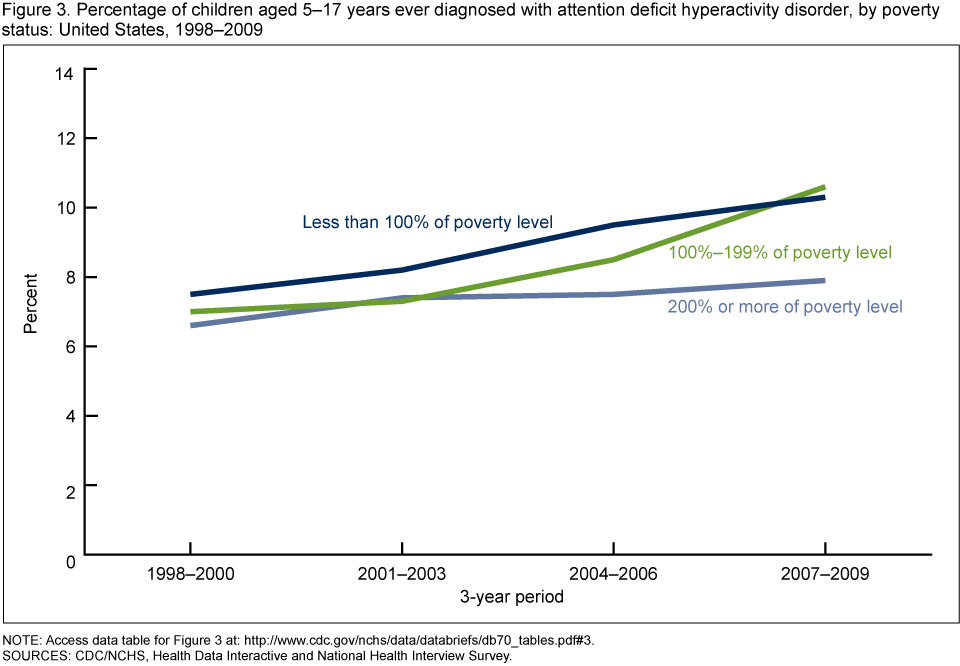
From 1998 through 2009, ADHD prevalence increased for children with family income less than 100% of the poverty level and for those with family income between 100% and 199% of the poverty level.
- From 1998–2000 to 2007–2009, ADHD prevalence increased from 7.5% to 10.3% for children with family income less than 100% of the poverty level, and from 7% to 10.6% for children with family income between 100% and 199% of the poverty level (Figure 3).
- In 1998–2000, ADHD prevalence was similar among all income groups, but in 2007–2009 the prevalence was higher among children with family income less than 100% or between 100% and 199% of the poverty level, compared with those with income greater than or equal to 200% of the poverty level.
NOTE: Access data table for Figure 3 [PDF – 87 KB].
SOURCES: CDC/NCHS, Health Data Interactive and National Health Interview Survey.
ADHD prevalence rose in the Midwest and South regions of the United States from 1998 through 2009.
- ADHD prevalence rose from 1998–2000 to 2007–2009 in the Midwest region (from 7.1% to 10.2%) and in the South region (from 8.1% to 10.3%) (Figure 4).
- In 1998–2000, ADHD prevalence was higher in the South region than in all other regions. In 2007–2009, ADHD prevalence was similar in the South and Midwest regions; prevalence in these two regions was higher than in the Northeast and West regions.

NOTES: For a listing of states in each of the four U.S. Census regions [PDF – 1 MB]. Access data table for Figure 4 [PDF – 87 KB].
SOURCES: CDC/NCHS, Health Data Interactive and National Health Interview Survey.
Summary
From 1998–2000 through 2007–2009, the prevalence of ADHD increased among children aged 5–17 years, from 6.9% to 9.0%. These increases were seen among both boys and girls, among children in most racial and ethnic groups except Mexican children, and among children with family income less than 200% of the poverty level. By geographic region, ADHD was more prevalent in the South and Midwest regions of the United States than in the Northeast and West regions during 2007–2009. Prevalence estimates in this report are based on parental report of the child ever receiving a diagnosis, and thus may be affected by the accuracy of parental memory (including recall bias), by differential access to health care between groups (diagnostic bias), or by willingness to report an ADHD diagnosis. One study that included clinical assessment of children for ADHD symptoms (8) found that only one-half of children meeting the criteria for ADHD had received a diagnosis of ADHD or regular medication treatment. For the present report, it was not possible to discern whether growing prevalence indicates a true change in prevalence or increased detection and diagnosis of ADHD. Nevertheless, the societal costs of ADHD—including those associated with medical, educational, and criminal justice resources—are large (8).
Definitions
ADHD prevalence: Estimated based on the number of adults responding “yes” to the question, “Has a doctor or health professional ever told you that your child had Attention Deficit Hyperactivity Disorder (ADHD) or Attention Deficit Disorder (ADD)?” This question is included in the standard National Health Interview Survey (NHIS) Sample Child questionnaire.
Poverty status or percentage of poverty level: Based on family income, family size, the number of children in the family, and, for families with two or fewer adults, on the age of the adults in the family. The poverty level is based on a set of income thresholds that vary by family size and composition. Families or individuals with income below their appropriate thresholds are classified as below the poverty level. These thresholds are updated annually by the U.S. Census Bureau to reflect changes in the Consumer Price Index for all urban consumers (9). Estimates by poverty status from NHIS are based on both reported and imputed family income (10).
Data source and methods
All ADHD prevalence estimates were obtained from the Health Data Interactive (HDI) table, “Attention deficit hyperactivity disorder, learning disability, behavior difficulty, ages 5–17: U.S., 1998–2009,” available from the Health Data Interactive website. NHIS data were used to estimate ADHD prevalence for this HDI table.
NHIS data are collected continuously throughout the year for the Centers for Disease Control and Prevention’s (CDC) National Center for Health Statistics (NCHS) by interviewers from the U.S. Census Bureau. NHIS collects information about the health and health care of the civilian noninstitutionalized U.S. population. Interviews are conducted in respondents’ homes, but follow-ups to complete interviews may be conducted over the telephone. The Sample Child component collects detailed data on health conditions for a randomly selected child in households with at least one child. A responsible adult, usually a parent, responds to the survey questions as proxy for the sample child. For further information about NHIS and the questionnaire, visit the NHIS website.
NHIS is designed to yield a sample that is representative of the civilian noninstitutionalized population of the United States, and the survey uses weighting to produce national estimates. Data weighting procedures are described in more detail elsewhere (11). Point estimates and estimates of corresponding variances for the HDI estimates were calculated using SUDAAN software (12) to account for the complex sample design of NHIS. The Taylor series linearization method was chosen for variance estimation.
Differences between percentages were evaluated using two-sided significance tests at the 0.05 level. Terms such as “higher than” and “less than” indicate statistically significant differences. Terms such as “similar” and “no difference” indicate that the statistics being compared were not significantly different. Lack of comment regarding the difference between any two statistics does not necessarily suggest that the difference was tested and found to be not significant.
All estimates shown in this report have a relative standard error less than or equal to 30%. The significance of trends was tested using weighted least squares regression models of the log of each outcome and Joinpoint software (13) to determine whether an apparent change over time was statistically significant, taking into account the standard error for each data point.
About the authors
Lara Akinbami, Xiang Liu, Patricia Pastor, and Cynthia Reuben are with the Centers for Disease Control and Prevention’s National Center for Health Statistics, Office of Analysis and Epidemiology.
References
- Fulton BD, Scheffler RM, Hinshaw SP, Levine P, Stone S, Brown TT, Modrek S. National variation of ADHD diagnostic prevalence and medication use: Health care providers and education policies. Psychiatr Serv 60(8):1075–83. 2009.
- Barkley RA. Associated cognitive, developmental, and health problems. In: Barkley RA, Murhpy KR, eds. Attention-deficit hyperactivity disorder: A clinical workbook. 3rd ed. New York, NY: Guilford Press 122–83. 2006.
- Yoshimasu K, Barbaresi WJ, Colligan RC, Killian JM, Voigt RG, Weaver AL, Katusic SK. Gender, attention-deficit/hyperactivity disorder, and reading disability in a population-based birth cohort. Pediatrics 126(4):e788–95. 2010.
- Khan SA, Faraone SV. The genetics of ADHD: A literature review of 2005. Curr Psychiatry Rep 8(5):393–7. 2006.
- American Academy of Pediatrics. Clinical practice guideline: Diagnosis and evaluation of the child with attention-deficit/hyperactivity disorder. Pediatrics 105(5):1158–70. 2000.
- CDC. Increasing prevalence of parent-reported attention-deficit/hyperactivity disorder among children—United States, 2003 and 2007. MMWR 59(44):1439–43. 2010.
- Boyle CA, Boulet S, Schieve LA, Cohen RA, Blumberg SJ, Yeargin-Allsopp M, et al. Trends in the prevalence of developmental disabilities in U.S. children, 1997–2008. Pediatrics 127(6):1034–42. 2011.
- Pelham WE, Foster EM, Robb JA. The economic impact of attention-deficit/hyperactivity disorder in children and adolescents. J Pediatr Psychol 32(6):711–27. 2007.
- U.S. Census Bureau: Poverty 2011.
- Schenker N, Raghunathan TE, Chiu P-L, Makuc DM, Zhang G, Cohen AJ. Multiple imputation of family income and personal earnings in the National Health Interview Survey: Methods and examples [PDF 814 KB]. Hyattsville, MD: National Center for Health Statistics. 2008.
- Botman SL, Moore TF, Moriarity CL, Parsons VL. Design and estimation for the National Health Interview Survey, 1995–2004 [PDF 300 KB]. National Center for Health Statistics. Vital Health Stat 2(130). 2000.
- SUDAAN, release 9.1 [computer software]. Research Triangle Park, NC: RTI International. 2004.
- Joinpoint Regression Program, version 3.4 [computer software]. Bethesda, MD: National Cancer Institute, National Institutes of Health. 2010.
Suggested citation
Akinbami LJ, Liu X, Pastor PN, Reuben CA. Attention deficit hyperactivity disorder among children aged 5–17 years in the United States, 1998–2009. NCHS data brief, no 70. Hyattsville, MD: National Center for Health Statistics. 2011.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Edward J. Sondik, Ph.D., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Office of Analysis and Epidemiology
Linda T. Bilheimer, Ph.D., Director