The Changing Profile of Autopsied Deaths in the United States, 1972–2007
- Key findings
- Autopsy rates declined more than 50 percent from 1972 through 2007.
- Deaths due to external causes were more likely to be determined by autopsy than deaths due to diseases or ill-defined conditions.
- Autopsy rates declined with increasing age after ages 15–24.
- The cause-of-death distribution of autopsied deaths has changed over time.
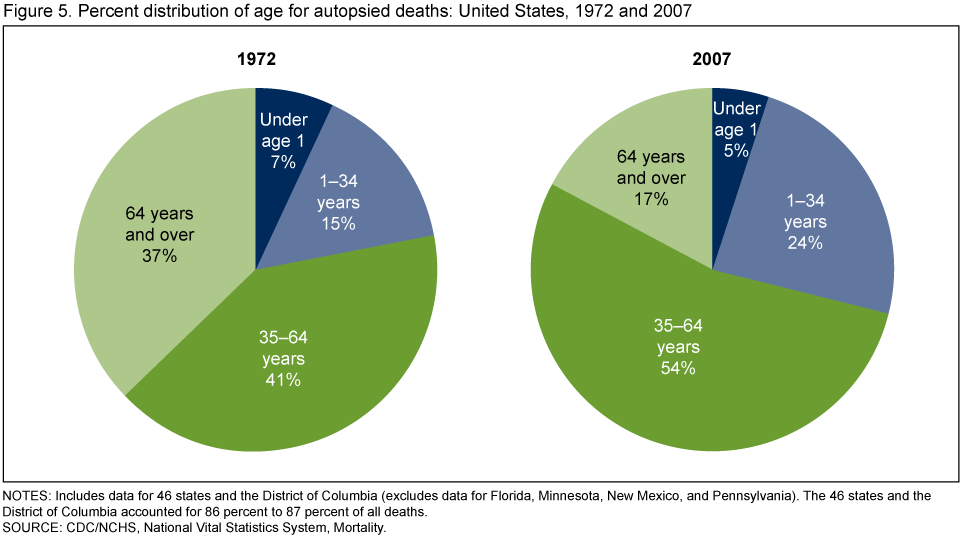
- The age distribution of autopsied deaths has changed over time.
- Summary
- Definitions
- Data source and methods
- About the author
- References
- Suggested citation
NCHS Data Brief No. 67, August 2011
PDF Version (642 KB)
Donna L. Hoyert, Ph.D.
Key findings
Data from the National Vital Statistics System, Mortality
- The percentage of deaths for which an autopsy was performed declined more than 50 percent from 1972 through 2007, from 19.3 percent to 8.5 percent.
- External causes accounted for 9 of the 10 most frequently autopsied causes of death.
- The percentage autopsied declined with age after ages 15–24: from 60 percent at 15–24, to 11 percent at 55–64, to less than 5 percent at 65–74.
- In 1972, 79 percent of autopsies were performed for deaths due to disease conditions and 19 percent for deaths due to external causes. By 2007, the respective percentages were 46 percent and 50 percent.
- While the age distribution of deaths shifted to older ages from 1972 through 2007, autopsied deaths were increasingly concentrated in the age groups 1–34 and 35–64.
An autopsy, the medical examination of a deceased person, may confirm clinical findings, provide more complete information to describe cause of death, or uncover conditions not recognized clinically prior to death (1). Two types are performed in the United States: a) hospital or clinical autopsies, which family or physicians request to clarify cause of death or assess care, and b) medicolegal autopsies, which legal officials order to further investigate the circumstances surrounding a death (2). The autopsy rate, or percentage of deaths that received this final assessment, was stable from the 1950s until the beginning of the 1970s, when the autopsy rate began to decrease (3). This report uses mortality data from the National Vital Statistics System (NVSS) over a 35-year period to examine changes in the autopsy rate and in the distribution of those autopsied by age and cause. Variation in autopsy patterns has implications for which deaths may have a more complete and conclusive cause-of-death determination.
Keywords: autopsy, autopsy rate, cause of death, National Vital Statistics System
Autopsy rates declined more than 50 percent from 1972 through 2007.
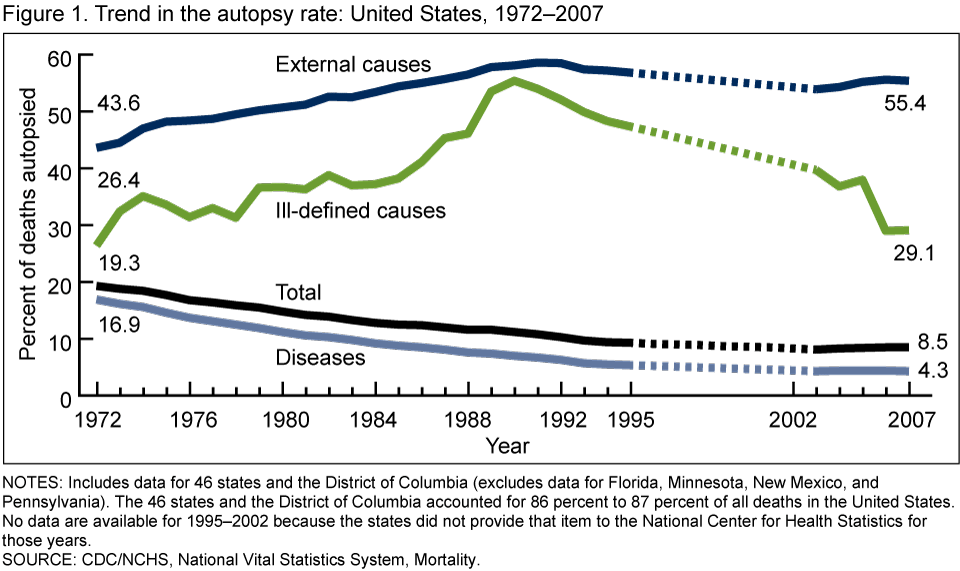
In 1972, almost 1 out of 5 deaths were autopsied. From 1972 through 2003, however, the autopsy rate dropped 58 percent from 19.3 percent to 8.1 percent. Although the autopsy rate has increased slightly since 2003, only 8.5 percent, or fewer than 1 out of 10 deaths, were autopsied in 2007 (Figure 1).
The autopsy rate can also be examined with respect to the cause of death: whether death was due to a disease such as heart disease or cancer; an external cause such as unintentional injury, homicide, or suicide; or an ill-defined condition such as unknown cause or sudden infant death syndrome (SIDS). Autopsies either confirm or alter the original cause-of-death determination.
From 1972 through 2007 autopsy rates declined for deaths from disease conditions from 16.9 percent to 4.3 percent and generally increased from 43.6 percent to 55.4 percent for deaths from external causes. The rates for deaths from ill-defined conditions were 26.4 percent in 1972 and 29.1 percent in 2007; however, this was variable over time.
Deaths due to external causes were more likely to be determined by autopsy than deaths due to diseases or ill-defined conditions.
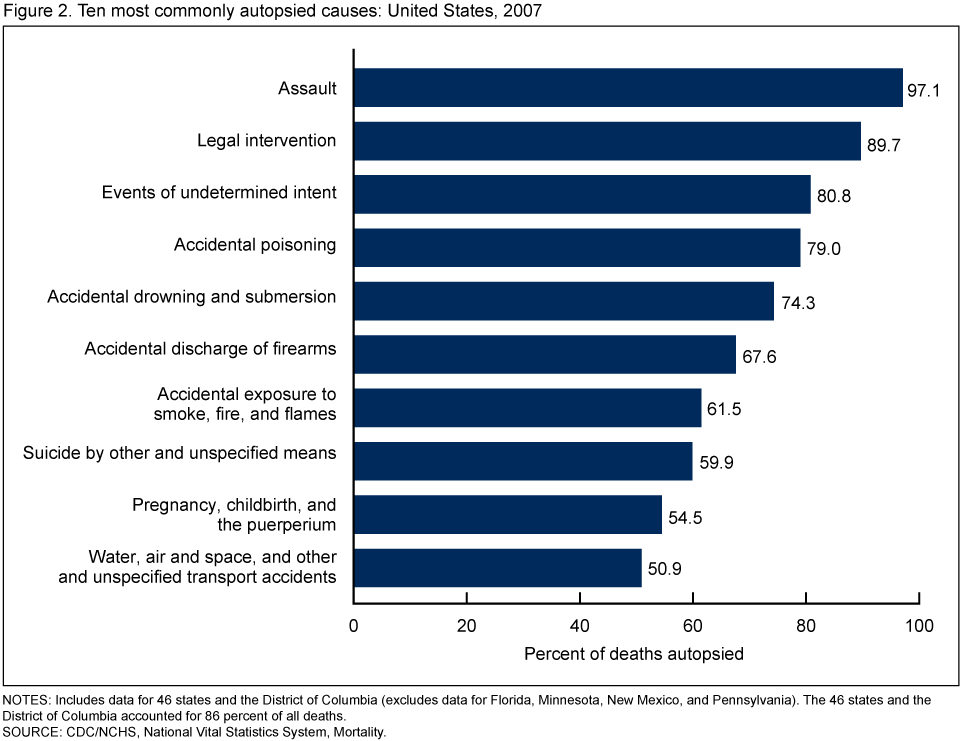
Although 91 percent of deaths in the United States in 2007 were due to a disease condition, these were less likely to be autopsied than deaths due to external causes (Figure 2). Deaths due to complications of pregnancy, childbirth, and the puerperium was the only disease condition among the 10 causes of death most often autopsied. Slightly more than one-half of deaths due to complications of pregnancy, childbirth, and puerperium were autopsied in 2007. Of the external causes of death, the highest percentages autopsied in 2007 were 97.1 percent for assault (homicide) deaths, 89.7 percent for legal intervention deaths, and 80.8 percent for events of undetermined intent.
Autopsy rates declined with increasing age after ages 15–24.
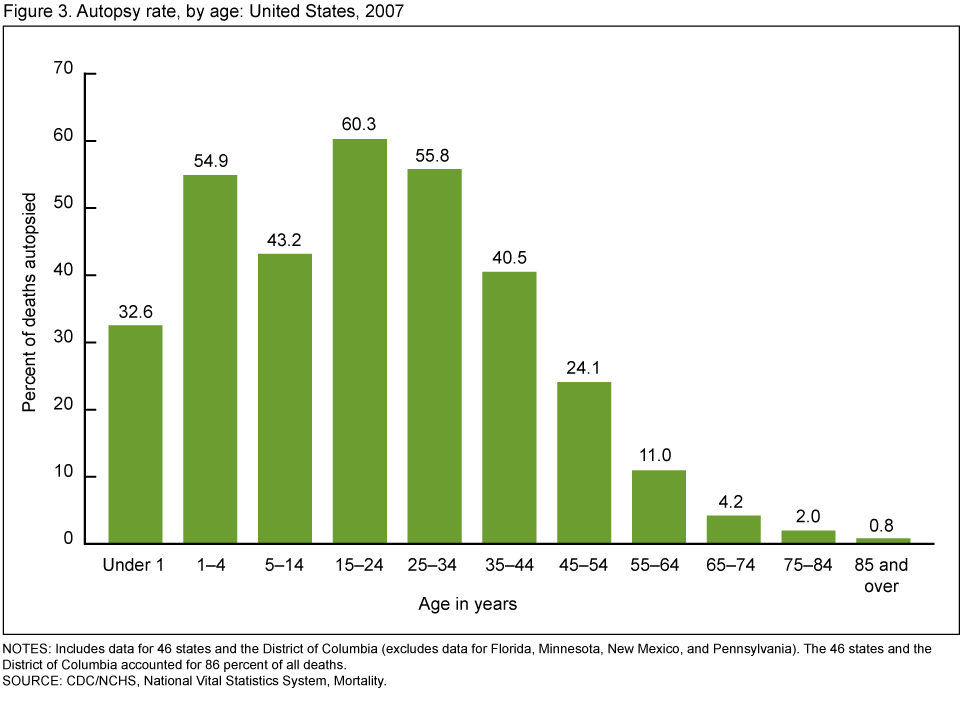
Although the number of deaths increased with age after age 1, autopsy rates declined in 2007 after ages 15–24. The percentage of deaths autopsied was highest for those deaths at ages 15–24 (60.3 percent), falling to 55.8 percent of deaths autopsied at ages 25–34. By age 65, only 4.2 percent of deaths were autopsied and less than 1 percent of deaths to persons aged 85 and over were autopsied (Figure 3).
Disease conditions were more likely to be the cause of death for older persons in contrast to external causes, which were more likely to be the cause of death at earlier ages. Ill-defined conditions were also likely to be the cause of death for older persons, but were also not uncommon among infants (e.g., SIDS).
The cause-of-death distribution of autopsied deaths has changed over time.
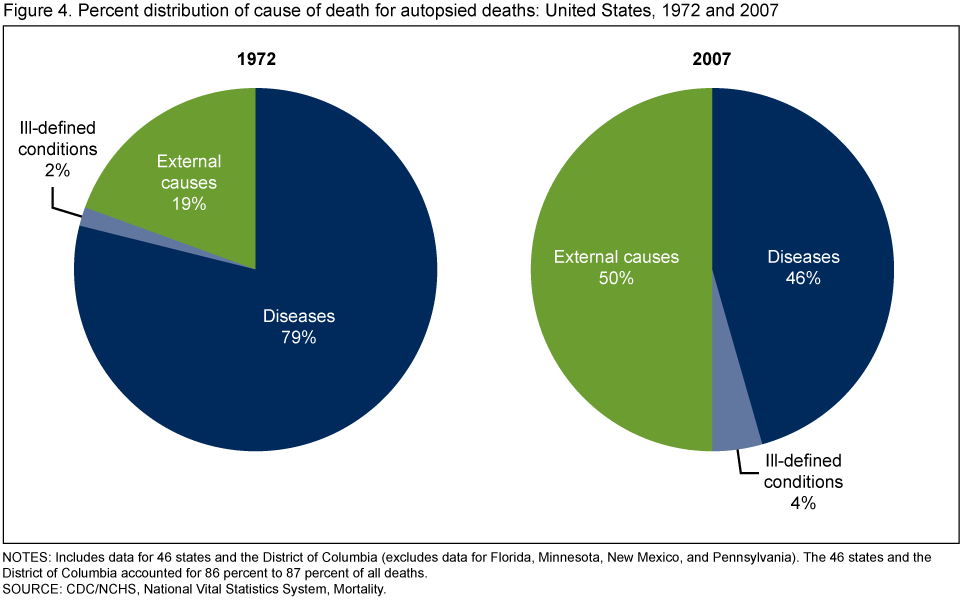
Cause-of-death distributions were similar in 1972 and 2007, with approximately 91 percent of all deaths due to diseases, 8 percent due to external causes, and 1 percent caused by ill-defined conditions. The distribution of autopsied deaths, however, changed substantially (Figure 4). While in 1972, 79 percent of autopsied deaths were deaths caused by disease conditions, in 2007 only 46 percent of autopsied deaths were due to disease conditions. In contrast, 50 percent of autopsied deaths in 2007 were external cause deaths compared with 19 percent in 1972. Ill-defined conditions accounted for 2 percent of autopsied deaths in 1972 and 4 percent in 2007.
The age distribution of autopsied deaths has changed over time.
From 1972 through 2007, the age distribution of all deaths shifted to older ages, so that more deaths were concentrated among persons aged 65 and over. For example, 63 percent of deaths occurred to persons aged 65 and over in 1972 compared with 72 percent in 2007. In contrast, autopsied deaths have become increasingly concentrated among decedents in the age groups 1–34 and 35–64 during this period (Figure 5). As a result, the age distribution of autopsied deaths was very different than for deaths in general in 1972 and was even more so in 2007. For example, while only 23 percent of all deaths in 2007 were to persons aged 35–64, 54 percent of those autopsied were from this age group.
Summary
Potential influences on the autopsy rate over the 1972–2007 period include hospital accreditation standards, state laws and regulations about which deaths should be investigated, and sudden and unexplained infant death protocols (2–5). The laws and regulations about investigations of deaths have changed little over time, although protocols for sudden and unexplained infant deaths that address autopsy practices have been developed since 1972 (6). However, in 1971 the Joint Commission on Accreditation of Hospitals dropped a hospital accreditation standard requiring a 20 percent to 25 percent autopsy rate for deaths occurring in hospitals (3). Findings that shifts in autopsy patterns result in an increasing percentage of autopsies among external cause deaths and persons under age 65 from 1972 through 2007 are consistent with declining trends in hospital autopsies and stable or increasing trends for medicolegal autopsies (2). With fewer autopsies being done on persons with characteristics typical of most deaths, cause-of-death determinations for important disease conditions or for deaths to those over age 65 are based on diagnoses and examinations prior to death and are not reviewed or confirmed by autopsy.
Definitions
Autopsy: Refers to an examination after death for medical, legal, or scientific reasons such as to establish medical conditions and the reason for death occurring when it did (1,2).
Autopsy rate: Refers to the number of deaths receiving an autopsy per all deaths, expressed per 100 deaths.
Hospital autopsy: Refers to an autopsy often performed at a hospital after being requested by family or medical personnel for reasons such as education, quality assessment, and establishing a cause of death (2,5).
Medicolegal autopsy: Refers to an autopsy often performed at a medical examiner’s office upon the order of a legal authority to determine the causes and circumstances of death for sudden, unexpected, unexplained, unattended, or nondisease deaths (2,5).
Data source and methods
Data presented in this report were based on information from death certificates filed in states and the District of Columbia and subsequently compiled into national data, also known as the NVSS, by the Centers for Disease Control and Prevention’s (CDC) National Center for Health Statistics (NCHS) for years 1972–1994 and 2003–2007 (7). Autopsy data were not available in the national data for the period 1995–2002 because, as agreed to by NCHS and the states, the item was not among those that the states provided to NCHS for those years. The item was restored to the national data in 2003 but not all 50 states and the District of Columbia provided the data to NCHS every year for the period 2003–2007. In order to compare the same states throughout the time period, data for 46 states and the District of Columbia were used and data for Florida, Minnesota, New Mexico, and Pennsylvania were excluded from this analysis. The 46 states and the District of Columbia accounted for 86 percent to 87 percent of all deaths in the United States from 1972 through 2007.
About the author
Donna L. Hoyert is with the CDC’s NCHS, Division of Vital Statistics, Mortality Statistics Branch.
References
- Hanzlick R. Case of the month: Wrapping things up. Arch Intern Med 160(20):3029–31. 2000.
- Wood MJ, Guha AK. Declining clinical autopsy rates versus increasing medicolegal autopsy rates in Halifax, Nova Scotia. Arch Pathol Lab Med 125(7):924–30. 2001.
- Hoyert DL, Kung HC, Xu J. Autopsy patterns in 2003. National Center for Health Statistics. Vital Health Stat 20(32). 2007.
- Scordi-Bello IA, Kalb TH, Lento PA. Clinical setting and extent of premortem evaluation do not predict autopsy discrepancy rates. Mod Pathol 23(9):1225–30. 2010.
- Godwin TA. End of life: Natural or unnatural death investigation and certification. Dis Mon 51(4):218–77. 2005.
- Centers for Disease Control and Prevention. Sudden unexpected infant death and sudden infant death syndrome. [Accessed 3/25/11].
- Xu JQ, Kochanek KD, Murphy SL, Tejada-Vera B. Deaths: Final data for 2007. National vital statistics reports; vol 58 no 19. Hyattsville, MD: National Center for Health Statistics. 2010.
Suggested citation
Hoyert DL. The changing profile of autopsied deaths in the United States, 1972–2007. NCHS data brief, no 67. Hyattsville, MD: National Center for Health Statistics. 2011.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Edward J. Sondik, Ph.D., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Vital Statistics
Charles J. Rothwell, M.S., Director