Drug Overdose Deaths in the United States, 2003–2023
NCHS Data Brief No. 522, December 2024
PDF Version (527 KB)
Matthew F. Garnett, M.P.H., and Arialdi M. Miniño, M.P.H.
- Key findings
- The overall age-adjusted rate of drug overdose deaths decreased 4.0% between 2022 and 2023.
- The rate of drug overdose deaths decreased among young and middle-aged adults from 2022 to 2023.
- Between 2022 and 2023, rates of drug overdose deaths increased for Black non-Hispanic and Native Hawaiian or Other Pacific Islander non-Hispanic people.
- After a period of increase between 2013 and 2022, rates of drug overdose deaths involving synthetic opioids other than methadone, which includes fentanyl, fentanyl analogs, and tramadol, decreased between 2022 and 2023.
Data from the National Vital Statistics System
- The age-adjusted rate of drug overdose deaths increased from 8.9 deaths per 100,000 standard population in 2003 to 32.6 in 2022; however, the rate decreased to 31.3 in 2023.
- Rates decreased between 2022 and 2023 for people ages 15–54 and increased for adults age 55 and older.
- From 2022 to 2023, rates decreased for White non-Hispanic people, while rates for other race and Hispanic-origin groups generally stayed the same or increased.
- Between 2022 and 2023, rates declined for deaths involving synthetic opioids other than methadone, heroin, and natural and semisynthetic opioids, while the rate for methadone remained the same.
- From 2022 to 2023, rates increased for deaths involving cocaine by 4.9% (from 8.2 to 8.6) and psychostimulants with abuse potential by 1.9% (10.4 to 10.6).
Drug overdoses are one of the leading causes of injury death in adults and have risen over the past several decades in the United States (1–3). Overdoses involving synthetic opioids (fentanyl, for example) and stimulants (cocaine and methamphetamine, for example) have also risen in the past few years (1). This report presents rates of drug overdose deaths from the National Vital Statistics System over a 20-year period by demographic group and by the type of drugs involved, specifically, opioids and stimulants, with a focus on changes from 2022 to 2023.
Keywords: opioids, heroin, cocaine, methamphetamine, National Vital Statistics System, Mortality
The overall age-adjusted rate of drug overdose deaths decreased 4.0% between 2022 and 2023.
- In 2023, 105,007 drug overdose deaths occurred, resulting in an age-adjusted rate of 31.3 deaths per 100,000 standard population (Figure 1, Table 1).
- After the age-adjusted rate of drug overdose deaths nearly quadrupled from 8.9 in 2003 to 32.6 in 2022, the rate decreased to 31.3 in 2023.
- From 2022 to 2023, the age-adjusted rate of drug overdose deaths for males decreased 2.9% from 45.6 to 44.3, while the rate for females decreased 5.7% from 19.4 to 18.3.
Figure 1. Age-adjusted drug overdose death rate, by sex: United States, 2003–2023
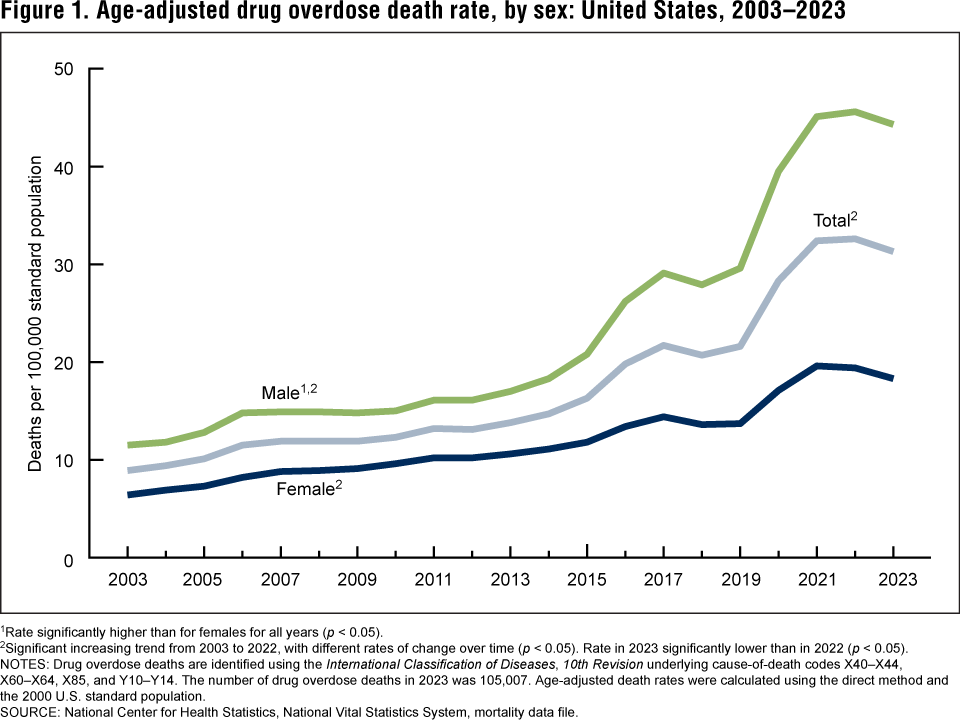
1Rate significantly higher than for females for all years (p < 0.05).
2Significant increasing trend from 2003 to 2022, with different rates of change over time (p < 0.05). Rate in 2023 significantly lower than in 2022 (p < 0.05).
NOTES: Drug overdose deaths are identified using the International Classification of Diseases, 10th Revision underlying cause-of-death codes X40–X44, X60–X64, X85, and Y10–Y14. The number of drug overdose deaths in 2023 was 105,007. Age-adjusted death rates were calculated using the direct method and the 2000 U.S. standard population.
SOURCE: National Center for Health Statistics, National Vital Statistics System, mortality data file.
The rate of drug overdose deaths decreased among young and middle-aged adults from 2022 to 2023.
- From 2022 to 2023, the rate of drug overdose deaths decreased among people ages 15–24 (from 15.1 deaths per 100,000 to 13.5), 25–34 (50.6 to 45.6), 35–44 (63.1 to 60.8), and 45–54 (55.3 to 53.3) (Figure 2, Table 2).
- Between 2022 and 2023, the rate of drug overdose deaths increased among adults ages 55–64 (from 48.1 to 49.2) and 65 and older (13.2 to 14.7).
- In both 2022 and 2023, the rate of drug overdose deaths was highest for adults ages 35–44. In 2022, the rate was lowest for adults age 65 and older, but in 2023 the rate was lowest for people ages 15–24.
- From 2022 to 2023, adults age 65 and older experienced the largest percentage increase in the rate of drug overdose deaths (11.4%), and the largest decrease was for people ages 15–24 (10.6%).
Figure 2. Drug overdose death rate, by selected age group: United States, 2022 and 2023
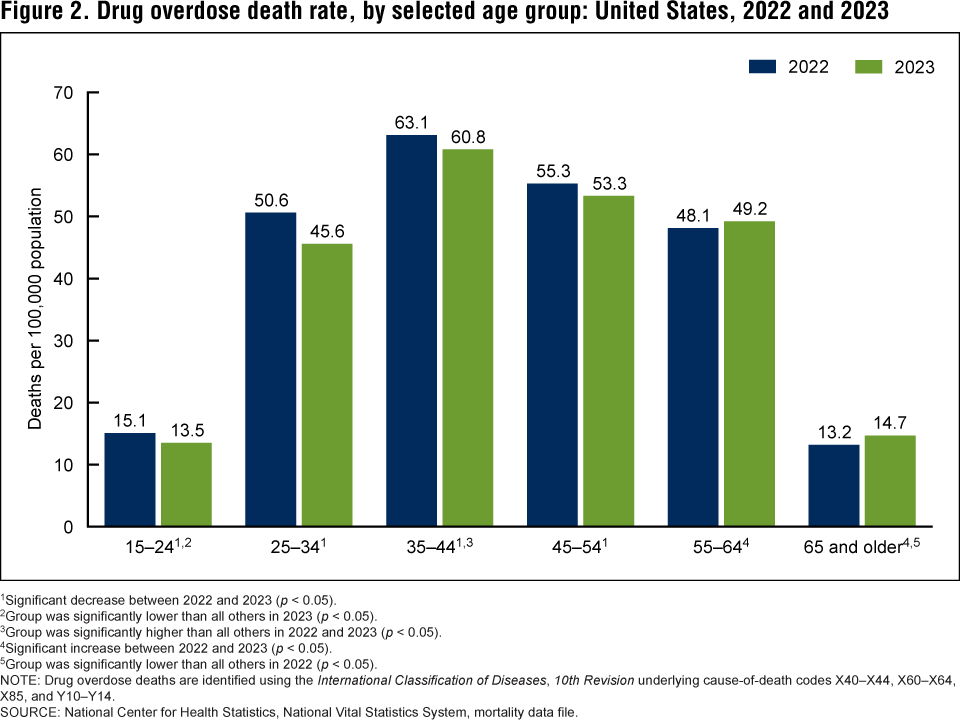
1Significant decrease between 2022 and 2023 (p < 0.05).
2Group was significantly lower than all others in 2023 (p < 0.05).
3Group was significantly higher than all others in 2022 and 2023 (p < 0.05).
4Significant increase between 2022 and 2023 (p < 0.05).
5Group was significantly lower than all others in 2022 (p < 0.05).
NOTE: Drug overdose deaths are identified using the International Classification of Diseases, 10th Revision underlying cause-of-death codes X40–X44, X60–X64, X85, and Y10–Y14.
SOURCE: National Center for Health Statistics, National Vital Statistics System, mortality data file.
Between 2022 and 2023, rates of drug overdose deaths increased for Black non-Hispanic and Native Hawaiian or Other Pacific Islander non-Hispanic people.
- For White non-Hispanic (subsequently, White) people, the age-adjusted rate of drug overdose deaths was lower in 2023 than in 2022, decreasing by 7.0% from 35.6 deaths per 100,000 standard population to 33.1 (Figure 3, Table 3). Drug overdose death rates increased for Black non-Hispanic (subsequently, Black) people (47.5 to 48.9) and Native Hawaiian or Other Pacific Islander non-Hispanic (subsequently, Native Hawaiian or Other Pacific Islander) people (18.8 to 26.2) from 2022 to 2023.
- From 2022 to 2023, the age-adjusted rate of drug overdose deaths did not significantly change for Asian non-Hispanic (subsequently, Asian) people (5.3 to 5.1), Hispanic people (22.7 to 22.8), and American Indian and Alaska Native non-Hispanic (subsequently, American Indian and Alaska Native) people (65.2 to 65.0).
- In both 2022 and 2023, the age-adjusted rate of drug overdose deaths was highest for American Indian and Alaska Native people (65.2 and 65.0, respectively), and lowest for Asian people (5.3 and 5.1, respectively).
- Native Hawaiian or Other Pacific Islander people experienced the largest percentage increase in the age-adjusted rate of drug overdose deaths from 2022 to 2023, with the rate increasing 39.4%.
Figure 3. Age-adjusted drug overdose death rate, by race and Hispanic origin: United States, 2022 and 2023
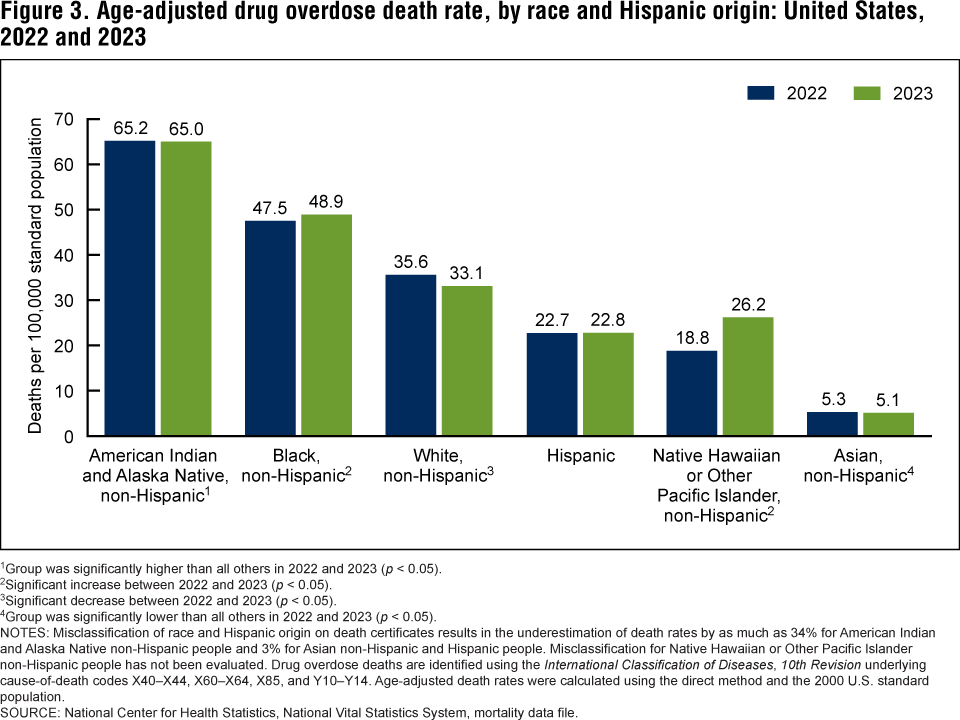
1Group was significantly higher than all others in 2022 and 2023 (p < 0.05).
2Significant increase between 2022 and 2023 (p < 0.05).
3Significant decrease between 2022 and 2023 (p < 0.05).
4Group was significantly lower than all others in 2022 and 2023 (p < 0.05).
NOTES: Misclassification of race and Hispanic origin on death certificates results in the underestimation of death rates by as much as 34% for American Indian and Alaska Native non-Hispanic people and 3% for Asian non-Hispanic and Hispanic people. Misclassification for Native Hawaiian or Other Pacific Islander non-Hispanic people has not been evaluated. Drug overdose deaths are identified using the International Classification of Diseases, 10th Revision underlying cause-of-death codes X40–X44, X60–X64, X85, and Y10–Y14. Age-adjusted death rates were calculated using the direct method and the 2000 U.S. standard population.
SOURCE: National Center for Health Statistics, National Vital Statistics System, mortality data file.
After a period of increase between 2013 and 2022, rates of drug overdose deaths involving synthetic opioids other than methadone, which includes fentanyl, fentanyl analogs, and tramadol, decreased between 2022 and 2023.
- The age-adjusted rate of drug overdose deaths involving synthetic opioids other than methadone, which includes fentanyl, fentanyl analogs, and tramadol, was mostly stable from 2003 (0.5 deaths per 100,000 standard population) to 2013 (1.0) and then increased through 2021 (21.8), with different rates of change over time (Figure 4, Table 4). From 2022 to 2023, the rate decreased by 2.2% from 22.7 to 22.2.
- After increasing from 2003 to 2006 and decreasing from 2006 to 2017, the age-adjusted rate of drug overdose deaths involving methadone remained stable through 2023.
- After no significant change from 2020 to 2021, the age-adjusted rate of drug overdose deaths involving natural and semisynthetic opioids, which includes drugs such as morphine, oxycodone, and hydrocodone, decreased 17.1% from 3.5 in 2022 to 2.9 in 2023.
- The age-adjusted rate of drug overdose deaths involving heroin decreased 33.3% from 1.8 in 2022 to 1.2 in 2023.
Figure 4. Age-adjusted rate of drug overdose deaths involving opioids, by type of opioid: United States, 2003–2023
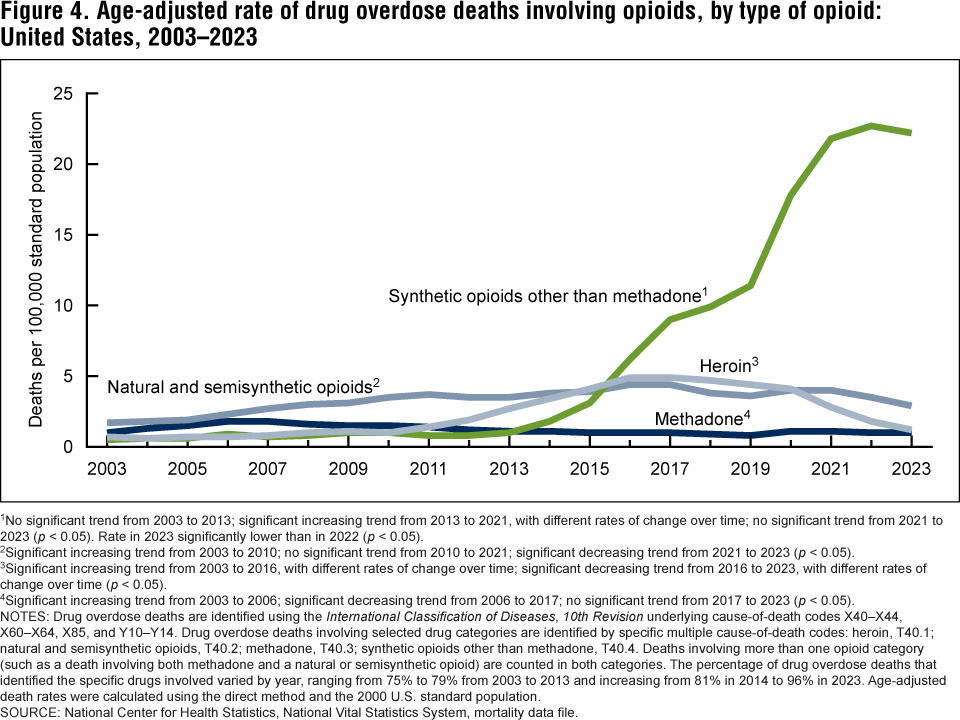
1No significant trend from 2003 to 2013; significant increasing trend from 2013 to 2021, with different rates of change over time; no significant trend from 2021 to 2023 (p < 0.05). Rate in 2023 significantly lower than in 2022 (p < 0.05).
2Significant increasing trend from 2003 to 2010; no significant trend from 2010 to 2021; significant decreasing trend from 2021 to 2023 (p < 0.05).
3Significant increasing trend from 2003 to 2016, with different rates of change over time; significant decreasing trend from 2016 to 2023, with different rates of change over time (p < 0.05).
4Significant increasing trend from 2003 to 2006; significant decreasing trend from 2006 to 2017; no significant trend from 2017 to 2023 (p < 0.05).
NOTES: Drug overdose deaths are identified using the International Classification of Diseases, 10th Revision underlying cause-of-death codes X40–X44, X60–X64, X85, and Y10–Y14. Drug overdose deaths involving selected drug categories are identified by specific multiple cause-of-death codes: heroin, T40.1; natural and semisynthetic opioids, T40.2; methadone, T40.3; synthetic opioids other than methadone, T40.4. Deaths involving more than one opioid category (such as a death involving both methadone and a natural or semisynthetic opioid) are counted in both categories. The percentage of drug overdose deaths that identified the specific drugs involved varied by year, ranging from 75% to 79% from 2003 to 2013 and increasing from 81% in 2014 to 96% in 2023. Age-adjusted death rates were calculated using the direct method and the 2000 U.S. standard population.
SOURCE: National Center for Health Statistics, National Vital Statistics System, mortality data file.
The increases in age-adjusted rates of drug overdose deaths involving cocaine and psychostimulants with abuse potential that began around 2011 have continued through 2023.
- The age-adjusted rate of drug overdose deaths involving cocaine increased slightly from 1.8 deaths per 100,000 standard population in 2003 to 2.5 in 2006, decreased to 1.3 in 2010, and then increased to 8.6 in 2023; the rate in 2023 was 4.9% higher than the rate in 2022 (8.2) (Figure 5, Table 5).
- The age-adjusted rate of drug overdose deaths involving psychostimulants with abuse potential (subsequently, psychostimulants), which includes methamphetamine, amphetamine, and methylphenidate, was stable between 2003 (0.4) and 2010 (0.6), after which it increased through 2021 (10.0), with different rates of change over time. The rate in 2023 (10.6) was 1.9% higher than the rate in 2022 (10.4).
Figure 5. Age-adjusted rate of drug overdose deaths involving stimulants, by type of stimulant: United States, 2003–2023
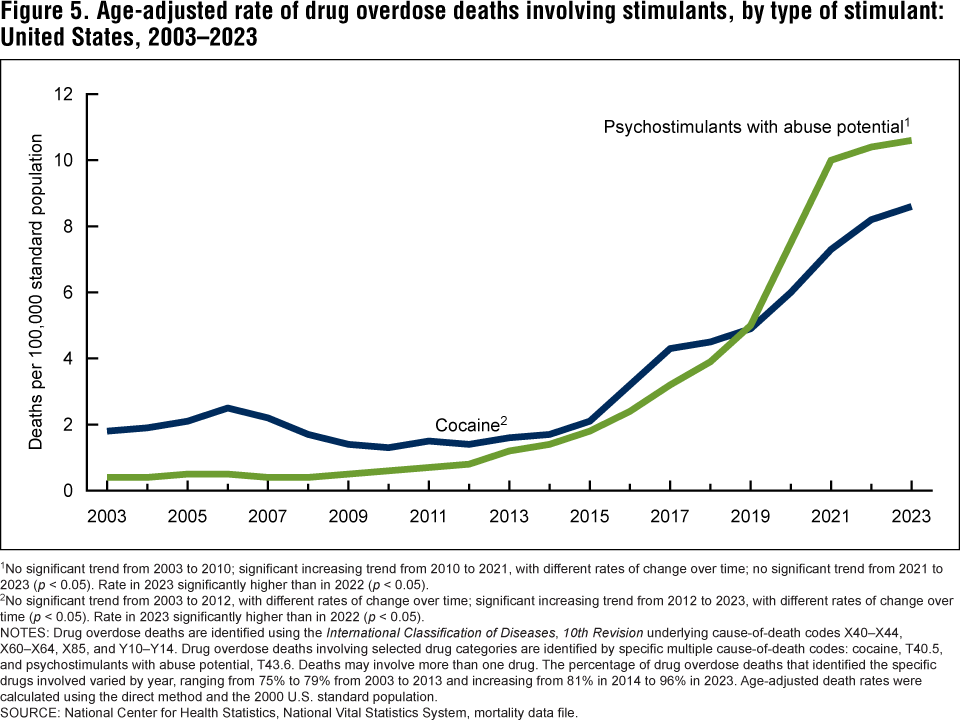
1No significant trend from 2003 to 2010; significant increasing trend from 2010 to 2021, with different rates of change over time; no significant trend from 2021 to 2023 (p < 0.05). Rate in 2023 significantly higher than in 2022 (p < 0.05).
2No significant trend from 2003 to 2012, with different rates of change over time; significant increasing trend from 2012 to 2023, with different rates of change over time (p < 0.05). Rate in 2023 significantly higher than in 2022 (p < 0.05).
NOTES: Drug overdose deaths are identified using the International Classification of Diseases, 10th Revision underlying cause-of-death codes X40–X44, X60–X64, X85, and Y10–Y14. Drug overdose deaths involving selected drug categories are identified by specific multiple cause-of-death codes: cocaine, T40.5, and psychostimulants with abuse potential, T43.6. Deaths may involve more than one drug. The percentage of drug overdose deaths that identified the specific drugs involved varied by year, ranging from 75% to 79% from 2003 to 2013 and increasing from 81% in 2014 to 96% in 2023. Age-adjusted death rates were calculated using the direct method and the 2000 U.S. standard population.
SOURCE: National Center for Health Statistics, National Vital Statistics System, mortality data file.
Summary
The age-adjusted rate of drug overdose deaths declined 4.0% between 2022 and 2023, which follows a nonsignificant increase between 2021 and 2022 (1). Previously, rates had generally increased across most years over the period 2003–2023.
From 2022 to 2023, the age-adjusted rate of drug overdose decreased 2.9% for males and 5.7% for females. In both 2022 and 2023, adults ages 35–44 had the highest rate among people age 15 and older. The age group with the lowest rates changed from 2022 to 2023, with adults age 65 and older having the lowest rates in 2022 and people ages 15–24 having the lowest rates in 2023. This was due to an increase in the rate for adults age 65 and older and a decrease in the rate for people ages 15–24. Between 2022 and 2023, rates of drug overdose deaths decreased for people ages 15–54 and increased for adults age 55 and older.
In both 2022 and 2023, the age-adjusted rate of drug overdose deaths was highest for American Indian and Alaska Native people and lowest among Asian people. Despite decreases in the overall rate, the rate only significantly decreased for White people. Rate changes for American Indian and Alaska Native, Asian, and Hispanic people were not significant, and rates significantly increased for Black and Native Hawaiian or Other Pacific Islander people.
The age-adjusted rate for drug overdose deaths involving synthetic opioids other than methadone decreased from 2022 to 2023, the first such decrease since the large increases that began in 2013. The rate also decreased for deaths involving natural and semisynthetic opioids and heroin between 2022 and 2023. For the same period, rates increased for drug overdose deaths involving psychostimulants and cocaine, and rates stayed the same for deaths involving methadone.
Definitions
Drug poisoning (overdose) deaths: Includes deaths resulting from unintentional or intentional overdose of a drug, being given the wrong drug, taking a drug in error, or taking a drug inadvertently.
Natural and semisynthetic opioids: Includes drugs such as morphine, codeine, hydrocodone, and oxycodone.
Psychostimulants with abuse potential: Includes drugs such as methamphetamine, amphetamine, and methylphenidate.
Synthetic opioids other than methadone: Includes drugs such as fentanyl, fentanyl analogs, and tramadol.
Data source and methods
Estimates are based on the National Vital Statistics System multiple cause-of-death mortality files (3). Drug poisoning (overdose) deaths were defined as having an International Classification of Diseases, 10th Revision underlying cause-of-death code of X40–X44 (unintentional), X60–X64 (suicide), X85 (homicide), or Y10–Y14 (undetermined intent). Of the drug overdose deaths in 2023, 92.6% were unintentional, 4.4% were suicides, 2.8% were of undetermined intent, and less than 1.0% were homicides. The type of drug(s) involved was indicated by International Classification of Diseases, 10th Revision multiple cause-of-death codes: T40.1 (heroin), T40.2 (natural and semisynthetic opioids), T40.3 (methadone), T40.4 (synthetic opioids other than methadone), T40.5 (cocaine), and T43.6 (psychostimulants with abuse potential).
Age-adjusted death rates were calculated using the direct method and adjusted to the 2000 U.S. standard population (4). Population estimates for 2021–2023 were estimated as of July 1, based on the blended base produced by the U.S. Census Bureau instead of the April 1, 2020, decennial population count. The blended base consists of the blend of vintage 2020 postcensal population estimates based on the 2010 population census, 2020 demographic analysis estimates, and the 2020 decennial census total counts (see https://www2.census.gov/programs-surveys/popest/technical-documentation/methodology/2020-2021/methods-statement-v2021.pdf and https://www2.census.gov/programs-surveys/popest/technical-documentation/methodology/2020-2023/methods-statement-v2023.pdf). Population data are July 1 postcensal census estimates.
Race and Hispanic origin were categorized based on the 1997 Office of Management and Budget standards for federal statistical and administrative reporting (5). All of the race categories are single race, meaning that only one race was reported on the death certificate. Data shown for the Hispanic population include people of any race. Death rates for Asian, American Indian and Alaska Native, and Hispanic people are affected by misclassification of race and Hispanic origin on death certificates (6). This misclassification results in underestimation of death rates for these groups by about 3% for Asian and Hispanic people and by about 34% for American Indian and Alaska Native people (7). Misclassification for Native Hawaiian or Other Pacific Islander people has not been evaluated. The extent of misclassification has not been evaluated by cause of death for all race and Hispanic-origin groups. As a result, rates of drug overdose deaths presented in this report are not adjusted for race and Hispanic-origin misclassification on death certificates.
Trends in age-adjusted death rates were evaluated using the Joinpoint Regression Program (Version 5.0.2) (8). Joinpoint software fitted weighted least-squares regression models to the rates on the log-transform scale. The permutation tests for model (number of joinpoints) significance were set at an overall alpha level of 0.05 (8,9). Pairwise comparisons of rates (for example, age-adjusted rates for males compared with females and year-to-year comparisons) were conducted using the z test with an alpha level of 0.05 (9).
Several factors related to death investigation and reporting may affect measurement of death rates involving specific drugs. At autopsy, the substances tested for and the circumstances under which the toxicology tests are performed vary by jurisdiction. This variability is more likely to affect substance-specific death rates than the overall drug overdose death rate. The percentage of drug overdose deaths that identified the specific drugs involved varied by year, ranging from 75% to 79% from 2003 to 2013, and increasing from 81% in 2014 to 96% in 2023. Additionally, drug overdose deaths may involve multiple drugs; therefore, a death might be included in more than one category when describing the rate of drug overdose deaths involving specific drugs. For example, a death that involved both fentanyl and cocaine would be included in both the rate of drug overdose deaths involving synthetic opioids other than methadone and the rate of drug overdose deaths involving cocaine.
About the author
The authors are with the National Center for Health Statistics: Matthew F. Garnett is with the Division of Analysis and Epidemiology and Arialdi M. Miniño is with the Division of Vital Statistics.
References
- Spencer MR, Garnett MF, Miniño AM. Drug overdose deaths in the United States, 2002–2022. NCHS Data Brief, no 491. Hyattsville, MD: National Center for Health Statistics. 2024. DOI: https://dx.doi.org/10.15620/cdc:135849.
- National Center for Injury Prevention and Control. WISQARS—Web-based Injury Statistics Query and Reporting System. 2023.
- National Center for Health Statistics. Mortality multiple cause files. 2023.
- Kochanek KD, Murphy SL, Xu JQ, Arias E. Deaths: Final data for 2020. National Vital Statistics Reports; vol 72 no 10. Hyattsville, MD: National Center for Health Statistics. 2023. DOI: https://dx.doi.org/10.15620/cdc:131355.
- Office of Management and Budget. Revisions to the standards for the classification of federal data on race and ethnicity. Fed Regist 62(210):58782–90. 1997.
- Arias E, Heron M, Hakes JK. The validity of race and Hispanic-origin reporting on death certificates in the United States: An update. National Center for Health Statistics. Vital Health Stat 2(172). 2016.
- Arias E, Xu JQ, Curtin S, Bastian B, Tejada-Vera B. Mortality profile of the non-Hispanic American Indian or Alaska Native population, 2019. National Vital Statistics Reports; vol 70 no 12. Hyattsville, MD: National Center for Health Statistics. 2021. DOI: https://dx.doi.org/10.15620/cdc:110370.
- National Cancer Institute. Joinpoint Regression Program (Version 5.0.2) [computer software]. 2023.
- Ingram DD, Malec DJ, Makuc DM, Kruszon-Moran D, Gindi RM, Albert M, et al. National Center for Health Statistics guidelines for analysis of trends. National Center for Health Statistics. Vital Health Stat 2(179). 2018.
Suggested citation
Garnett MF, Miniño AM. Drug overdose deaths in the United States, 2003–2023. NCHS Data Brief, no 522. Hyattsville, MD: National Center for Health Statistics. 2024. DOI: https://dx.doi.org/10.15620/cdc/170565.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Brian C. Moyer, Ph.D., Director
Amy M. Branum, Ph.D., Associate Director for Science
Division of Analysis and Epidemiology
Irma E. Arispe, Ph.D., Director
Kimberly A. Lochner, Sc.D., Associate Director for Science
Division of Vital Statistics
Paul D. Sutton, Ph.D., Acting Director
Andrés A. Berruti, Ph.D., M.A., Associate Director for Science