Emergency Department Visits With an Influenza Test Ordered or Provided: United States, 2013-2022
NCHS Data Brief No. 517, December 2024
PDF Version (454 KB)
Susan M. Schappert, M.A., and Loredana Santo, M.D., M.P.H.
- Key findings
- Did the percentage of ED visits with an influenza test ordered or provided increase between 2013 and 2022?
- Did the percentage of ED visits with an influenza test ordered or provided differ by age group between 2013 and 2022?
- Which reasons for the ED visit had the highest percentage of influenza tests ordered or provided, and did these percentages change between 2013 and 2022?
- Did the percentage of ED visits with an influenza test ordered or provided increase by geographic region between 2013 and 2022?
Data from the National Hospital Ambulatory Medical Care Survey
- The percentage of annual emergency department (ED) visits with an influenza test ordered or provided increased from 2.5% in 2013 to 10.9% in 2022.
- ED visits by children ages 0–5 years had the highest percentage of influenza tests ordered or provided in 2013 (8.6%) and 2022 (23.1%).
- Fever and cough were the most frequent first-listed reasons for ED visits with an influenza test ordered or provided in both 2013 and 2022.
- Percentages of ED visits with an influenza test ordered or provided increased for each geographic region of the United States (Northeast, Midwest, South, and West) between 2013 and 2022.
Influenza, also known as flu, is a viral respiratory infection. Preliminary data from the Centers for Disease Control and Prevention for the 2022–2023 influenza season suggest that 31 million people developed influenza, 360,000 were hospitalized with influenza, and 21,000 died from influenza (1). To prevent more serious illness, early identification and treatment of influenza is important (2). This report uses data from the National Hospital Ambulatory Medical Care Survey (NHAMCS) to study trends in the use of influenza testing at hospital emergency department (ED) visits during 2013–2022.
Keywords: flu, diagnostic test, respiratory illness, National Hospital Ambulatory Medical Care Survey
Did the percentage of ED visits with an influenza test ordered or provided increase between 2013 and 2022?
- In 2013, 2.5% of ED visits included an influenza test documented in the medical record as either ordered or provided. This percentage increased to 10.9% in 2022 (Figure 1, Table 1).
Figure 1. Percentage of emergency department visits with an influenza test ordered or provided: United States, 2013–2022
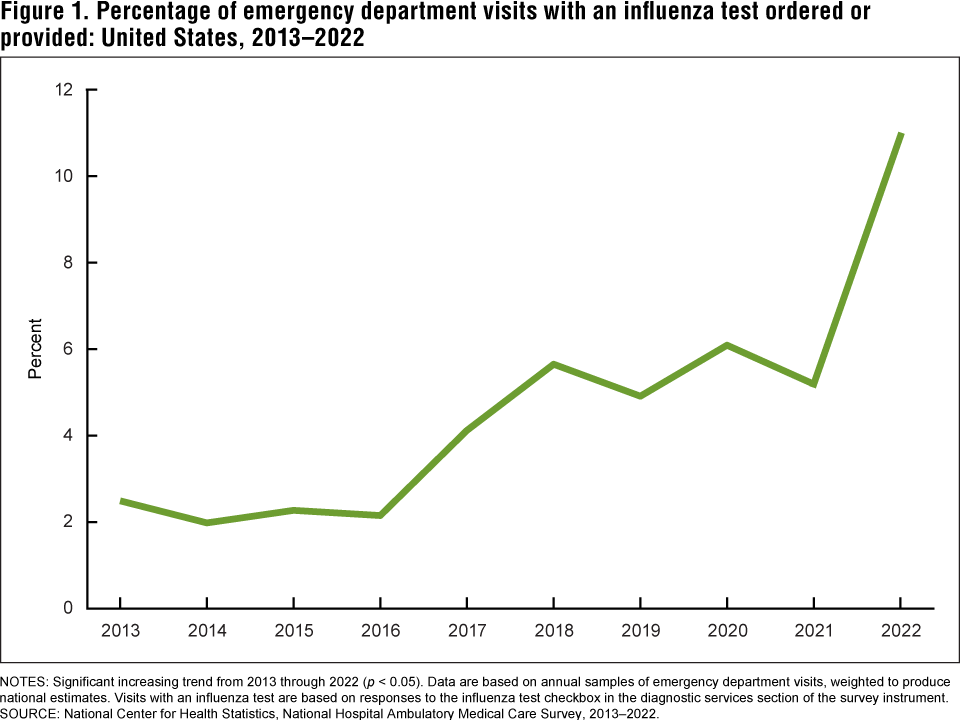
NOTES: Significant increasing trend from 2013 through 2022 (p < 0.05). Data are based on annual samples of emergency department visits, weighted to produce national estimates. Visits with an influenza test are based on responses to the influenza test checkbox in the diagnostic services section of the survey instrument.
SOURCE: National Center for Health Statistics, National Hospital Ambulatory Medical Care Survey, 2013–2022.
Did the percentage of ED visits with an influenza test ordered or provided differ by age group between 2013 and 2022?
- The percentage of ED visits with an influenza test ordered or provided increased from 8.6% of visits by infants and children ages 0–5 years in 2013 to 23.1% in 2022 (Figure 2, Table 2).
- This pattern of a higher percentage of visits with influenza tests ordered or provided in 2022 was consistent for all age groups. Among ED visits by children ages 6–17, the percentage with an influenza test increased from 2.6% in 2013 to 13.4% in 2022. Among ED visits by adults, the percentage with an influenza test increased from 1.9% to 9.1% for ages 18–44, from 1.3% to 8.7% for ages 45–64, and from 1.5% to 9.6% for age 65 and older.
- The percentage of ED visits with an influenza test ordered or provided was highest for infants and children ages 0–5 years compared with all other age groups in both 2013 and 2022.
Figure 2. Percentage of emergency department visits with an influenza test ordered or provided, by patient age group: United States, 2013 and 2022
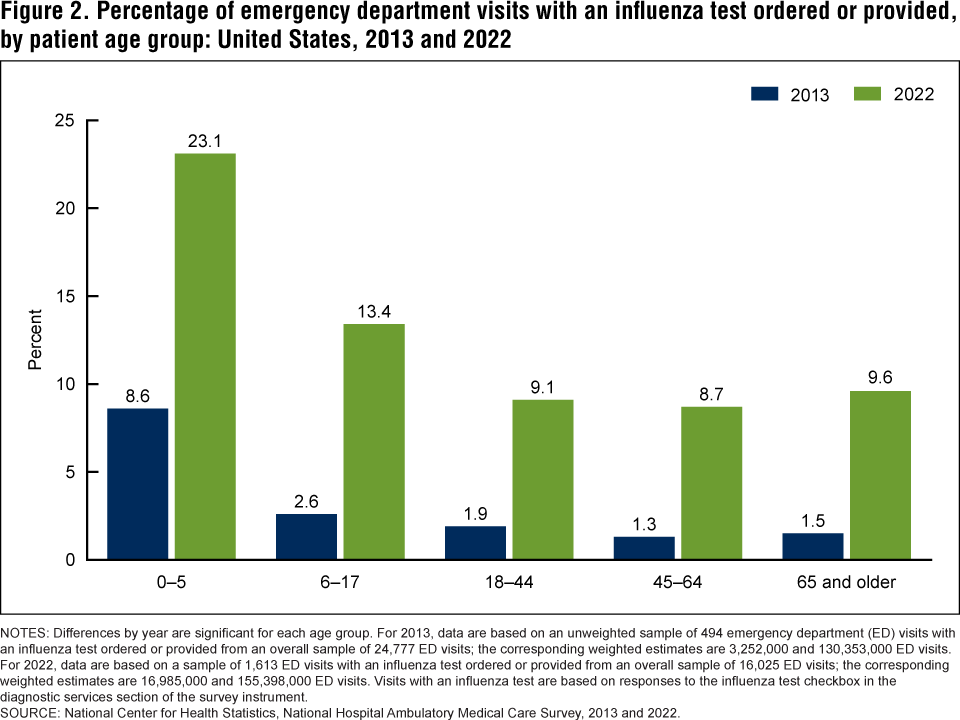
NOTES: Differences by year are significant for each age group. For 2013, data are based on an unweighted sample of 494 emergency department (ED) visits with an influenza test ordered or provided from an overall sample of 24,777 ED visits; the corresponding weighted estimates are 3,252,000 and 130,353,000 ED visits. For 2022, data are based on a sample of 1,613 ED visits with an influenza test ordered or provided from an overall sample of 16,025 ED visits; the corresponding weighted estimates are 16,985,000 and 155,398,000 ED visits. Visits with an influenza test are based on responses to the influenza test checkbox in the diagnostic services section of the survey instrument.
SOURCE: National Center for Health Statistics, National Hospital Ambulatory Medical Care Survey, 2013 and 2022.
Which reasons for the ED visit had the highest percentage of influenza tests ordered or provided, and did these percentages change between 2013 and 2022?
-
The percentages of ED visits with an influenza test ordered or provided increased for most selected first-listed reasons for visit (Figure 3, Table 3).
-
An influenza test was ordered or provided at 16.8% of ED visits with a first-listed reason of fever in 2013; this increased to 38.5% of visits in 2022. Similarly, the percentage of ED visits with a first-listed reason of cough with an influenza test ordered or provided increased from 13.3% in 2013 to 35.8% in 2022.
-
Nausea (22.6%), shortness of breath (19.6%), and psychological symptoms (16.7%) were also among the first-listed reasons for visit with an influenza test ordered or provided in 2022. These percentages were significantly higher than corresponding percentages in 2013 for nausea (2.2%) and shortness of breath (3.1%). Visits for psychological symptoms in 2013 did not include any influenza testing.
Figure 3. Percentage of emergency department visits with an influenza test ordered or provided, by selected first-listed reason for visit: United States, 2013 and 2022
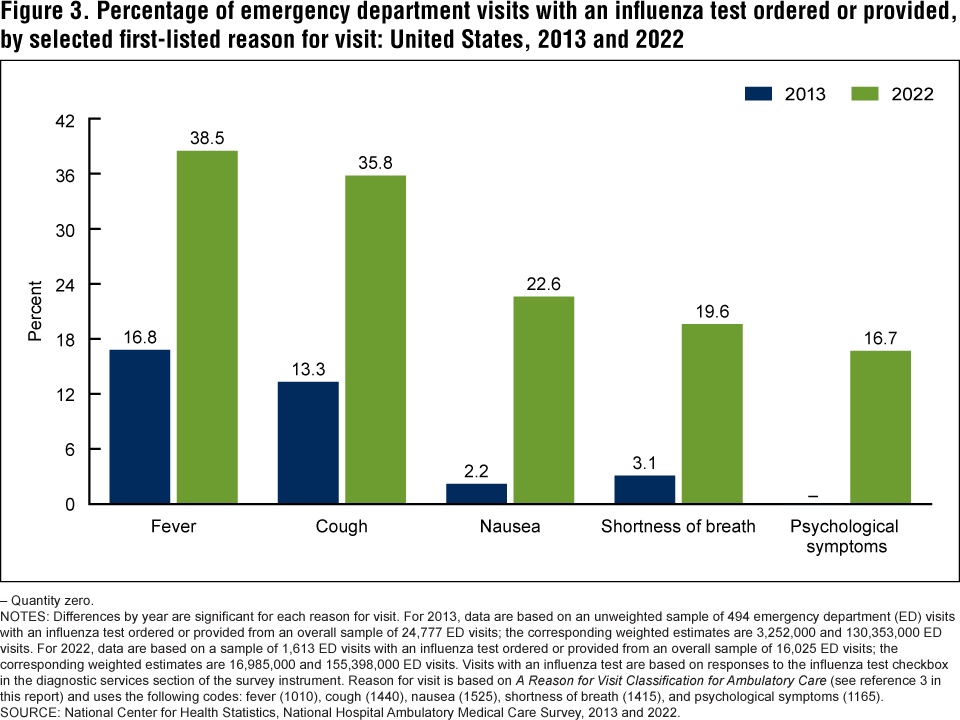
– Quantity zero.
NOTES: Differences by year are significant for each reason for visit. For 2013, data are based on an unweighted sample of 494 emergency department (ED) visits with an influenza test ordered or provided from an overall sample of 24,777 ED visits; the corresponding weighted estimates are 3,252,000 and 130,353,000 ED visits. For 2022, data are based on a sample of 1,613 ED visits with an influenza test ordered or provided from an overall sample of 16,025 ED visits; the corresponding weighted estimates are 16,985,000 and 155,398,000 ED visits. Visits with an influenza test are based on responses to the influenza test checkbox in the diagnostic services section of the survey instrument. Reason for visit is based on A Reason for Visit Classification for Ambulatory Care (see reference 3 in this report) and uses the following codes: fever (1010), cough (1440), nausea (1525), shortness of breath (1415), and psychological symptoms (1165).
SOURCE: National Center for Health Statistics, National Hospital Ambulatory Medical Care Survey, 2013 and 2022.
Did the percentage of ED visits with an influenza test ordered or provided increase by geographic region between 2013 and 2022?
- The percentages of ED visits with an influenza test ordered or provided increased in each of the four geographic regions of the United States between 2013 and 2022 (Figure 4, Table 4).
- In the Northeast, the percentage of ED visits with an influenza test ordered or provided increased from 1.6% to 12.9%, and in the Midwest the percentage increased from 0.4% to 8.4%. In the South, the percentage of ED visits with an influenza test ordered or provided increased from 5.0% to 11.4%, and in the West the percentage increased from 1.0% to 11.1%.
Figure 4. Percentage of emergency department visits with an influenza test ordered or provided, by geographic region: United States, 2013 and 2022
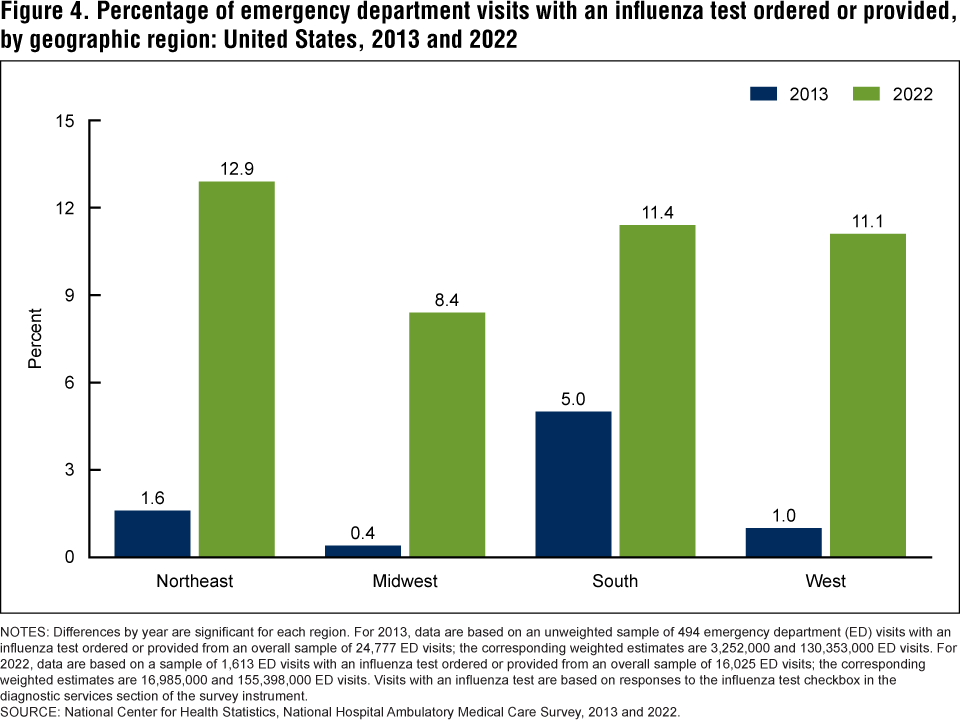
NOTES: Differences by year are significant for each region. For 2013, data are based on an unweighted sample of 494 emergency department (ED) visits with an influenza test ordered or provided from an overall sample of 24,777 ED visits; the corresponding weighted estimates are 3,252,000 and 130,353,000 ED visits. For 2022, data are based on a sample of 1,613 ED visits with an influenza test ordered or provided from an overall sample of 16,025 ED visits; the corresponding weighted estimates are 16,985,000 and 155,398,000 ED visits. Visits with an influenza test are based on responses to the influenza test checkbox in the diagnostic services section of the survey instrument.
SOURCE: National Center for Health Statistics, National Hospital Ambulatory Medical Care Survey, 2013 and 2022.
Summary
During 2013–2022, the percentage of ED visits with an influenza test ordered or provided increased significantly from 2.5% in 2013 to 10.9% in 2022. Visits by infants and children ages 0–5 years had the highest percentages of such visits in both years. The percentage of ED visits made by this age group increased significantly between 2013 and 2022, as did the percentages for all other age groups. ED visits with either fever or cough as the first-listed reason for visit had the highest percentages of influenza testing in both years. Visits with a first-listed reason of nausea, shortness of breath, or psychological symptoms also had relatively high percentages of influenza testing in 2022; the percentages for nausea and shortness of breath were significantly higher than the corresponding percentages in 2013. Visits with a first-listed reason of psychological symptoms did not have influenza testing reported in 2013. In each of the four geographic regions of the United States, the percentage of ED visits with an influenza test ordered or provided increased significantly from 2013 to 2022.
Definitions
Influenza test ordered or provided: For each year of NHAMCS from 2013–2022, a section on diagnostic and screening services was included. This section included a list of about 45 checkboxes for various services under the headings of laboratory tests, other tests, and imaging. In 2022, an additional section for COVID-19 tests was added. The checkbox for influenza test was included in the “other tests” section. NHAMCS data collection agents were instructed to review the patient’s medical record and check all services that were either ordered or provided during the sampled ED visit. Visits with “influenza test” checked were selected for inclusion in this report.
Reason for visit: Patients’ medical records were reviewed by NHAMCS data collection agents and up to five reasons for making the sampled ED visit were recorded. Verbatim text was used to describe the patient’s (or patient’s surrogate’s) expressed symptom, complaint, or other reason for making the ED visit. The first-listed reason is the most important reason related to the current visit. These text entries were later coded by National Center for Health Statistics (NCHS) medical coders using A Reason for Visit Classification for Ambulatory Care developed by NCHS for use with NHAMCS data (3). Reason for visit codes used in this report are as follows: fever (1010), cough (1440), nausea (1525), shortness of breath (1415), and psychological symptoms (1165). Psychological symptoms most often reflected verbatim entries of altered mental states, including disorientation, confusion, and lethargy.
Data source and methods
This report analyzed data from NHAMCS, a nationally representative annual survey of nonfederal general and short-stay hospitals in the United States. NHAMCS uses a multistage probability design with samples of geographic primary sampling units, hospitals within primary sampling units, and patient visits within EDs. Analyses for this report were conducted using data from restricted-use data files. Public-use versions of these files are available from: https://www.cdc.gov/nchs/nhamcs/documentation/index.html. Count estimates and measures of variance could differ between the restricted-use and public-use files. Information for accessing the restricted-use data file is available from: https://www.cdc.gov/rdc/. Additional information on NHAMCS’s methodology is available online (4–13). This report presents results for the 2013–2022 survey years.
Data analyses were performed using the statistical packages SAS version 9.4 (SAS Institute, Cary, N.C.) and SAS-callable SUDAAN version 11.0 (RTI International, Research Triangle Park, N.C.). Differences among groups were evaluated using two-sided significance tests at the p < 0.05 level. To test for linear and quadratic trends over time, the null hypothesis of nonlinear or quadratic trend was examined using the POLY option in SUDAAN. If a quadratic trend was significant, Joinpoint software (14) was used to determine the change point in the trend line. Linear regression was used to test the significance of slope according to NCHS trend analysis guidelines (15). All estimates meet NCHS presentation standards for proportions unless otherwise noted (16).
About the authors
Susan M. Schappert and Loredana Santo are with the National Center for Health Statistics, Division of Health Care Statistics.
References
- Centers for Disease Control and Prevention. Preliminary estimated flu disease burden 2022–2023 flu season. 2024.
- Centers for Disease Control and Prevention. Testing and respiratory viruses.
- Schneider D. A reason for visit classification for ambulatory care. Vital and Health Statistics Series 2(78). National Center for Health Statistics: Hyattsville, MD. 1979.
- National Center for Health Statistics. 2013 NHAMCS micro-data file documentation. 2015.
- National Center for Health Statistics. 2014 NHAMCS micro-data file documentation. 2016.
- National Center for Health Statistics. 2015 NHAMCS micro-data file documentation. 2017.
- National Center for Health Statistics. 2016 NHAMCS micro-data file documentation. 2018.
- National Center for Health Statistics. 2017 NHAMCS micro-data file documentation. 2019.
- National Center for Health Statistics. 2018 NHAMCS micro-data file documentation. 2020.
- National Center for Health Statistics. 2019 NHAMCS micro-data file documentation. 2021.
- National Center for Health Statistics. 2020 NHAMCS micro-data file documentation. 2022.
- National Center for Health Statistics. 2021 NHAMCS micro-data file documentation. 2023.
- National Center for Health Statistics. 2022 NHAMCS micro-data file documentation. 2024.
- National Cancer Institute. Joinpoint Regression Program (Version 4.6.0) [computer software]. 2019.
- Ingram DD, Malec DJ, Makuc DM, Kruszon-Moran D, Gindi RM, Albert M, et al. National Center for Health Statistics guidelines for analysis of trends. National Center for Health Statistics. Vital Health Stat 2(179). 2018.
- Parker JD, Talih M, Malec DJ, Beresovsky V, Carroll M, Gonzalez JF Jr, et al. National Center for Health Statistics data presentation standards for proportions. National Center for Health Statistics. Vital Health Stat 2(175). 2017.
Suggested citation
Schappert SM, Santo L. Emergency department visits with an influenza test ordered or provided: United States, 2013–2022. NCHS Data Brief, no 517. Hyattsville, MD: National Center for Health Statistics. DOI: https://dx.doi.org/10.15620/cdc/168516.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Brian C. Moyer, Ph.D., Director
Amy M. Branum, Ph.D., Associate Director for Science
Division of Health Care Statistics
Carol J. DeFrances, Ph.D., Director
Alexander Strashny, Ph.D., Associate Director for Science