Dental Care Among Adults Aged 65 and Over, 2017
- Key findings
- What percentage of the population aged 65 and over had dental insurance, and did this vary by characteristics?
- Did the percentage of the population aged 65 and over who had a dental visit in the past 12 months vary by characteristics?
- Did the percentage of the population aged 65 and over who had unmet need for dental care due to cost in the past 12 months vary by characteristics?
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 337, May 2019
PDF Version (481 KB)
Ellen A. Kramarow, Ph.D.
Key findings
Data from the National Health Interview Survey
- In 2017, slightly less than one-third (29.2%) of adults aged 65 and over had dental insurance. The percentage with dental insurance was higher among those aged 65–74 (34.3%) compared with older age groups, and lower among Hispanic adults (17.5%) compared with other race and Hispanic-origin groups.
- Overall, approximately two-thirds of adults aged 65 and over had a dental visit in the past 12 months. Older adults who were poor (42.7%) or near poor (42.8%) were less likely to have had a dental visit compared with not-poor (74.4%) older adults.
- Non-Hispanic black (11.2%) and Hispanic (12.3%) adults aged 65 and over were more likely to have unmet need for dental care due to cost compared with non-Hispanic white (6.8%) and non-Hispanic Asian (5.9%) older adults.
Dental care is often an overlooked aspect of overall health care among older adults. Regular dental care is recommended for all older adults, even those with full dentures (1). Because Medicare does not cover routine dental care, older adults may have trouble accessing appropriate dental care (2). This report describes the prevalence, overall and by selected characteristics, of dental insurance, dental visits, and unmet need for dental care due to cost among adults aged 65 and over.
Keywords: dental insurance, dental visits, unmet need, National Health Interview Survey
What percentage of the population aged 65 and over had dental insurance, and did this vary by characteristics?
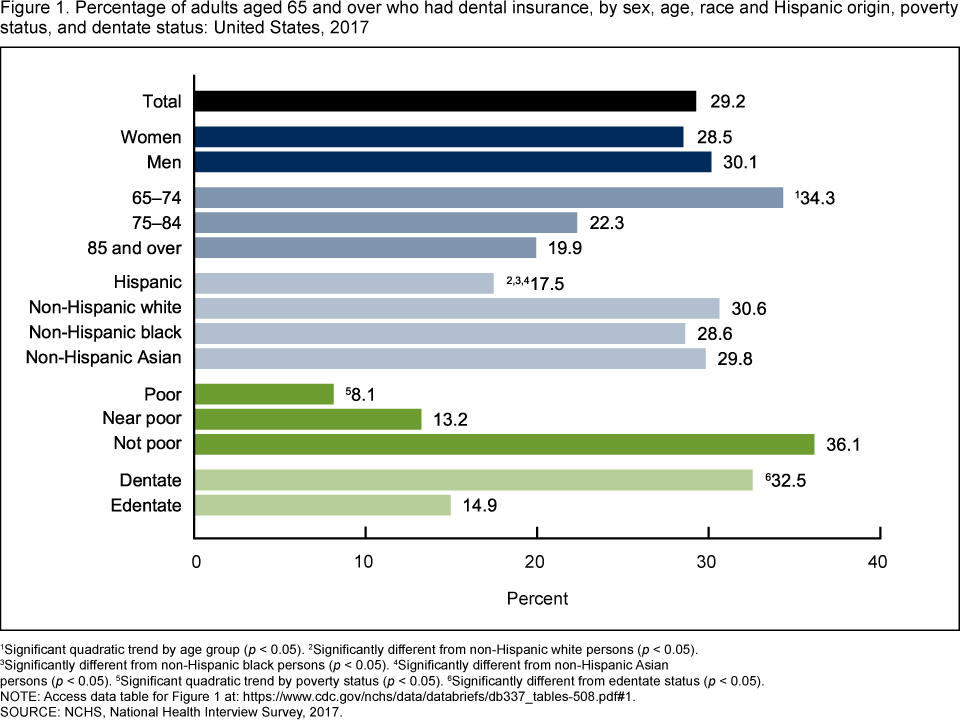
- In 2017, among adults aged 65 and over, 29.2% had dental insurance (Figure 1).
- The percentage of adults who had dental insurance was higher among those aged 65–74 (34.3%) compared with those aged 75–84 (22.3%) and 85 and over (19.9%).
- Hispanic adults aged 65 and over were less likely to have dental insurance (17.5%) than non-Hispanic white (30.6%), non-Hispanic black (28.6%), and non-Hispanic Asian (29.8%) adults.
- Adults aged 65 and over who were not poor were more likely to have dental insurance (36.1%) compared with those who were near poor (13.2%) and poor (8.1%).
- Edentate older adults (those who had lost all of their natural teeth) were less likely to have dental insurance compared with dentate older adults (14.9% compared with 32.5%).
Figure 1. Percentage of adults aged 65 and over who had dental insurance, by sex, age, race and Hispanic origin, poverty status, and dentate status: United States, 2017
1Significant quadratic trend by age group (p < 0.05).
2Significantly different from non-Hispanic white persons (p < 0.05).
3Significantly different from non-Hispanic black persons (p < 0.05).
4Significantly different from non-Hispanic Asian persons (p < 0.05).
5Significant quadratic trend by poverty status (p < 0.05).
6Significantly different from edentate status (p < 0.05).
NOTE: Access data table for Figure 1.
SOURCE: NCHS, National Health Interview Survey, 2017.
Did the percentage of the population aged 65 and over who had a dental visit in the past 12 months vary by characteristics?
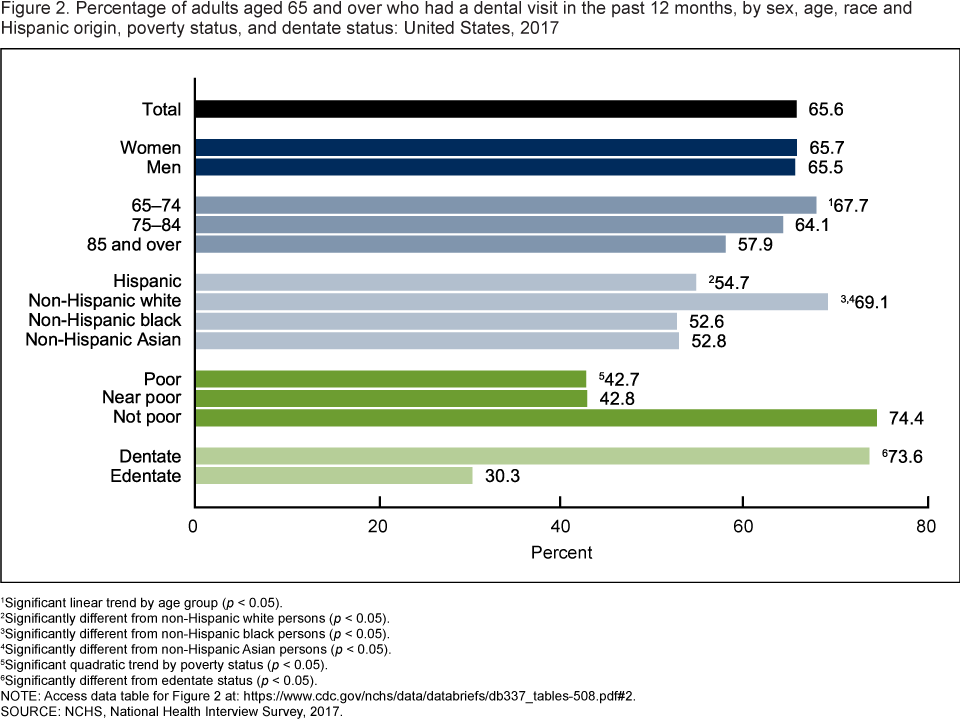
- In 2017, among adults aged 65 and over, 65.6% had a dental visit in the past 12 months (Figure 2).
- The percentage of adults aged 65 and over who had a dental visit in the past 12 months decreased with age, from 67.7% among adults aged 65–74 to 64.1% among those aged 75–84 to 57.9% among those aged 85 and over.
- Non-Hispanic white adults aged 65 and over were more likely to have had a dental visit in the past year (69.1%) compared with Hispanic (54.7%), non-Hispanic black (52.6%), and non-Hispanic Asian (52.8%) adults.
- Poor and near-poor older adults were less likely to have had a dental visit in the past year (42.7% and 42.8%, respectively) compared with adults who were not poor (74.4%).
- Edentate adults aged 65 and over were less likely (30.3%) than dentate older adults (73.6%) to have had a dental visit in the past 12 months.
Figure 2. Percentage of adults aged 65 and over who had a dental visit in the past 12 months, by sex, age, race and Hispanic origin, poverty status, and dentate status: United States, 2017
1Significant linear trend by age group (p < 0.05).
2Significantly different from non-Hispanic white persons (p < 0.05).
3Significantly different from non-Hispanic black persons (p < 0.05).
4Significantly different from non-Hispanic Asian persons (p < 0.05).
5Significant quadratic trend by poverty status (p < 0.05).
6Significantly different from edentate status (p < 0.05).
NOTE: Access data table for Figure 2.
SOURCE: NCHS, National Health Interview Survey, 2017.
Did the percentage of the population aged 65 and over who had unmet need for dental care due to cost in the past 12 months vary by characteristics?
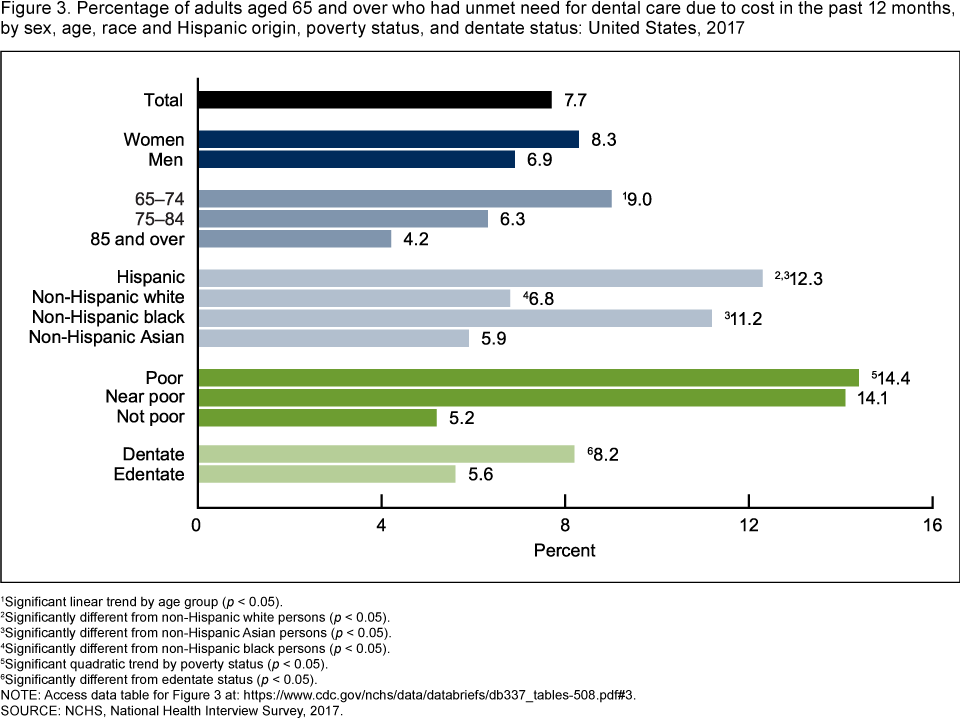
- In 2017, 7.7% of adults aged 65 and over needed dental care in the past 12 months but did not get it because of cost (Figure 3).
- The percentage of adults aged 65 and over who had unmet need for dental care due to cost decreased with age, from 9.0% among adults aged 65–74 to 6.3% among those aged 74–84 to 4.2% among those aged 85 and over.
- Hispanic and non-Hispanic black adults aged 65 and over were more likely to have unmet need for dental care due to cost (12.3% and 11.2%, respectively) compared with non-Hispanic white (6.8%) and non-Hispanic Asian (5.9%) adults.
- Poor and near-poor adults aged 65 and over were more likely to have unmet need for dental care due to cost (14.4% and 14.1%, respectively) compared with not-poor older adults (5.2%).
- Edentate older adults were less likely to have unmet need for dental care due to cost compared with dentate older adults (5.6% compared with 8.2%).
Figure 3. Percentage of adults aged 65 and over who had unmet need for dental care due to cost in the past 12 months, by sex, age, race and Hispanic origin, poverty status, and dentate status: United States, 2017
1Significant linear trend by age group (p < 0.05).
2Significantly different from non-Hispanic white persons (p < 0.05).
3Significantly different from non-Hispanic Asian persons (p < 0.05).
4Significantly different from non-Hispanic black persons (p < 0.05).
5Significant quadratic trend by poverty status (p < 0.05).
6Significantly different from edentate status (p < 0.05).
NOTE: Access data table for Figure 3.
SOURCE: NCHS, National Health Interview Survey, 2017.
Summary
In 2017, among adults aged 65 and over, 29.2% had dental insurance; 65.6% had a dental visit in the past 12 months; and 7.7% had an unmet need for dental care due to cost. No statistically significant differences by sex were observed in any of these dental care indicators. Adults aged 65–74 were more likely to have dental insurance, to have visited the dentist in the past 12 months, and to have unmet need for dental care due to cost compared with adults over age 75. Poor older adults were less likely to have dental insurance and to have visited the dentist, and more likely to have an unmet need for dental care due to cost compared with not-poor older adults. Edentate older adults were less likely to have had a dental visit in the past 12 months compared with dentate older adults.
Dental care is an important component of health care for the older population. Chronic diseases that may impact oral health and the need for care, such as diabetes and osteoporosis, are common among the older population, and poor oral health may contribute to the risk of certain conditions (1). Most adults aged 65 and over have access to health insurance through Medicare; however, Medicare does not cover routine dental care. The percentage of older adults with dental insurance is lower, in general, than the percentage with private insurance who have dental coverage among the population under 65 (3). Among older adults who qualify for both Medicare and Medicaid, some report dental coverage. Dental care covered through the Medicaid program varies by state (4) and may not be fully reflected in the estimates presented here.
Definitions
Dental insurance: Many older adults have private health insurance that supplements Medicare coverage. Dental insurance is estimated from questions on whether the respondent’s private health insurance plan covers dental care and whether the respondent has a single-service plan covering dental care. Respondents who answer yes to either of these questions are considered to have dental insurance. Respondents who report dental coverage through a Medicare Advantage plan are also considered to have dental insurance.
Dental visit in past 12 months: Estimates are based on responses to the question, “About how long has it been since you last saw or talked to a dentist? Include all types of dentists, such as orthodontists, oral surgeons, and all other dental specialists, as well as dental hygienists.” Responses of “6 months or less” and “more than 6 months, but not more than 1 year ago” were considered as having had a visit in the past 12 months.
Dentate or edentate status: The percentage with no natural teeth (edentate) is estimated from responses to the question, “Have you lost all of your upper and lower natural (permanent) teeth?”
Poverty status: Estimates are based on family income and family size using the U.S. Census Bureau’s poverty thresholds for the previous calendar year. “Poor” adults are defined as having incomes below the federal poverty level (FPL). “Near-poor” adults are defined as having family incomes that are 100% to less than 200% of the FPL. “Not-poor” adults are defined as having incomes that are 200% or greater than the FPL. The 2017 National Health Interview Survey (NHIS) imputed income files were used to help create the poverty variable, and this variable is based on reported and imputed family income (5).
Unmet need for dental care due to cost in past 12 months: Estimates are based on the question, “During the past 12 months, was there any time when you needed dental care (including checkups) but didn’t get it because you couldn’t afford it?”
Data source and methods
Data from the 2017 NHIS were used for this analysis. NHIS is a nationally representative, continuously fielded cross-sectional household interview survey from the National Center for Health Statistics (NCHS) that produces annual estimates of the health of the U.S. civilian noninstitutionalized population. Interviews are conducted in respondents’ homes, with follow-ups to complete interviews conducted by telephone if needed. Data for this analysis come from the Family Core and Sample Adult components of NHIS. For further information about NHIS, including the questionnaire, visit the NHIS website.
Analyses were conducted using SAS-callable SUDAAN version 11.0.3 (6), which accounts for the complex sample design of NHIS. All estimates for adults were weighted using the annual sample weights for adults. Data weighting procedures are described in more detail elsewhere (7). The Taylor series linearization method was chosen for estimation of standard errors. Trends in dental insurance, dental visit, and unmet need for dental care due to cost by age and poverty level were evaluated according to the guidelines specified in “National Center for Health Statistics Guidelines for Analysis of Trends” (8). Differences between percentages were evaluated using two-sided significance tests at the 0.05 level with no adjustments made for multiple comparisons. All estimates in this report meet NCHS standards of reliability as specified in “National Center for Health Statistics Data Presentation Standards for Proportions” (9).
About the author
Ellen A. Kramarow is with the National Center for Health Statistics, Office of Analysis and Epidemiology.
References
- The Gerontological Society of America. Oral health: An essential element of healthy aging. The Gerontological Society of America Newsletter. 2017.
- Raphael C. Oral health and aging. Am J Public Health 107(S1):S44–45. 2017.
- Bloom B, Cohen RA. Dental insurance for persons under age 65 years with private health insurance: United States, 2008. NCHS Data Brief, no 40. Hyattsville, MD: National Center for Health Statistics. 2010.
- Manski RJ, Moeller J, Schimmel J, St. Clair PA, Chen H, Magder L, Pepper JV. Dental care coverage and retirement. J Public Health Dent 70(1):1–12. 2010.
- National Center for Health Statistics. Multiple imputation of family income and personal earnings in the National Health Interview Survey: Methods and examples. 2018.
- RTI International. SUDAAN (Release 11.0.3) [computer software]. 2018.
- Parsons VL, Moriarity C, Jonas K, Moore TF, Davis KE, Tompkins L. Design and estimation for the National Health Interview Survey, 2006–2015. National Center for Health Statistics. Vital Health Stat 2(165). 2014.
- Ingram DD, Malec DJ, Makuc DM, Kruszon-Moran D, Gindi RM, Albert M, et al. National Center for Health Statistics Guidelines for Analysis of Trends. National Center for Health Statistics. Vital Health Stat 2(179). 2018.
- Parker JD, Talih M, Malec DJ, Beresovsky V, Carroll M, Gonzalez Jr JF, et al. National Center for Health Statistics Data Presentation Standards for Proportions. National Center for Health Statistics. Vital Health Stat 2(175). 2017.
Suggested citation
Kramarow EA. Dental care among adults aged 65 and over, 2017. NCHS Data Brief, no 337. Hyattsville, MD: National Center for Health Statistics. 2019.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Jennifer H. Madans, Ph.D., Acting Director
Amy M. Branum, Ph.D., Acting Associate Director for Science
Office of Analysis and Epidemiology
Irma E. Arispe, Ph.D., Director
Kevin C. Heslin, Ph.D., Associate Director for Science