CDC’s Drug Overdose Surveillance and Epidemiology (DOSE) System
DOSE data provide information on nonfatal drug overdoses
CDC’s Overdose Data to Action (OD2A) program supports the collection of data on nonfatal overdoses through the Drug Overdose Surveillance and Epidemiology (DOSE) system. Data reported to DOSE are captured by health departments and are used to describe nonfatal overdoses at the local, state, and national levels.
Provides timely data on nonfatal overdoses treated in emergency departments.
Identifies overdose anomalies or outbreaks and changes in trends.
Informs drug overdose response and prevention activities.
CDC’s DOSE system includes emergency department (ED) syndromic surveillance data and ED and inpatient hospitalization discharge data. DOSE syndromic surveillance data and DOSE ED and inpatient hospitalization discharge data provide complementary information to understand nonfatal drug overdose trends in the United States. In total, 48 jurisdictions participate in DOSE with 42 states and the District of Columbia submitting syndromic surveillance data and 25 states submitting discharge data (Figure 1).
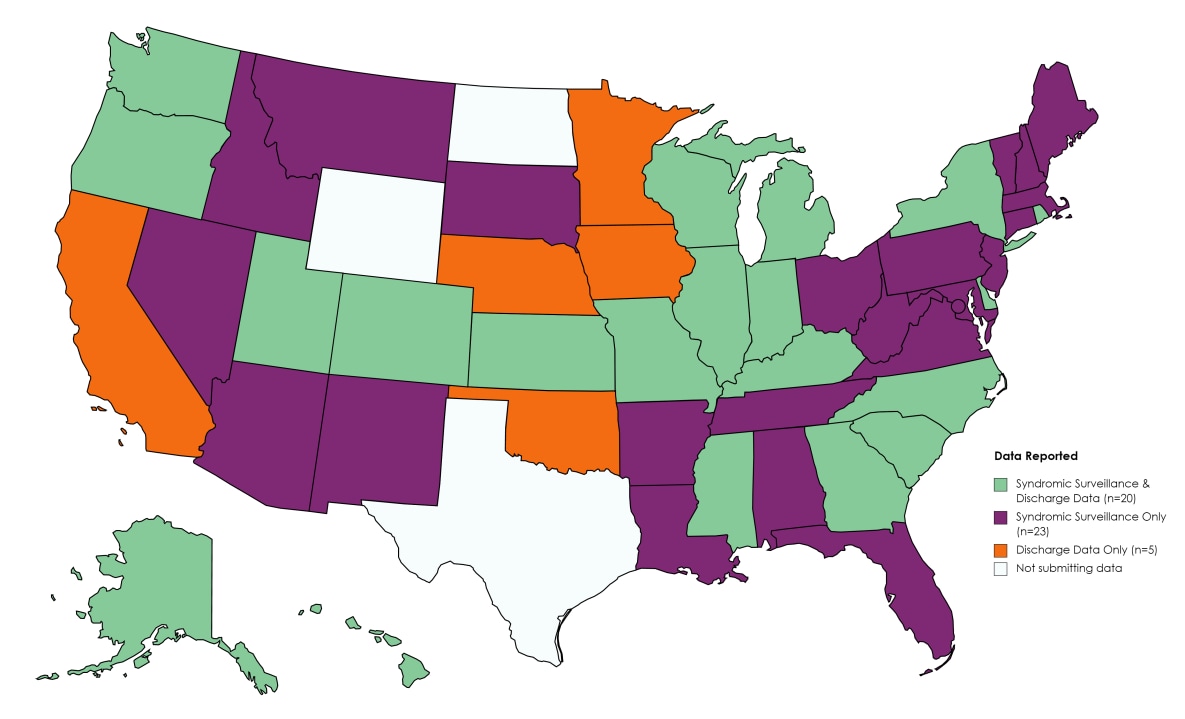
Figure 1. Jurisdictions participating in CDC’s Drug Overdose Surveillance and Epidemiology (DOSE) system, 2018-2021

Explore nonfatal overdose data from CDC’s Drug Overdose Surveillance and Epidemiology (DOSE) system:
DOSE leverages timely ED syndromic surveillance data captured by health departments to rapidly assess trends and maintain situational awareness of changes in suspected nonfatal drug overdose-related ED visits at the local, state, and national level. On average, more than 90% of ED visits among the 42 participating states and the District of Columbia are captured within the syndromic surveillance data (Figure 1).
Jurisdictions share aggregate data on ED visits for suspected nonfatal all drug, heroin-, all opioid-, and all stimulant-involved overdoses with CDC with a one-month delay. Syndromic surveillance data are preliminary and may not contain a confirmed diagnosis. Suspected overdoses identified may not be confirmed by toxicological testing, which is often limited in EDs. Data are disaggregated by (1) age group and sex, and (2) county of patient residence. The number of jurisdictions included in the calculations of monthly and annual percent change estimates in rates varies over time. Additionally, comparisons between jurisdictions should not be made because of variations in data quality, completeness, and reporting across jurisdictions. Although coverage is high within participating states (>90% on average), these data are not nationally representative.
SYNDROMIC SURVEILLANCE DEFINITIONS
The DOSE system uses standardized syndromic surveillance definitions for suspected nonfatal all drug, heroin-, all opioid-, and all stimulant-involved overdoses established by CDC. All definitions draw from multiple fields within ED data to classify visits as overdose-related.
Suspected nonfatal overdose-related ED visits are identified according to diagnostic codes used for clinical diagnosis and insurance billing purposes, specifically, International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) codes, International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes, and SNOMED CT (Systematized Nomenclature of Medicine — Clinical Terms) codes. Where manner of injury is defined, only diagnosis codes for “unintentional” or “undetermined” intent drug poisoning are included in the DOSE standardized syndromic surveillance definitions.
Although many diagnostic codes provide sufficient indication of a suspected drug overdose, another subset of diagnostic codes specific to opioid drug use, abuse, and dependence is less specific; therefore, when these are the only codes present, additional information (e.g., chief complaint field) is needed for the ED visit to be captured as a suspected opioid-involved overdose.
Syndromic surveillance definitions also utilize the free text field called “chief complaint”, which represents the purpose of an ED visit, for example, “Patient was found unresponsive. Emergency medical services (EMS) provided Narcan and patient said took heroin.” The amount and type of information provided in unstandardized text such as the chief complaint field can vary. To be included as an overdose-related ED visit based on chief complaint, records must include two components: 1) text indicating an overdose or poisoning and 2) text indicating the involvement of a drug or a diagnostic code for opioid use, abuse, and dependence. The free text search of the chief complaint field is not case sensitive and common misspellings of key search terms, for example, “herion” instead of “heroin”, are also included. A list of exclusions is applied to the chief complaint field after all inclusion criteria have been assessed. For example, if a diagnostic code for heroin-involved poisoning is not present, exclusions such as “no loss of consciousness”, “denied heroin”, “detox”, and “withdrawal” would be applied and therefore the visit would not be captured as a suspected heroin-involved overdose.
The syndromic surveillance definitions are not mutually exclusive but rather reflect nesting of drug categories. Heroin-, opioid-, and stimulant-involved overdose visits are included in the numbers of suspected all drug overdose visits. Heroin-involved overdose visits are included in the numbers of suspected opioid-involved overdose visits. Additionally, some overdose visits may involve multiple substances (e.g., a given overdose-related ED visit could have involved both opioids and stimulants).
Please click on each link below to see the full nonfatal syndromic surveillance definition:
DOSE leverages finalized discharge data from ED visits and inpatient hospitalizations to estimate trends in nonfatal overdoses and calculate burden. Discharge data offer a more complete and accurate understanding of overdose burden compared to syndromic surveillance data. Currently, 25 states participate in DOSE discharge data sharing: 18 states submit ED and inpatient hospitalization discharge data, 4 states submit only ED discharge data, and 3 states submit only inpatient hospitalization discharge data (Figure 2). The average percent of ED visits and inpatient hospitalizations currently captured from states participating in DOSE discharge data sharing is 90%.
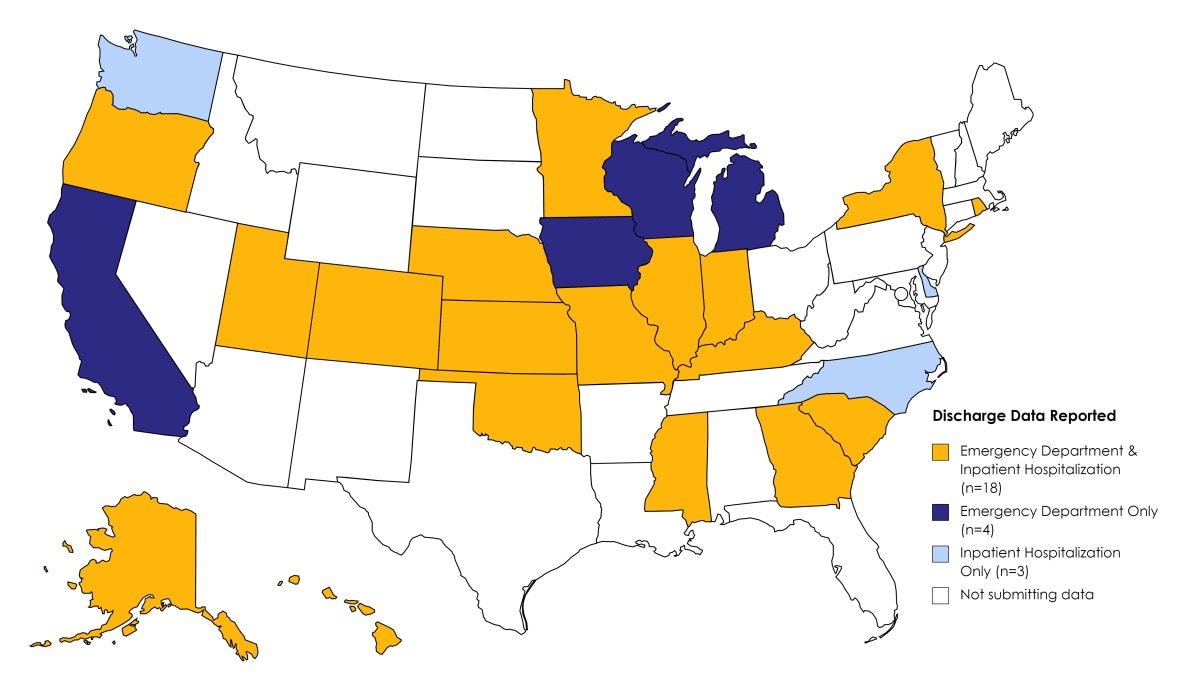
Figure 2. States participating in CDC’s DOSE system that report emergency department and/or inpatient hospitalization discharge data, 2018‒2021.
Participating jurisdictions share aggregate data on monthly ED visits and inpatient hospitalizations involving nonfatal all drug, all opioid-, heroin-, and all stimulant-involved overdoses with CDC quarterly, with a 3.5-month lag. Whereas syndromic surveillance data are preliminary and may not contain a confirmed diagnosis, discharge data may offer a more complete and accurate estimation of overdose burden in EDs and among hospitalizations. Data are reported by (1) age group, sex, and intentionality, and (2) county of patient residence and intentionality.
ED and inpatient hospitalization discharge data are collected for administrative/billing purposes. The standardized coding scheme is considered more reliable than self-reports, and less expensive to obtain than survey data or medical chart abstractions. However, billing coders assign diagnosis codes in discharge data and the assigned codes may not provide a fully accurate, comprehensive account of the conditions treated. Diagnosis codes may be reported strategically to optimize reimbursement and surveillance for drug overdoses using these data may not accurately reflect the true overdose burden.
Additionally, the overdoses identified may not be confirmed by toxicological testing, which is often limited in ED or hospital settings. Data not available by the reporting deadline may not ever be submitted, as data are typically considered final at submission. Comparisons between ED and inpatient hospitalization discharge data should be made with caution, as some states submit ED data only or inpatient hospitalization data only. Although coverage is high within participating states (>90% on average), these data are not nationally representative.
DISCHARGE DATA DEFINITIONS
The DOSE system uses standardized discharge data definitions for nonfatal all drug, heroin-, all opioid-, and all stimulant-involved overdoses established by CDC.
While syndromic surveillance definitions are applied to the chief complaint and discharge diagnosis codes available immediately following a patient encounter, discharge data definitions are applied to ICD-10-CM codes reported in finalized medical billing data discharge diagnosis fields. Discharge data definitions are applied by submitting jurisdictions to identify initial encounters for acute drug poisonings, stratified by intent (unintentional and undetermined intent, or intentional self-harm). Although discharge data on intentional self-harm are reported to DOSE, these visits are not reported in the DOSE Nonfatal Overdose Emergency Department and Inpatient Hospitalization Discharge Data Dashboard at this time.
Similar to the syndromic surveillance definitions, the discharge data definitions are nested. All drug overdose visit counts include heroin-, opioid-, and stimulant-involved overdose visits, in addition to overdoses involving other drug classes outlined in the discharge data definitions below. Opioid-involved overdose visit counts include all heroin-involved overdoses. Additionally, some overdose visits may involve multiple substances (e.g., a given overdose-related ED visit or hospitalization could have involved both opioids and stimulants so the single visit would count towards both).
The tables below describe unintentional and undetermined intent ICD-10-CM codes for discharge data definitions:
| ICD-10-CM for unintentional or undetermined intent | Description |
| T36.0X1A, T36.0X4A, T36.1X1A, T36.1X4A, T36.2X1A, T36.2X4A, T36.3X1A, T36.3X4A, T36.4X1A, T36.4X4A, T36.5X1A, T36.5X4A, T36.6X1A, T36.6X4A, T36.7X1A, T36.7X4A, T36.8X1A, T36.8X4A, T36.91XA, T36.94XA | Poisoning by systemic antibiotics, such as penicillins, cephalosporins and other beta-lactam antibiotics, chloramphenicol group, etc. |
| T37.0X1A, T37.0X4A, T37.1X1A, T37.1X4A, T37.2X1A, T37.2X4A, T37.3X1A, T37.3X4A, T37.4X1A, T37.4X4A, T37.5X1A, T37.5X4A, T37.8X1A, T37.8X4A, T37.91XA, T37.94XA | Poisoning by other systemic anti-infectives and antiparasitics, such as sulfonamides, antimycobacterial drugs, antimalarials and drugs acting on other blood protozoa, etc. |
| T38.0X1A, T38.0X4A, T38.1X1A, T38.1X4A, T38.2X1A, T38.2X4A, T38.3X1A, T38.3X4A, T38.4X1A, T38.4X4A, T38.5X1A, T38.5X4A, T38.6X1A, T38.6X4A, T38.7X1A, T38.7X4A, T38.801A, T38.804A, T38.811A, T38.814A, T38.891A, T38.894A, T38.901A, T38.904A, T38.991A, T38.994A | Poisoning by hormones and their synthetic substitutes and antagonists, not elsewhere classified, such as glucocorticoids and synthetic analogues, thyroid hormones and substitutes, antithyroid drugs, etc. |
| T39.011A, T39.014A, T39.091A, T39.094A, T39.1X1A, T39.1X4A, T39.2X1A, T39.2X4A, T39.311A, T39.314A, T39.391A, T39.394A, T39.4X1A, T39.4X4A, T39.8X1A, T39.8X4A, T39.91XA, T39.94XA | Poisoning by nonopioid analgesics, antipyretics and antirheumatics, such as aspirin, salicylates, 4-Aminophenol derivatives, etc. |
| T40.0X1A, T40.0X4A, T40.1X1A, T40.1X4A, T40.2X1A, T40.2X4A, T40.3X1A, T40.3X4A, T40.4X1A, T40.4X4A, T40.411A, T40.414A, T40.421A, T40.424A, T40.491A, T40.494A, T40.5X1A, T40.5X4A, T40.601A, T40.604A, T40.691A, T40.694A, T40.7X1A, T40.7X4A, T40.711A, T40.714A, T40.721A, T40.724A, T40.8X1A, T40.8X4A, T40.901A, T40.904A,T40.991A, T40.994A | Poisoning by narcotics and psychodysleptics [hallucinogens], such as fentanyl, heroin, cocaine, cannabis, etc. |
| T41.0X1A, T41.0X4A, T41.1X1A, T41.1X4A, T41.201A, T41.204A, T41.291A, T41.294A, T41.3X1A, T41.3X4A, T41.41XA, T41.44XA, T41.5X1A, T41.5X4A | Poisoning by anesthetics and therapeutic gases, such as inhaled anesthetics, intravenous anesthetics, unspecified general anesthetics, etc. |
| T42.0X1A, T42.0X4A, T42.1X1A, T42.1X4A, T42.2X1A, T42.2X4A, T42.3X1A, T42.3X4A, T42.4X1A, T42.4X4A, T42.5X1A, T42.5X4A, T42.6X1A, T42.6X4A, T42.71XA, T42.74XA, T42.8X1A, T42.8X4A | Poisoning by antiepileptic, sedative-hypnotic and antiparkinsonism drugs, such as hydantoin derivatives, iminostilbenes, succinimides and oxazolidinediones, etc. |
| T43.011A, T43.014A, T43.021A, T43.024A, T43.1X1A, T43.1X4A, T43.201A, T43.204A, T43.211A, T43.214A, T43.221A, T43.224A, T43.291A, T43.294A, T43.3X1A, T43.3X4A, T43.4X1A, T43.4X4A, T43.501A, T43.504A, T43.591A, T43.594A, T43.601A, T43.604A, T43.611A, T43.614A, T43.621A, T43.624A, T43.631A, T43.634A, T43.641A, T43.644A, T43.651A, T43.654A, T43.691A, T43.694A, T43.8X1A,T43.8X4A, T43.91XA, T43.94XA | Poisoning by psychotropic drugs, not elsewhere classified, such as tricyclic antidepressants, methamphetamines, other psychostimulants, etc. |
| T44.0X1A, T44.0X4A, T44.1X1A, T44.1X4A, T44.2X1A, T44.2X4A, T44.3X1A, T44.3X4A, T44.4X1A, T44.4X4A, T44.5X1A, T44.5X4A, T44.6X1A, T44.6X4A, T44.7X1A, T44.7X4A, T44.8X1A, T44.8X4A, T44.901A, T44.904A, T44.991A, T44.994A | Poisoning by drugs primarily affecting the autonomic nervous system, such as anticholinesterase agents, other parasympathomimetics [cholinergics], ganglionic blocking drugs, etc. |
| T45.0X1A, T45.0X4A, T45.1X1A, T45.1X4A, T45.2X1A, T45.2X4A, T45.3X1A, T45.3X4A, T45.4X1A, T45.4X4A, T45.511A, T45.514A, T45.521A, T45.524A, T45.601A, T45.604A, T45.611A, T45.614A, T45.621A, T45.624A, T45.691A, T45.694A, T45.7X1A, T45.7X4A, T45.8X1A, T45.8X4A, T45.91XA, T45.94XA | Poisoning by primarily systemic and hematological agents, not elsewhere classified, such as antiallergic and antiemetic drugs, antineoplastic and immunosuppressive drugs, vitamins, etc. |
| T46.0X1A, T46.0X4A, T46.1X1A, T46.1X4A, T46.2X1A, T46.2X4A, T46.3X1A, T46.3X4A, T46.4X1A, T46.4X4A, T46.5X1A, T46.5X4A, T46.6X1A, T46.6X4A, T46.7X1A, T46.7X4A, T46.8X1A, T46.8X4A, T46.901A, T46.904A, T46.991A, T46.994A | Poisoning by agents primarily affecting the cardiovascular system, such as cardiac-stimulant glycosides and drugs of similar action, calcium-channel blockers, other antidysrhythmic drugs, etc. |
| T47.0X1A, T47.0X4A, T47.1X1A, T47.1X4A, T47.2X1A, T47.2X4A, T47.3X1A, T47.3X4A, T47.4X1A, T47.4X4A, T47.5X1A, T47.5X4A, T47.6X1A, T47.6X4A, T47.7X1A, T47.7X4A, T47.8X1A, T47.8X4A, T47.91XA, T47.94XA | Poisoning by agents primarily affecting the gastrointestinal system, such as histamine H2-receptor blockers, other antacids and anti-gastric-secretion drugs, stimulant laxatives, etc. |
| T48.0X1A, T48.0X4A, T48.1X1A, T48.1X4A, T48.201A, T48.204A, T48.291A, T48.294A, T48.3X1A, T48.3X4A, T48.4X1A, T48.4X4A, T48.5X1A, T48.5X4A, T48.6X1A, T48.6X4A, T48.901A, T48.904A, T48.991A, T48.994A | Poisoning by agents primarily acting on smooth and skeletal muscles and the respiratory system, such as oxytocic drugs, skeletal muscle relaxants [neuromuscular blocking agents], unspecified drugs acting on muscles, etc. |
| T49.0X1A, T49.0X4A, T49.1X1A, T49.1X4A, T49.2X1A, T49.2X4A, T49.3X1A, T49.3X4A, T49.4X1A, T49.4X4A, T49.5X1A, T49.5X4A, T49.6X1A, T49.6X4A, T49.7X1A, T49.7X4A, T49.8X1A, T49.8X4A, T49.91XA, T49.94XA | Poisoning by topical agents primarily affecting skin and mucous membrane and by ophthalmological, otorhinorlaryngological and dental drugs, such as local antifungal, anti-infective and anti-inflammatory drugs, antipruritics, local astringents and local detergents, etc. |
| T50.0X1A, T50.0X4A, T50.1X1A, T50.1X4A, T50.2X1A, T50.2X4A, T50.3X1A, T50.3X4A, T50.4X1A, T50.4X4A, T50.5X1A, T50.5X4A, T50.6X1A, T50.6X4A, T50.7X1A, T50.7X4A, T50.8X1A, T50.8X4A, T50.901A, T50.904A, T50.911A, T50.914A, T50.991A, T50.994A, T50.A11A, T50.A14A, T50.A21A, T50.A24A, T50.A91A, T50.A94A, T50.B11A, T50.B14A, T50.B91A, T50.B94A, T50.Z11A, T50.Z14A, T50.Z91A, T50.Z94A | Poisoning by diuretics and other and unspecified drugs, medicaments and biological substances, such as mineralocorticoids and their antagonists, loop [high-ceiling] diuretics, carbonic-anhydrase inhibitors, benzothiadiazides and other diuretics, etc. |
1ICD-10-CM codes included in discharge data definitions are limited to those that indicated accidental (unintentional) or undetermined intent and indicated an initial encounter for the drug poisoning. Codes that indicated adverse effect of or underdosing are not included in DOSE discharge data definitions.
| ICD-10-CM for unintentional or undetermined intent | Description |
| T40.1X1A | Poisoning by heroin, accidental (unintentional), initial encounter. |
| T40.1X4A | Poisoning by heroin, undetermined, initial encounter. |
| ICD-10-CM for unintentional or undetermined intent | Description |
| T40.0X1A | Poisoning by opium, accidental (unintentional), initial encounter. |
| T40.0X4A | Poisoning by opium, undetermined, initial encounter. |
| T40.1X1A | Poisoning by heroin, accidental (unintentional), initial encounter. |
| T40.1X4A | Poisoning by heroin, undetermined, initial encounter. |
| T40.2X1A | Poisoning by other opioids, accidental (unintentional), initial encounter. |
| T40.2X4A | Poisoning by other opioids, undetermined, initial encounter. |
| T40.3X1A | Poisoning by methadone, accidental (unintentional), initial encounter. |
| T40.3X4A | Poisoning by methadone, undetermined, initial encounter. |
| T40.4X1A | Poisoning by other synthetic narcotics, accidental (unintentional), initial encounter.
[This code was replaced by T40.411A, T40.421A, and T40.491A beginning October 1, 2020.] |
| T40.4X4A | Poisoning by other synthetic narcotics, undetermined, initial encounter.
[This code was replaced by T40.414A, T40.424A, and T40.494A beginning October 1, 2020.] |
| T40.411A | Poisoning by fentanyl or fentanyl analogs, accidental (unintentional), initial encounter. |
| T40.414A | Poisoning by fentanyl or fentanyl analogs, undetermined, initial encounter. |
| T40.421A | Poisoning by tramadol, accidental (unintentional), initial encounter. |
| T40.424A | Poisoning by tramadol, undetermined, initial encounter. |
| T40.491A | Poisoning by other synthetic narcotics, accidental (unintentional), initial encounter. |
| T40.494A | Poisoning by other synthetic narcotics, undetermined, initial encounter. |
| T40.601A | Poisoning by unspecified narcotics, accidental (unintentional), initial encounter. |
| T40.604A | Poisoning by unspecified narcotics, undetermined, initial encounter. |
| T40.691A | Poisoning by other narcotics, accidental (unintentional), initial encounter. |
| T40.694A | Poisoning by other narcotics, undetermined, initial encounter. |
| ICD-10-CM for unintentional or undetermined intent | Description |
| T40.5X1A | Poisoning by cocaine, accidental (unintentional), initial encounter. |
| T40.5X4A | Poisoning by cocaine, undetermined, initial encounter. |
| T43.601A | Poisoning by unspecified psychostimulants, accidental (unintentional), initial encounter. |
| T43.604A | Poisoning by unspecified psychostimulants, undetermined, initial encounter. |
| T43.611A | Poisoning by caffeine, accidental (unintentional), initial encounter. |
| T43.614A | Poisoning by caffeine, undetermined, initial encounter. |
| T43.621A | Poisoning by amphetamines, accidental (unintentional), initial encounter. |
| T43.624A | Poisoning by amphetamines, undetermined, initial encounter. |
| T43.631A | Poisoning by methylphenidate, accidental (unintentional), initial encounter. |
| T43.634A | Poisoning by methylphenidate, undetermined, initial encounter. |
| T43.641A | Poisoning by ecstasy, accidental (unintentional), initial encounter. |
| T43.644A | Poisoning by ecstasy, undetermined, initial encounter. |
| T43.651A | Poisoning by methamphetamines, accidental (unintentional), initial encounter. |
| T43.654A | Poisoning by methamphetamines, undetermined, initial encounter. |
| T43.691A | Poisoning by other psychostimulants, accidental (unintentional), initial encounter. |
| T43.694A | Poisoning by other psychostimulants, undetermined, initial encounter. |
The following four data reports come from CDC’s Enhanced State Opioid Overdose Surveillance (ESOOS) program, which was funded from 2016-2019 to provide more timely and comprehensive data on fatal and nonfatal opioid overdoses and risk factors associated with fatal overdoses. Twelve states were initially funded in September 2016, and an additional 20 states and the District of Columbia were funded in September 2017, to share data on nonfatal all drug, all opioid, and/or heroin overdoses with CDC on a quarterly basis. Data from ESOOS have not been updated since April 2019, and data may differ from those in the DOSE system. For example, ESOOS states were able to develop and apply their own overdose case definitions, whereas DOSE required standardized case definitions to be used across all funded recipients. Furthermore, stimulant overdose data are reported in the DOSE system but were not collected as part of the ESOOS program.
Data reports from CDC’S DOSE system on overdoses during the COVID-19 pandemic
The data report below comes from CDC’s DOSE system. The report displays total ED visits, ED visit counts for suspected overdoses, and overdose rates overall and by 41 states and the District of Columbia, through September 2020. During the first several months of the COVID-19 pandemic, the number of total ED visits across the United States substantially declined; however, nonfatal overdoses did not decline at a similar pace.
There are several important caveats to consider when viewing the figures included in this report. During the COVID-19 pandemic, states onboarded new facilities that began sharing data; also, some facilities stopped sharing data during this period. Thus, the number of facilities included was not constant over this time period. In addition, states collaborated with existing facilities to increase the proportion of ED visits that contained diagnosis codes, which facilitates the identification of overdose-related visits. Caution is warranted in interpreting counts, rates, and comparisons over time due to these data issues.
- Drug Overdose Surveillance and Epidemiology (DOSE) System Fact Sheet
- State, Local Communities, & Tribes Information
- DOSE Dashboard: Nonfatal Overdose Syndromic Surveillance Data
- DOSE Dashboard: Nonfatal Overdose Emergency Department and Inpatient Hospitalization Discharge Data
- The Fentalog Study: A Subset of Nonfatal Suspected Opioid Overdoses with Toxicology Testing
- SUDORS Dashboard: Fatal Overdose Data
- CDC’s ESOOS Program

