Key points
- Rapid, accurate rabies diagnoses are crucial for timely administration of post-exposure prophylaxis (PEP) following potential rabies exposures.
- These results can help decide if costly PEP is needed and potentially save patients from unnecessary physical, emotional, and financial stress.
- Different rabies specimens require different laboratory tests to confirm or rule out rabies infection.

Test approaches
Diagnosis in animals
Rabies testing requires that the animal be euthanized. There are no approved methods for antemortem rabies testing of animals. Professionals should immediately euthanize animals showing signs of rabies and submit specimens to a qualified rabies laboratory for testing. A rabies diagnosis can be made after detecting rabies virus from any part of the affected brain. To rule out rabies, the test must include a full cross-section of tissue from both the brain stem and cerebellum.
In the United States, the results of a rabies test are typically available within 24 to 72 hours after a specimen is received by the laboratory. Suspected rabies exposure requires urgent medical attention, but most people with suspected rabies exposure can delay post-exposure prophylaxis until the results of this test are returned. Rabies testing of animals is reportable to state health departments and CDC.
Methods approved for diagnosing rabies in animals
- Direct fluorescent antibody test
- Direct rapid immunohistochemical test
- Immunohistochemistry
- Realtime reverse transcription-polymerase chain reaction
Diagnosis in humans
Several tests are necessary to diagnose rabies antemortem (before death) in humans; no single test is sufficient. Tests are performed on samples of saliva, serum, cerebrospinal fluid, and nuchal skin biopsies. Antemortem human rabies testing that is negative is a strong indication that the patient does not have rabies, but postmortem (after death) confirmatory testing should be pursued if an alternative diagnosis is not identified.
Postmortem testing requires the collection of brainstem and cerebellum tissues.
Due to the risk of rabies exposure to healthcare workers and close community contacts, deceased patients suspected of rabies should always undergo an autopsy and post-mortem rabies testing. Rabies testing in humans is reportable to state health departments and CDC.
Methods approved for diagnosing rabies in humans
- Direct fluorescent antibody test
- Immunohistochemistry
- Realtime reverse transcription-polymerase chain reaction
- Rabies serology
Assessing immune response to rabies vaccine
Rabies virus-neutralizing antibody tests are used to assess the immune response after vaccination. In certain cases, such as international travel, pets may be required to have a rabies antibody test to ensure they are adequately vaccinated.
For most people completing an approved rabies vaccination regimen, routine serological testing is not necessary to document seroconversion, unless:
- The person is immunosuppressed.
- There are significant deviations from the prophylaxis schedule.
- The patient was vaccinated outside the United States with a product of questionable quality.
- The person's antibody status is being monitored routinely due to occupational exposure to rabies virus.
If you need help determining if this test is appropriate, consult your health department. Testing may be available through your state health department, a research university, or one of these commercial laboratories:
Atlanta Health Associates*
309 Pirckle Ferry Road, Suite D300
Cumming, GA 30040
Phone: 770-205-9091 or 800-717-5612
Fax: 770-204-9021
www.atlantahealth.net
Kansas State University (KSU)*
1800 Denison Avenue
Manhattan, KS 66506-5600
Phone: 785-532-4483
www.ksvdl.org/rabies-laboratory
Testing at KSU may also be requested through Quest Labs as Rabies Vaccine Response End Point Titer (order # 5789).
University of Missouri One Health–Rabies Laboratory*
Veterinary Medical Diagnostic Laboratory
University of Missouri
901 E. Campus Loop
Columbia, MO 65211
Phone: 573-882-3646 or 800-862-8635
Fax: 573-882-7120
Email: muvmdlrabies@missouri.edu
vmdl.missouri.edu/one-health-rabies
*Use of trade names, commercial sources, or private organizations is for identification only and does not imply endorsement by the U.S. Department of Health and Human Services and/or CDC.
Diagnostic testing methods
Several tests can confirm a rabies infection, but tests with high sensitivity and specificity should be used to rule out rabies.
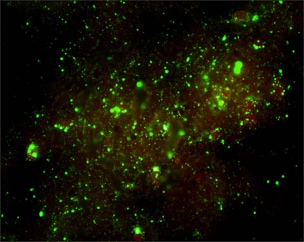
Direct fluorescent antibody (DFA) test
The DFA test demonstrates that animals with rabies have rabies virus- expressed proteins (antigens) in their tissues.
- Brain tissues are ideal for this test because rabies is present in nervous tissue (and not blood like many other viruses).
- Other innervated tissues may have antigens, but these tissues are less accurate at detecting rabies when compared to brain tissues.
- The most important part of a DFA test is fluorescently labeled anti-rabies antibody.
- When the labeled antibody is incubated with rabies-suspect brain tissue, it will bind to rabies antigen.
- Unbound antibodies can be washed away and areas where antigen is present can be visualized as fluorescent-apple-green areas using a fluorescence microscope.
- If rabies virus is absent, there will be no staining.
The DFA test has high sensitivity and specificity for detecting rabies and has been rigorously evaluated by international, national, and state health laboratories.
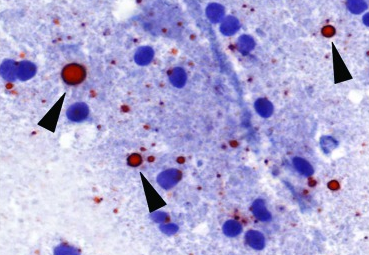
Direct rapid immunohistochemical test (DRIT)
The DRIT for rabies functions similarly to the DFA test in detecting the presence of rabies virus antigen in animal tissues. Like DFA, DRIT relies on observing rabies virus-expressed proteins in infected nervous system tissues.
- Brain tissue is ideal due to its high concentration of rabies antigen.
- Other innervated tissues may have antigens, but they are less accurate at detecting rabies when compared to brain tissues.
- The key component of the DRIT test is rapid immunohistochemical staining with anti-rabies antibodies.
- These antibodies are labeled with a chromogenic marker and when incubated with suspect tissue, the marker binds specifically to rabies antigen.
- Excess antibodies are then washed away, and areas containing rabies antigens appear in color under a light microscope.
- The absence of staining indicates the absence of rabies virus
Like DFA, DRIT boasts high sensitivity and specificity. It has been thoroughly evaluated by international, national, and state health laboratories.
Realtime Reverse Transcriptase Polymerase Chain Reaction (RT-PCR)
The LN34 PCR test for rabies is a newer diagnostic test that uses real-time reverse transcriptase polymerase chain reaction (real-time RT-PCR) methodology to detect the presence of rabies virus genetic material.
- Rabies rule-out requires a full cross-section of the brainstem and representative samples from the cerebellum.
- LN34 can detect rabies in suspect human rabies cases using antemortem skin biopsy samples from the nape of the neck and saliva samples.
- Its versatility allows for testing on a variety of sample types, including decomposed or formalin-fixed tissues, which may not be viable for other diagnostic techniques.
- This innovative test targets a highly conserved region of the virus genome, including the leader region and nucleoprotein gene, which ensures robust detection across all viruses that can cause rabies.
- LN34 works by a single-tube reaction where viral genetic material is amplified into many copies and detected by a fluorescent probe.
The LN34 PCR test offers numerous advantages, including its exceptional sensitivity, specificity, rapid turnaround time, and specimen versatility.
Immunohistochemistry (IHC)
IHC methods are sensitive and specific for the detection of rabies virus antigen in formalin-fixed tissues. IHC testing is more sensitive and specific than histologic staining methods, such as hematoxylin and eosin (H&E) and Sellers stains.
- Brain tissues fixed in formalin must first be processed by routine histologic methods, embedded in paraffin, and sectioned to formalin-fixed paraffin-embedded slides.
- Rabies virus antigen is detected using specific anti-rabies monoclonal or polyclonal antibodies.

Rabies serology
Two serological assays are considered acceptable for detecting rabies virus neutralizing antibodies: Rapid Fluorescent Focus Inhibition Test (RFFIT) and Fluorescent Antibody Virus Neutralization (FAVN) test. These assays cannot differentiate between an antibody response to vaccination or as a result of infection.
- Detection of neutralizing antibodies in cerebrospinal fluid or the serum of an unvaccinated individual is considered a positive test for rabies virus infection
- RFFIT (human and animals) and FAVN (animals) are also used to confirm an adequate vaccination response. A serological titer greater than or equal to 0.5 international units per milliliter is considered evidence of an adequate immune response.
- Serological testing may also be performed in animals to confirm a vaccine response and should align with NASPHV Compendia.
The indirect immunofluorescence assay (IFA) detects binding antibodies against rabies virus encoded proteins and can be an early indication of rabies virus infection in humans. This test is only used as part of antemortem rabies testing in humans. IFA test has the advantage of detecting isotype specific response, i.e. IgM and IgG antibodies.
Diagnostic test kits
Recently, point-of-care diagnostic tests have become increasingly available to the public. Promising studies conducted in Africa, Asia, and the United States have found that certain point-of-care tests can demonstrate high sensitivity and specificity. However, no point-of-care test for rabies has been rigorously validated and none are approved for use by USDA, CDC's National Rabies Reference Laboratory, WHO, or WOAH.
In general, if a diagnostic product contains all materials needed to run a particular test, including instructions on the interpretation of results, and if the intent of the manufacturer is to provide a self-contained, point-of-care product, the product may be considered a diagnostic kit. The kit is under regulation by the United States Department of Agriculture Center for Veterinary Biologics and the Animal and Plant Health Inspection Service.