Increase in Extensively Drug-Resistant Shigellosis in the United States

Distributed via the CDC Health Alert Network
February 24, 2023, 11:30 AM ET
CDCHAN-00486
Summary
The Centers for Disease Control and Prevention (CDC) has been monitoring an increase in extensively drug-resistant (XDR) Shigella infections (shigellosis) reported through national surveillance systems [1]. In 2022, about 5% of Shigella infections reported to CDC were caused by XDR strains, compared with 0% in 2015. Clinicians treating patients infected with XDR strains have limited antimicrobial treatment options. Shigella bacteria are easily transmissible. XDR Shigella strains can spread antimicrobial resistance genes to other enteric bacteria. Given these potentially serious public health concerns, CDC asks healthcare professionals to be vigilant about suspecting and reporting cases of XDR Shigella infection to their local or state health department and educating patients and communities at increased risk about prevention and transmission.
Shigellosis is an acute enteric infection that is an important cause of domestically acquired and travel-associated bacterial diarrhea in the United States. Shigellosis usually causes inflammatory diarrhea that can be bloody and may also lead to fever, abdominal cramping, and tenesmus. Infections are generally self-limiting; however, antimicrobial treatment may be indicated to prevent complications or shorten the duration of illness [2]. CDC defines XDR Shigella bacteria as strains that are resistant to all commonly recommended empiric and alternative antibiotics — azithromycin, ciprofloxacin, ceftriaxone, trimethoprim-sulfamethoxazole (TMP-SMX), and ampicillin. Currently, there are no data from clinical studies of treatment of XDR Shigella to inform recommendations for the optimal antimicrobial treatment of these infections. As such, CDC does not have recommendations for optimal antimicrobial treatment of XDR Shigella infections.
Background
Shigella bacteria are transmitted by the fecal-oral route, directly through person-to-person contact including sexual contact, and indirectly through contaminated food, water, and other routes. Shigella bacteria are easily transmitted because of the low infectious dose (as few as 10–100 organisms), and outbreaks tend to occur among people in close-contact settings [2–6].
Historically, shigellosis has predominantly affected young children (age 1–4 years) in the United States. More recently, CDC has observed an increase in antimicrobial-resistant Shigella infections among adult populations [4,5] especially
- Gay, bisexual, and other men who have sex with men (MSM)
- People experiencing homelessness
- International travelers
- People living with HIV
Most people with diarrheal illness require only supportive care and fluid replacement. Antimicrobial agents are not always needed for mild shigellosis, but they may be indicated to
- Shorten the duration of illness (by about 2 days), or
- Reduce the likelihood of transmission, for example
- during outbreaks,
- in institutional settings,
- from food handlers,
- to immunocompromised persons or those being treated with immunosuppressive drugs, and
- to people living with HIV.
In the United States, recommended empiric antimicrobial agents include azithromycin, ciprofloxacin, or ceftriaxone. Ampicillin or TMP-SMX are recommended as alternative treatments for susceptible strains [2].
In the United States, the percentage of Shigella infections caused by XDR strains reported to CDC increased from zero in 2015 to 5% in 2022 (Figure). Between January 1, 2015, and January 22, 2023, CDC received reports of 239 XDR Shigella isolates, with Shigella sonnei accounting for the largest percentage (66%) followed by Shigella flexneri (34%). The median age of patients was 42 years (range 1–83 years). Among 232 patients with available information, 82% were men, 13% were women, and 5% were children. Among 41 patients who answered questions about recent sexual activity, 88% reported male-to-male sexual contact.
Figure: Percentage of Shigella isolates that showed an extensively drug resistant (XDR)* phenotype or genotype in the United States, by year, 2015–2022†
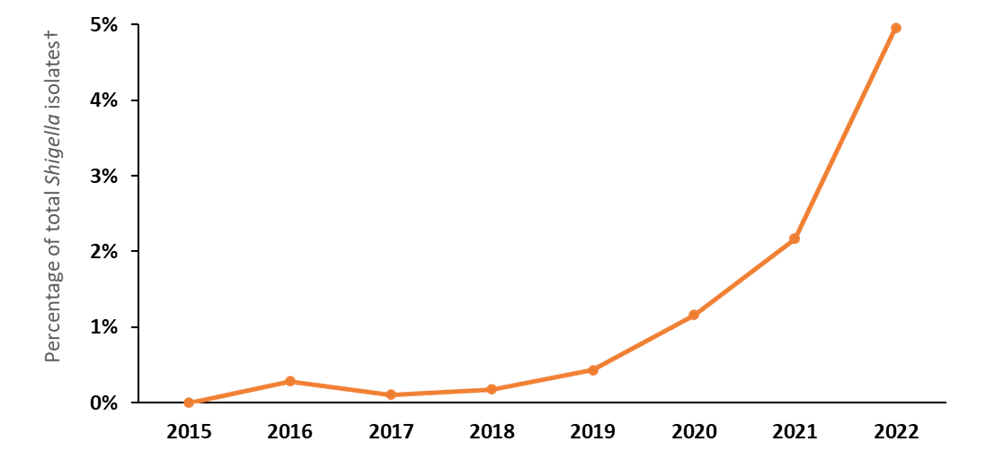
*XDR Shigella bacteria (n=239) are defined as resistant to azithromycin, ciprofloxacin, ceftriaxone, trimethoprim-sulfamethoxazole, and ampicillin.
†Among sequenced Shigella isolates submitted to CDC’s PulseNet Whole Genome Sequencing Database; data are preliminary and based on broth microdilution susceptibility testing and/or presence of resistance genes and mutations found in whole genome sequences of bacterial DNA.
CDC will continue to monitor XDR Shigella infections and track Shigella isolates with unique or worrisome antimicrobial susceptibility patterns and genetic resistance markers. In addition, CDC is conducting an analysis of antimicrobial-resistant Shigella infections in the United States using data in the National Antimicrobial Resistance Monitoring System for Enteric Bacteria (NARMS).
Recommendations for Healthcare Professionals
Diagnosis
- Consider shigellosis in the differential diagnosis of acute diarrhea, especially for patients at higher risk for Shigella infection, including
- Young children
- MSM
- People experiencing homelessness
- International travelers
- Immunocompromised persons
- People living with HIV
- If shigellosis is suspected,
- Ask the patient about relevant exposures and social history, including sexual activity, housing status, and international travel.
- When ordering diagnostic testing for Shigella, stool culture is preferred for patients who will require antimicrobial treatment.
- If a culture-independent diagnostic test (CIDT) is performed instead of culture and Shigella bacteria are detected, request on sample submission that the clinical laboratory perform reflex culture.
- If a culture is positive for Shigella, order antimicrobial susceptibility testing (AST) to inform antimicrobial selection.
Clinical Management
- Most patients recover from shigellosis without antimicrobial treatment. Oral rehydration may be sufficient for many people with shigellosis.
- Use AST results to guide antimicrobial treatment selection, when possible.
- Encourage patients to inform you if symptoms do not improve within 48 hours after beginning antibiotics.
- To date, there are no CDC recommendations for treating XDR shigellosis in the United States; however, a recent publication from the United Kingdom outlined a possible strategy for treating severe XDR shigellosis using oral pivmecillinam and fosfomycin (for patients with prolonged symptoms or as oral step-down after intravenous treatment) or IV carbapenems and colistin (for hospitalized patients with severe infections or complications) [7].
- XDR Shigella isolates in the United States typically do not carry resistance mechanisms for fosfomycin or carbapenems.
- Note: Pivmecillinam is not commercially available for use in the United States.
- Healthcare providers treating XDR shigellosis should consult with a specialist knowledgeable in treating antibiotic-resistant bacteria to determine the best treatment options.
- Be aware that overusing antibiotics can contribute to the development of antimicrobial resistance. CDC recommends using antibiotics only when clinically indicated.
Considerations for Sexual Health
Increases in drug-resistant Shigella infections have been described among adult men and may be associated with transmission among MSM. Cases of shigellosis co-occurring with other sexually transmitted infections (STIs), including HIV, have been described among MSM [8].
- Take a sexual history if shigellosis is suspected.
- People with acute proctitis and concern for sexually transmitted proctocolitis or enteritis should be tested for other STIs, including HIV, syphilis, gonorrhea, and chlamydia at exposed sites [9].
- Clinicians should encourage all persons with STIs to notify their sex partners and urge them to seek medical evaluation and treatment. Exceptions to this practice include circumstances posing a risk for intimate partner violence [9].
Reporting
- Shigellosis is a nationally notifiable disease. Healthcare professionals and clinical laboratories should report all cases to their local or state health department.
- Healthcare professionals should consult their local or state health department for guidance on when patients may return to childcare, school, or work.
Counseling Patients
Please counsel patients with suspected or confirmed shigellosis about measures they can take to keep others healthy. Patients taking antibiotics should continue to follow prevention measures. All patients with suspected or confirmed shigellosis should
- Stay home from school or from healthcare, food service, or childcare jobs while sick or until the health department says it’s safe to return.
- During diarrhea and for 2 weeks after it ends,
- Abstain from sex (anal, oral, penile, or vaginal).
- Wash hands often with soap and water for at least 20 seconds, including at key times such as after using the toilet, before and after changing diapers, cleaning up after someone who is sick, and before preparing or eating food.
- Do not prepare food for others, if possible.
- Stay out of recreational water, including swimming pools, hot tubs, water playgrounds, oceans, lakes, and rivers.
- Closely follow safer sex practices for at least 2 weeks after resuming sex to prevent the spread of Shigella bacteria that may remain in stool.
- Wash hands, genitals, and anus with soap and water before and after sexual activity.
- Wash hands after touching sex toys, external and internal condoms, dental dams, and any other items that might have been in contact with the vagina or anus.
- Use condoms or dental dams during oral-genital sex and oral-anal sex.
- Use latex gloves during anal fingering or fisting.
- Wash sex toys with soap and water after each use.
Recommendations for Laboratories
- Clinical laboratories should submit known or suspected XDR Shigella isolates to the local or state public health laboratory.
- State laboratories should perform whole genome sequencing whenever possible.
- For questions or concerns, contact CDC at EntericBacteria@cdc.gov.
Recommendations for Public Health Officials
- Be aware that
- Shigella transmission is difficult to control because the bacteria spread easily and rapidly between people, including through sexual activity.
- Drug-resistant Shigella infections have been reported with increasing frequency, particularly among people experiencing homelessness, international travelers, immunocompromised people, and MSM.
- To help CDC gather data to improve outcomes, report information about treatment response and clinical outcomes of XDR Shigella infections to EntericBacteria@cdc.gov.
- Consider working with your infection prevention and control network and other partners to educate providers and people at high risk for XDR Shigella infections.
Recommendations for the Public
Shigella bacteria can spread easily from one person to another – and it only takes a small amount of Shigella to make someone sick. Learn how you can help protect yourself and your loved ones from getting sick.
For More Information
- Shigella and Shigellosis
- Handwashing and Hand Hygiene in Healthcare Settings
- Antimicrobial Resistance
- Antibiotic Prescribing and Use
References
- CDC. National Antimicrobial Resistance Monitoring System (NARMS) Now: Human Data. Atlanta, Georgia: U.S. Department of Health and Human Services, CDC. 2/24/2023.
- Shane AL, Mody RK, Crump J, et al. 2017 Infectious Diseases Society of America clinical practice guidelines for the diagnosis and management of infectious diarrhea. Clin Infect Dis. 2017 Dec; 65(12): p. e45–e80.
- Simms I, Field N, Jenkins C, et al. Intensified shigellosis epidemic associated with sexual transmission in men who have sex with men—Shigella flexneri and S. sonnei in England, 2004 to end of February 2015. Euro Surveill. 2015 Apr; 20(15): 21097.
- Hines JZ, Pinsent T, Rees K, et al. Notes from the field: Shigellosis outbreak among men who have sex with men and homeless persons – Oregon, 2015–2016. MMWR Morb Mortal Wkly Rep. 2016 Aug; 65(31): p. 812–13.
- Shiferaw B, Solghan S, Palmer A, et al. Antimicrobial susceptibility patterns of Shigella isolates in Foodborne Diseases Active Surveillance Network (FoodNet) sites, 2000–2010. Clin Infect Dis. 2012 June; 54(Suppl 5): p. S458–63.
- Mohan K, Hibbert M, Rooney G, et al. What is the overlap between HIV and shigellosis epidemics in England: further evidence of MSM transmission? Sex Transm Infect. 2018 Feb; 94(1): p. 67–71.
- Charles H, Prochazka M, Thorley K, et al. Outbreak of sexually transmitted, extensively drug-resistant Shigella sonnei in the UK, 2021-22: a descriptive epidemiological study. Lancet Infect Dis. 2022 Oct; 22(10): p. 1503–10.
- McNeil CJ, Kirkcaldy RD, Workowski K. Enteric infections in men who have sex with men. Clin Infect Dis. 2022 Apr; 74(Suppl 2): p. S169–78.
- Workowski KA, Bachmann LH, Chan PA, et al. Sexually transmitted infections treatment guidelines, 2021. MMWR Recomm Rep. 2021 Jul; 70(4): p. 1–187.
The Centers for Disease Control and Prevention (CDC) protects people’s health and safety by preventing and controlling diseases and injuries; enhances health decisions by providing credible information on critical health issues; and promotes healthy living through strong partnerships with local, national and international organizations.
Department of Health and Human Services
HAN Message Types
- Health Alert: Conveys the highest level of importance about a public health incident.
- Health Advisory: Provides important information about a public health incident.
- Health Update: Provides updated information about a public health incident.
###
This message was distributed to state and local health officers, state and local epidemiologists, state and local laboratory directors, public information officers, HAN coordinators, and clinician organizations.
###