At a glance

Summary
To reduce the risk of influenza (flu) illness, hospitalization, and death, the Centers for Disease Control and Prevention (CDC) recommends annual flu vaccination for all people ≥6 months who do not have contraindications1. CDC analyzed data from two nationally representative surveys, the National Immunization Survey-Flu (NIS-Flu) and the Behavioral Risk Factor Surveillance System (BRFSS), to estimate flu vaccination coverage for the U.S. population during the 2021–22 flu season. Vaccination coverage with ≥1 dose of flu vaccine was 57.8% among children 6 months through 17 years, a decrease of 0.8 percentage points from the 2020–21 flu season, and flu vaccination coverage among adults ≥18 years was 49.4%, also a decrease of 0.8 percentage points from the prior season. Half of all people ≥6 months (51.4%) were vaccinated during the 2021–22 season, a decrease of 0.7 percentage points from the prior season. Racial/ethnic disparities in flu vaccination coverage persist. Interpretation of the estimates in this report should be done with consideration of the surveys' limitations, including reliance on self or parental reports of vaccination status and low response rates, as well as with consideration of consistency of estimates from other data sources.
Getting a flu vaccine is especially important this fall and winter, when flu viruses and the virus that causes COVID-19 could be spreading simultaneously. Flu vaccination can help prevent or reduce the severity of flu illness. September and October are ideal times to get vaccinated; however, if flu viruses are circulating, vaccination should continue. To avoid missed opportunities for vaccination, providers should offer vaccination during routine health care visits and hospitalizations. Flu vaccines and COVID-19 vaccines, including the updated bivalent COVID-19 booster vaccine, can be given at the same appointment1.
For this report, CDC analyzed data from the NIS-Flu for children 6 months through 17 years and the BRFSS for adults ≥18 years to estimate national- and state-level flu vaccination coverage for the 2021–22 flu season. The analyses included data collected from interviews completed from September 2021 for BRFSS and October 2021 for NIS-Flu through June 2022 for vaccinations received between July 1, 2021, and the time of interview or by May 31, 2022, for those interviewed in June 2022.
The NIS-Flu is a national random-digit-dialed cellular telephone survey of households2. Respondents ≥18 years knowledgeable about the child's vaccinations (hereafter referred to as "parent" in this report) were asked if their child received a flu vaccination since July 1, 2021, and the month of vaccination; this information was not verified by medical records. Month of vaccination was missing for 19.1% of respondents who indicated their child was vaccinated. For these children, month was imputed using the hot-deck imputation method from other survey respondents who matched the week of interview, age group, state of residence, and race/ethnicity of the child with missing data. Respondents who indicated the child received a flu vaccination were asked the place where the child was vaccinated. The range of the Council of American Survey and Research Organizations (CASRO) response rates for the NIS-Flu for the 2021–22 season was 21.1%–25.0%. The estimates for children are based on n=158,146 completed NIS-Flu interviews.
The BRFSS is a state-based random-digit-dialed cellular and landline telephone survey that collects information on various health conditions and risk behaviors from one randomly selected adult ≥18 years in a household. The BRFSS survey asks if the respondent has received a flu vaccine in the past 12 months and, if so, the month and year of vaccination. Respondents who did not answer yes or no to the question about flu vaccination in the past 12 months were excluded from the analysis. This included 0.5% who reported they did not know, 0.3% who refused to answer, and 8.0% who most likely ended the interview before the flu question was asked. For 9.8% of BRFSS participants who were vaccinated but had a missing month or year of vaccination, month and year were imputed using the hot-deck imputation method from other survey respondents who matched the week of the interview, age group, state of residence, and race/ethnicity of the respondent with missing data. Information on high-risk conditions was missing for 1.5% of adults; these respondents were not included in the estimates by risk condition. Estimates are not available for the entire 2021–22 flu season for California because interview data for January–June 2022 from California were not available; therefore, California estimates represent vaccinations received only through November 2021 and not through May 2022 as for other states. In addition, estimates for adults living in Florida were based on interviews from January through June because interview data for September–December 2021 from Florida were not available; however, vaccinations received through May 2022 could be estimated for Florida. The median state BRFSS response rate for a complete or partially complete interview was 42.5% for September–December 2021 and 45.4% for January–June 2022. The estimates for adults are based on n=291,839 completed BRFSS interviews.
Flu vaccination coverage estimates from both the surveys were calculated using Kaplan-Meier survival analysis using the month of the reported flu vaccination to determine cumulative flu vaccination coverage. Coverage estimates for all persons ≥6 months were determined by combining the state-level monthly NIS-Flu and BRFSS estimates weighted by the age-specific populations of each state3. All estimates were weighted and analyzed using SAS and SAS-callable SUDAAN statistical software to account for the complex survey designs. For simplified graphical display, only four racial/ethnic groups are displayed (Hispanic, White only, non-Hispanic (White), Black only, non-Hispanic (Black), and other or multiple races, non-Hispanic (other/multiple)); a link to a supplemental table that includes a more detailed racial/ethnic breakdown of estimates can be found in the "Additional Flu Vaccination Coverage Estimates" section at the end of the report. Differences between groups and between 2021–22 and prior season (2020–21) estimates were determined using t-tests with significance at p<0.05. Increases or decreases noted in this report were statistically significant differences.
Results
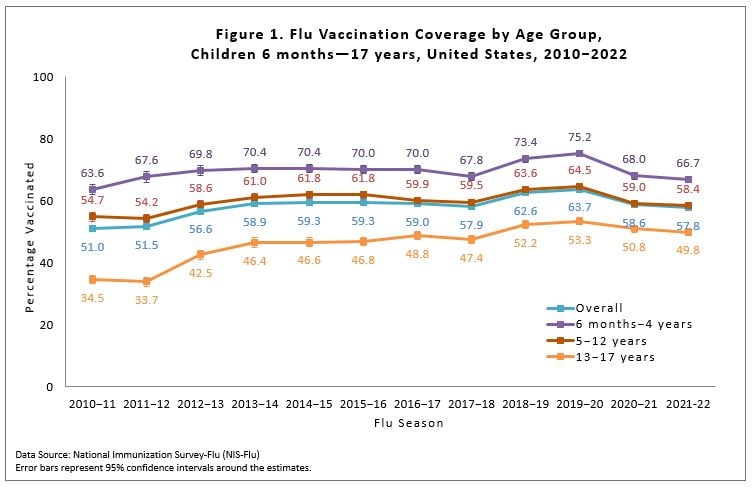
Among children 6 months through 17 years, the percentage receiving ≥1 dose of flu vaccine during the 2021–22 season was 57.8%, 0.8 percentage points lower than coverage in the 2020–21 season (58.6%; Figure 1).
Flu vaccination coverage among children aged 6 months–4 years (66.7%), 5–12 years (58.4%), and 13–17 years (49.8%) did not significantly differ from coverage in the previous season (Figure 1). However, for children aged 6–23 months (70.3%), flu vaccination coverage decreased 2.4 percentage points compared with the previous season (72.7%) [see additional table].
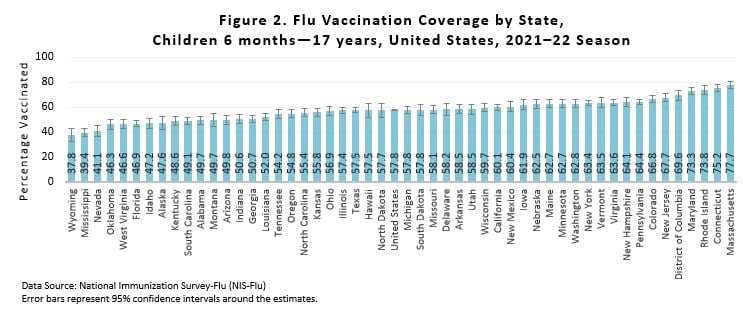
There was wide between-state variability in flu vaccination coverage among children, ranging from 37.8% (Wyoming) to 77.7% (Massachusetts); (Figure 2). See the interactive FluVaxView application for additional state-level estimates by age groups and multiple flu seasons.
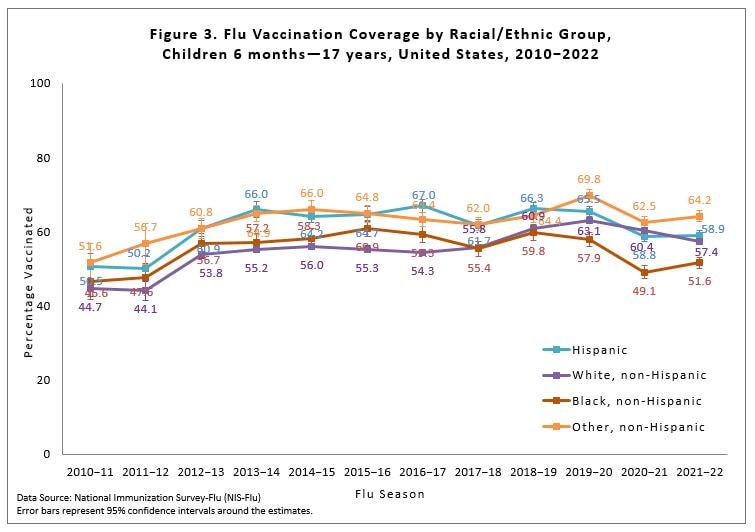
Flu vaccination coverage for the 2021–22 season was 3.0 percentage points lower among White children compared with the 2020–21 season and was 2.5 percentage points higher for Black children. Coverage for Hispanic children and children of other or multiple races did not change compared with the previous season (Figure 3). Children of other/multiple races had higher flu vaccination coverage than Black, White, and Hispanic children. Hispanic children had higher coverage than White and Black children. Black children had lower coverage than White children. No other statistically significant pair-wise differences were observed. Flu vaccination coverage estimates for more detailed racial/ethnic groups (Asian, American Indian/Alaska Native) are provided as a table weblink in the "Additional Flu Vaccination Coverage Estimates" section of this report.
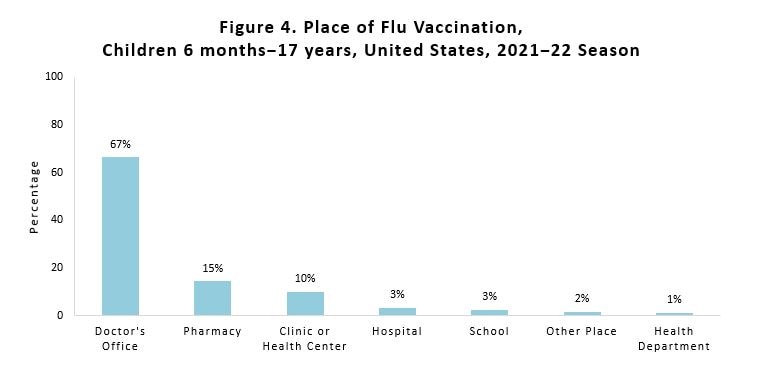
Place of flu vaccination among vaccinated children 6 months through 17 years was most often a doctor's office (67%), followed by a pharmacy (15%), and clinic/health center (10%) (Figure 4). Place of flu vaccination by child age groups can be found in the "Additional Flu Vaccination Coverage Estimates" section of this report.
Overall, among adults ≥18 years, flu vaccination coverage was 49.4%, 0.8 percentage points lower than coverage during the 2020–21 season (50.2%; Figure 5) and 1.0 percentage points higher than during the 2019-20 season (48.4%).
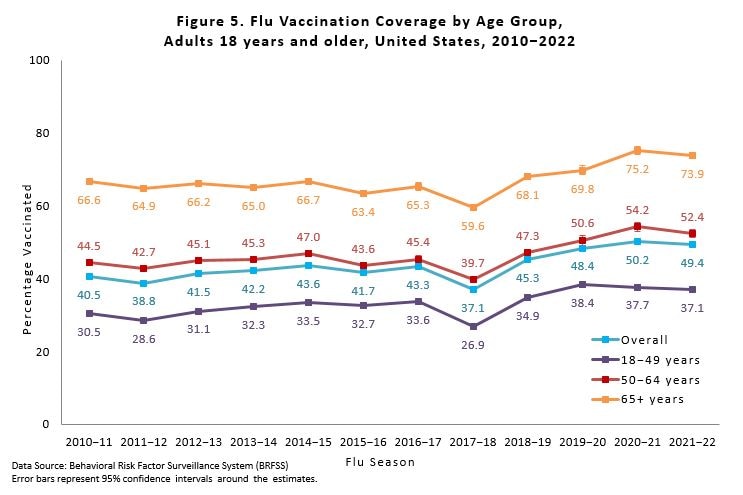
Flu vaccination coverage for 2021–22 was 1.8 percentage points lower for adults 50–64 years and 1.3 percentage points lower for adults ≥65 years; coverage did not change among adults 18–49 years compared with the 2020–21 season (Figure 5). Compared to two seasons prior (2019–20), a pre-pandemic season, flu vaccination coverage during 2021–22 was 1.3 percentage points lower for adults 18–49 years, 1.8 percentage points higher for adults aged 50–64 years, and 4.1 percentage points higher for adults aged ≥65 years.
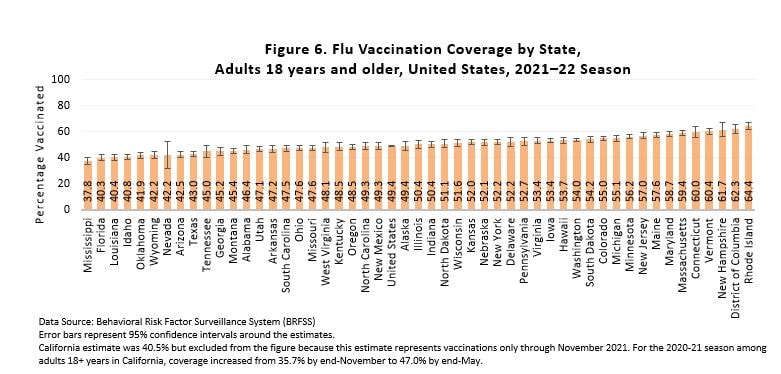
There was wide between-state variability in flu vaccination coverage among adults, ranging from 37.8% in Mississippi to 64.4% in Rhode Island (Figure 6). See the interactive FluVaxView application for additional state-level estimates by age-groups and multiple flu seasons.
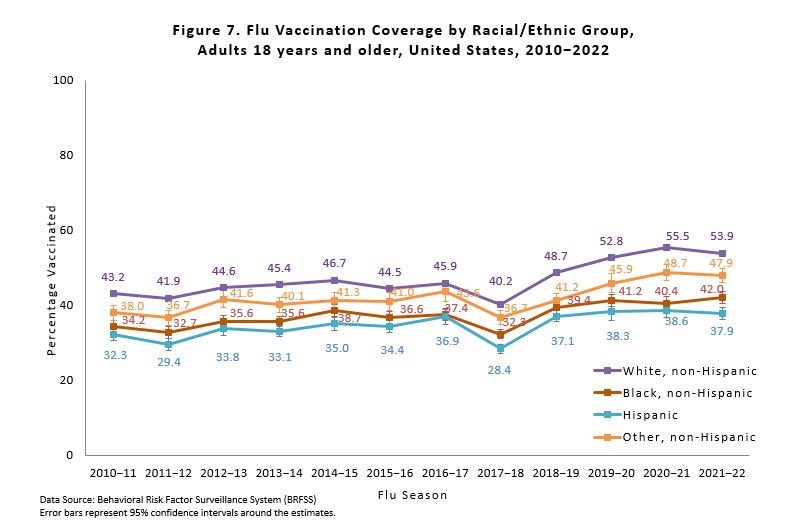
Flu vaccination coverage for Black, Hispanic, and adults of other or multiple races during the 2021–22 season did not differ compared with the 2020–21 season, while White adults had a 1.6 percentage point decrease in coverage (Figure 7). White adults had higher flu vaccination coverage than Black, Hispanic, and adults of other or multiple races. Additionally, Hispanic, and Black adults had lower flu vaccination coverage than adults of other or multiple races. Black adults had higher coverage than Hispanic adults. No other differences were observed. Flu vaccination coverage estimates for more detailed racial/ethnic groups (Asian, American Indian/Alaska Native) are provided as a table weblink in the "Additional Flu Vaccination Coverage Estimates" section at the end of this report.
Flu vaccination coverage among all people ≥6 months during the 2021–22 season was 51.4%, 0.7 percentage points lower than coverage in the 2020–21 season (52.1%; Table 1). Coverage during the 2021–22 season decreased by 1.8 percentage points for White people (Table 1). White people had higher flu coverage than Black, Hispanic, and people of other or multiple races. Additionally, people of other or multiple races had higher coverage than Black and Hispanic people. No other differences were observed.
Table 1. Flu Vaccination Coverage* among All People 6 months and older, by Race/Ethnicity, United States,† 2021–22 Season
| Race/Ethnicity‡ | %§ ± 95% CI|| | Difference from the 2020–21 Season ± 95% CI |
|---|---|---|
| Overall | 51.4 ± 0.3 | -0.7 ± 0.6¶ |
| White only, non-Hispanic | 54.6 ± 0.5 | -1.8 ± 0.7¶ |
| Black only, non-Hispanic | 44.5 ± 1.2 | 1.8 ± 1.8 |
| Hispanic | 45.0 ± 1.1 | 0.1 ± 1.7 |
| Other, non-Hispanic** | 52.5 ± 1.3 | 0.4 ± 2.1 |
* Estimates of the percentage vaccinated are based on interviews conducted September (BRFSS) or October (NIS-Flu) 2021 through June 2022 and reported vaccinations from July 2021 through May 2022.
† Excludes U.S. territories.
‡ Race is self-reported; people of Hispanic ethnicity may be of any race.
§ Percentage vaccinated. Percentages are weighted to the U.S. population. Month of vaccination was imputed for respondents with missing month of vaccination data.
|| Confidence interval (CI) half-widths.
¶ Statistically significant difference between the 2021–22 season and the 2020–21 season by t-test (p<0.05).
** Includes Asian, American Indian/Alaska Native, Native Hawaiian or other Pacific Islander, multiracial, and other races.
Children:
- Flu Vaccination Coverage, by Age Group, Children, United States, 2021–22 Season [12 KB]
- Flu Vaccination Coverage by Sex, Children, United States, 2021–22 Season [14 KB]
- Flu Vaccination Coverage by Race/Ethnicity and Age Group, Children, United States, 2021–22 Season [15 KB]
- Flu Vaccination Coverage for Local Areas and Territories, Children, 2021–22 Season [65 KB]
- Place of Flu Vaccination by Age Group, Children, United States, 2021–22 Season [16 KB]
Adults:
- Flu Vaccination Coverage, by Age Group and High Risk Status, Adults, United States, 2021–22 Season [12 KB]
- Flu Vaccination Coverage by Sex, Adults, United States, 2021–22 Season [14 KB]
- Flu Vaccination Coverage by Race/Ethnicity and Age Group, Adults, United States, 2021–22 Season [16 KB]
- Flu Vaccination Coverage for Local Areas and Territories, Adults, 2021–22 Season [45 KB]
Limitations
Several limitations of the estimates produced from the NIS-Flu and BRFSS surveys should be considered when interpreting the results in this report. First, survey weighting adjustments may not eliminate all the possible bias from incomplete sample frames; both surveys exclude households with no telephones, and NIS-Flu excludes households with only landline telephones. Second, response rates for both surveys were low, and flu vaccination coverage may differ between survey respondents and non-respondents; survey weighting adjustments may not adequately control these differences. Third, there may be flu vaccination status errors due to recall errors of parents for NIS-Flu and of respondents for BRFSS45. Fourth, errors from incomplete sample frame, nonresponse, and accuracy of reported flu vaccination status might change over time, leading to inaccurate assessment of trends in flu vaccination coverage. Fifth, due to BRFSS interview data not being available for all months from California, estimates for California represent vaccination coverage through November rather than through May. Sixth, estimates based on the sources in this report have differed from National Health Interview Survey (NHIS) estimates6. NHIS, the data source for evaluating progress toward the Healthy People 2030 flu vaccination coverage objectives, uses a different sampling method than the NIS-Flu and BRFSS, and uses in-person interviews but also relies on self or parental report. A recent study found that NIS-Flu estimates were generally higher than NHIS estimates over several flu seasons for children6. CDC continues to assess consistency between flu vaccination coverage estimates from different surveys and other data sources and to evaluate the accuracy of estimates from these data sources.
Discussion
Flu vaccination coverage during the 2021–22 season was lower than coverage during the 2020–21 season for both children and adults. Following the COVID-19 pandemic, coverage among children markedly decreased in the 2020-21 season after increases had been observed in the two prior seasons78. This decrease in flu vaccination is consistent with decreases in coverage for routine childhood vaccinations that have been documented since the start of the COVID-19 pandemic910. While a smaller decrease was observed in the 2021-22 season, coverage among children continues to be below pre-pandemic levels. In contrast to children, flu vaccination coverage among adults increased in 2020-21, the season immediately following the start of the COVID-19 pandemic. While coverage decreased slightly between 2020-21 and 2021-22, coverage remains above pre-pandemic levels in adults aged ≥50 years. Coverage has decreased slightly since the 2019-20 season among adults aged 18–49. Coverage among adults is still nearly 20 percentage points lower than the Healthy People 2030 national target of 70% for flu vaccination of persons ≥6 months; coverage among children is lagging by approximately 12 percentage points. Flu vaccination coverage varies by state, with some states having coverage more than 30 percentage points below the national target. Racial/ethnic disparities in vaccination persist.
CDC recommends that everyone 6 months and older get a yearly flu vaccine, with rare exceptions, to protect themselves, their loved ones, and community against flu1. During the 2022–23 flu season, flu and SARS-CoV-2 (the virus that causes COVID-19) will likely be spreading in the United States at the same time. Flu vaccines will not protect against COVID-19 but have been shown to reduce the risk of flu illness, hospitalization, and death, and, thus, can help reduce the burden on the health care system and conserve potentially scarce health care resources during the ongoing COVID-19 pandemic. Vaccinating people at higher risk, including those with a chronic condition like a breathing or lung problem, heart disease, or a weakened immune system, is a critical strategy to help decrease their risk of severe flu illness. Many people at higher risk from flu complications also are at higher risk from COVID-19.
Health care providers should use every opportunity during the flu season to administer flu vaccines to all eligible persons; COVID-19 vaccines may be administered without regard to timing of other vaccines1. September and October are ideal times to get vaccinated; however, vaccination should continue as long as flu viruses are circulating. For the 2022–23 season, vaccine manufacturers have projected they will provide as many as 173.5–183.5 million doses of flu vaccine11.
- Grohskopf LA, Blanton LH, Ferdinands JM, et al. Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices — United States, 2022–23 Influenza Season. MMWR Recomm Rep 2022;71(No. RR-1):1–28. DOI: http://dx.doi.org/10.15585/mmwr.rr7101a1
- Wolter, K. K., Smith, P. J., Khare, M., Welch, B., Copeland, K. R., Pineau, V. J., & Davis, N. (2017). Statistical Methodology of the National Immunization Survey, 2005-2014. Vital Health Stat 1(61), 1-107.
- Furlow-Parmley, C., Singleton, J. A., Bardenheier, B., & Bryan, L. (2012). Combining estimates from two surveys: an example from monitoring 2009 influenza A (H1N1) pandemic vaccination. Stat Med, 31(27), 3285-3294. https://doi.org/10.1002/sim.5333.
- Brown, C., Clayton-Boswell, H., Chaves, S. S., Prill, M. M., Iwane, M. K., Szilagyi, P. G., Edwards, K. M., Staat, M. A., Weinberg, G. A., Fairbrother, G., Hall, C. B., Zhu, Y., & Bridges, C. B. (2011). Validity of parental report of influenza vaccination in young children seeking medical care. Vaccine, 29(51), 9488-9492. https://doi.org/10.1016/j.vaccine.2011.10.023.
- Irving, S.A., et al., Evaluation of self-reported and registry-based influenza vaccination status in a Wisconsin cohort. Vaccine, 2009. 27(47): p. 6546-9.
- Santibanez, T. A., Srivastav, A., Zhai, Y., & Singleton, J. A. (2020). Trends in Childhood Influenza Vaccination Coverage, United States, 2012-2019. Public Health Rep, 135(5), 640-649. https://doi.org/10.1177/0033354920944867
- https://www.cdc.gov/fluvaxview/coverage-by-season/2020-2021.html
- https://www.cdc.gov/fluvaxview/coverage-by-season/vaccination-2019-2020.html
- Pingali C, Yankey D, Elam-Evans LD, et al. National Vaccination Coverage Among Adolescents Aged 13–17 Years — National Immunization Survey-Teen, United States, 2021. MMWR Morb Mortal Wkly Rep 2022;71:1101–1108. DOI: http://dx.doi.org/10.15585/mmwr.mm7135a1
- Patel B, Murthy , Zell E, et al. Impact of the COVID-19 Pandemic on Administration of Selected Routine Childhood and Adolescent Vaccinations — 10 U.S. Jurisdictions, March–September 2020. MMWR Morb Mortal Wkly Rep 2021;70:840–845. DOI: http://dx.doi.org/10.15585/mmwr.mm7023a2
- Seasonal Influenza Vaccine Supply for the U.S. 2022-2023 Influenza Season. https://www.cdc.gov/flu/prevent/vaxsupply.htm.