|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
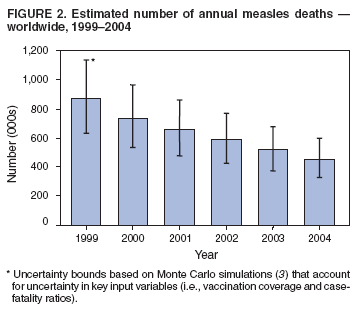
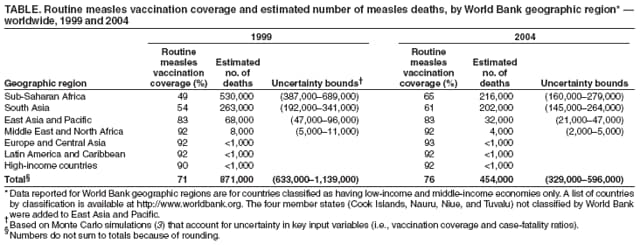
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress in Reducing Global Measles Deaths, 1999--2004Measles remains a substantial cause of global childhood mortality, particularly in developing countries. In their joint strategic plan for Measles Mortality Reduction, 2001--2005, the World Health Organization (WHO) and the United Nations Children's Fund (UNICEF) targeted 45 priority countries* (Figure 1) with the highest measles mortality for implementation of a comprehensive strategy for accelerated and sustained measles mortality reduction (1). Components of this strategy include achieving high routine vaccination coverage (>90%) in every district and ensuring that all children receive a second opportunity for measles vaccination. In May 2003, the World Health Assembly endorsed a resolution urging member countries to achieve a goal (adopted in 2002 by the United Nations General Assembly Special Session on Children) to reduce 1999 deaths resulting from measles by half by the end of 2005. This report updates progress toward this goal and introduces a new goal for measles mortality reduction by 2010. Immunization ActivitiesBy July of each year, all countries are asked to submit information on measles vaccination coverage from the previous year using the WHO/UNICEF Joint Reporting Form. Estimates of routine coverage with 1 dose of measles vaccine are based on review of coverage data from administrative records, surveys, national reports, and consultation with local and regional experts. Coverage achieved during nationwide supplementary immunization activities (SIAs) against measles are reported on the basis of the reported number of doses administered, divided by the target population. WHO/UNICEF estimates indicate that global routine measles vaccination coverage increased from 71% in 1999 to 76% in 2004. Coverage varied significantly by geographic region† (Table). Substantial increases in routine coverage were evident in Sub-Saharan Africa (from 49% to 65%) and South Asia (54% to 61%). Moreover, an increase has occurred in the proportion of countries offering children a second opportunity for measles vaccination, through either SIAs or routine services. During 2004, a total of 168 (88%) countries offered children a second opportunity, compared with 150 (78%) countries in 2001. During 2000--2004, SIAs were offered in 36 of the 45 priority countries; 28 (78%) of these SIAs were nationwide and 24 (67%) were in Sub-Saharan Africa (Figure 1). Of the SIAs in Sub-Saharan Africa, 18 (75%) were nationwide. Of the 232 million (93%) children aged 9 months--14 years targeted to receive measles vaccine through these SIAs, an estimated 215 million (93%) were vaccinated. Mortality EstimatesAnnual estimates of global measles deaths were generated for the years 1999 through 2004 using the same method used to calculate 1999--2003 estimates of measles deaths (2). Data sources included updates to information on both historical and 2004 measles vaccination coverage (including both routine and SIAs) and 2004 United Nations population estimates (including updates for 1999--2004). Results from surveillance data combined with the natural history model§ indicate that overall global measles mortality decreased 48%, from 871,000 deaths (uncertainty bounds¶: 633,000--1,139,000) in 1999 to 454,000 deaths (uncertainty bounds: 329,000--596,000) in 2004 (Table, Figure 2). The largest percentage reduction during this period (59%) was in Sub-Saharan Africa, followed by East Asia and the Pacific (52%) and the Middle East and North Africa (50%). Reported by: Dept of Immunization, Vaccines, and Biologicals, WHO, Geneva, Switzerland. UNICEF, New York, New York. Global Immunization Div, National Immunization Program, CDC. Editorial Note:During 1999--2004, improvements in routine measles vaccination coverage and implementation of measles SIAs in the 45 priority countries targeted by the WHO/UNICEF joint strategic plan have resulted in a 48% decrease in the estimated number of global measles deaths. Worldwide, since 1999, an estimated 500 million persons have received measles vaccine through SIAs, and an estimated 1.4 million measles deaths have been averted as a result of implementing the strategy of improving routine vaccination coverage with the first dose along with providing a second opportunity for measles vaccination. The largest decrease in estimated measles deaths (59%) was seen in Sub-Saharan Africa. The reduction in South Asia (23%) was smaller because certain large countries had not yet begun large-scale measles SIAs by the end of 2004. If global progress has continued at the rates achieved in recent years, data for 2005 likely will reveal that the 2005 measles mortality reduction goal was met. The mortality estimates based on the natural history model have been corroborated by data from countries that have fully implemented recommended vaccination strategies and strengthened measles surveillance. An analysis of the effect of intensified vaccination efforts in 19 African countries observed a 92% reduction in reported measles cases; only one country (Burkina Faso) experienced a large outbreak after an SIA. This outbreak resulted, in part, from large-scale population migration caused by civil unrest in neighboring Côte d'Ivoire. Both disease surveillance and mathematical models have been used to monitor progress towards the 2005 measles mortality reduction goal. Models are limited by their assumptions and the lack of current information for key parameters such as proportional cause-specific mortality or measles case-fatality ratios. Emphasis on strengthening surveillance as a key strategy for measles mortality reduction has led to improvement in reporting measles cases by countries. During 2004, a total of 190 countries reported on measles cases through the WHO/UNICEF joint reporting form, compared with 174 countries during 2003 and 166 countries during 1999. However, strengthening disease surveillance and registration of cause-specific mortality continue to be needed in many developing countries. While better health information systems are being developed, models remain useful for monitoring and directing program activities. Support of the Measles Initiative has been a key factor contributing to progress in reducing measles mortality. Begun in 2001, the Measles Initiative is a partnership formed to sustainably reduce the number of deaths from measles.** The Measles Initiative serves an important role in providing technical and financial support to priority countries and in strengthening political and social commitment in the fight against measles. The Measles Initiative is led by the American Red Cross, United Nations Foundation, CDC, WHO, UNICEF, and the Canadian International Development Agency. During 2000--2004, the Measles Initiative supported approximately 40 African countries in implementing high-quality measles SIAs. Because the 2005 measles mortality reduction goal likely was met on schedule (final 2005 data will not be available until 2007), a more ambitious goal has been proposed in the Global Immunization Vision and Strategy (GIVS).†† The new goal calls for a 90% reduction in measles mortality by 2010 compared with the 2000 level. However, major challenges exist to achieving this new goal. First, measles mortality reduction activities need to be successfully implemented in several large countries with high measles burden (e.g., India, Nigeria, and Pakistan). Second, to sustain the gains in reduced measles deaths in the 45 priority countries, vaccination systems need to be improved to ensure that >90% of infants are vaccinated against measles through routine health services before their first birthday. Third, priority countries will need to conduct follow-up SIAs every 3--4 years until their routine vaccination systems are capable of providing two opportunities for measles vaccination to >90% of every birth cohort. Fourth, disease surveillance systems at district, provincial, and national levels need to be strengthened to enable case-based surveillance with testing of clinical specimens from suspected cases in laboratories participating in the global measles and rubella laboratory network (4). Finally, measles case management, including appropriate vitamin A supplementation, should be strengthened. References
* Afghanistan, Angola, Bangladesh, Benin, Burkina Faso, Burundi, Cambodia, Cameroon, Central African Republic, Chad, Congo, Côte d'Ivoire, Democratic Republic of the Congo, Djibouti, Equatorial Guinea, Eritrea, Ethiopia, Gabon, Ghana, Guinea, Guinea-Bissau, India, Indonesia, Kenya, Lao People's Democratic Republic, Liberia, Madagascar, Mali, Mozambique, Myanmar, Nepal, Niger, Nigeria, Pakistan, Papua New Guinea, Rwanda, Senegal, Sierra Leone, Somalia, Sudan, Togo, Uganda, United Republic of Tanzania, Vietnam, and Zambia. † Data reported for World Bank geographic regions are for countries classified as having low-income and middle-income economies only. A list of countries by classification is available at http://www.worldbank.org. Four member states (Cook Islands, Nauru, Niue, and Tuvalu) not classified by World Bank were added to East Asia and Pacific. § Incorporates historical figures with population data that are annually updated. ¶ Based on Monte Carlo simulations (3) that account for uncertainty in key input variables (i.e., vaccination coverage and case-fatality ratios). ** Additional information is available at http://www.measlesinitiative.org. †† Developed by WHO and UNICEF for the period 2006--2015. Additional information is available at http://www.who.int/vaccines/givs . Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 3/9/2006 |
|||||||||
|