 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress in Reducing Measles Mortality --- Worldwide, 1999--2003Measles remains an important cause of childhood mortality, especially in developing countries. In the joint Strategic Plan for Measles Mortality Reduction, 2001--2005, the World Health Organization (WHO) and the United Nations Children's Fund (UNICEF) targeted 45 priority countries* with high measles burden for implementation of a comprehensive strategy for accelerated and sustained measles mortality reduction (1). Components of this strategy include achieving high routine vaccination coverage (>90%) in every district and ensuring that all children receive a second opportunity for measles immunization. In May 2003, the World Health Assembly endorsed a resolution urging member countries to reduce deaths attributed to measles by half (compared with 1999 estimates) by the end of 2005 (2). This report updates progress toward this goal and summarizes recent recommendations on methods to estimate global measles mortality. Vaccination ActivitiesBy July of each year, all countries are requested to submit information on measles vaccination coverage from the previous year using the WHO/UNICEF Joint Reporting Form. Estimates of routine coverage with 1 dose of measles vaccine among children aged 1 year are based on review of coverage data from administrative records, surveys, national reports, and consultation with local and regional experts (3). Coverage achieved during nationwide supplementary immunization activities (SIAs) against measles are reported on the basis of tally sheets of the number of doses administered divided by the target population. On the basis of WHO/UNICEF estimates, global routine measles vaccination coverage among children aged 1 year increased from 71% in 1999 to 77% in 2003. Coverage varied substantially by region (Table). Moreover, an increase was observed in the proportion of countries offering children a second opportunity for measles immunization. In 2003, a total of 164 (85%) countries offered children a second opportunity, compared with 150 (78%) countries in 2001. During 2000--2003, approximately 197 million children received measles vaccination through "catch-up" and "follow-up" SIAs in 30 of the 45 priority countries (Figure 1). Of the 30 countries that conducted measles SIAs during this period, 23 (77%) were nationwide and 23 (77%) were in the African Region. Median reported coverage for these SIAs was 98% (range: 65%--99%). Mortality EstimatesBecause of limited disease surveillance and death registration in many countries with weak infrastructure and high measles burden, current routine reporting systems are inadequate for monitoring global measles mortality. Different modeling approaches have been used to estimate the global number of measles deaths (4,5). Published estimates from these approaches vary both in level and precision and have wide uncertainty bounds that overlap. A panel of six experts was convened in January 2005 to advise WHO on how best to monitor progress toward the 2005 measles mortality reduction goal. The panel noted strengths and weaknesses in various approaches to estimating measles mortality but endorsed the use of surveillance data (where they are reliable) and a natural history model (where surveillance data are unreliable) because the latter accounts for recent changes in vaccination coverage and is therefore better suited for monitoring trends. However, the panel recommended that uncertainty bounds around the point estimates be calculated to indicate the lack of precision. On the basis of results from the natural history model, overall global measles mortality decreased 39%, from 873,000 deaths (uncertainty bounds†: 645,000--1,196,000 deaths) in 1999 to 530,000 deaths (bounds: 383,000--731,000 deaths) in 2003 (Table; Figure 2). The largest reduction was in Africa, where estimated measles mortality decreased by 46% during this period. Reported by: Dept of Immunization, Vaccines, and Biologicals, World Health Organization, Geneva, Switzerland. United Nations Children's Fund, New York, New York. Global Immunization Div, National Immunization Program, CDC. Editorial Note:Improvements in routine measles vaccination coverage and implementation of measles SIAs in 30 of the 45 priority countries have substantially decreased the estimated number of global measles deaths. Although difficult to quantify, the widespread use of vitamin A through polio and measles SIAs and routine services has also likely contributed to the reduction of measles mortality. If progress continues at the rates achieved in recent years, the 2005 measles mortality reduction goal likely will be met. The mortality estimates based on the natural history model have been corroborated by surveillance data from countries that have fully implemented the recommended vaccination strategies; an analysis of the impact of intensified vaccination efforts in 19 African countries indicated that a 92% reduction in reported measles cases occurred and that only one country (Burkina Faso) experienced a large outbreak after the SIA (WHO, Regional Office for Africa, unpublished data, 2005). This outbreak was attributed to large-scale population migration as a result of civil unrest in neighboring Côte d'Ivoire. Both disease surveillance and mathematical models have been used to monitor progress toward the 2005 measles mortality reduction goal. The models are limited by their assumptions, overlapping and wide uncertainty bounds, and the lack of current information for key parameters, such as proportional cause-specific mortality or measles case-fatality ratios. As in polio-eradication programs, case-based surveillance with laboratory confirmation of suspected cases should be the "gold standard" for measuring program impact. Investments in strengthening disease surveillance and registration of cause-specific mortality are urgently needed in many developing countries. In the interim, while these health information systems are being developed, models remain useful for monitoring and directing program activities. More field studies of the natural history of measles, especially documenting the case-fatality in high-burden settings and the proportional mortality attributed to measles in similar settings, are needed to update model estimates. A key factor contributing to progress in reducing measles mortality in Africa has been the support of the Africa Measles Initiative. This partnership, which was formed in 2001 and spearheaded by the American Red Cross, CDC, UNICEF, WHO, and the United Nations Foundation, has played a critical role in supporting African countries in their measles mortality reduction efforts. Since 2001, this partnership has mobilized $144 million, which has resulted in the vaccination of approximately 150 million African children against measles. Major challenges remain in reaching the 2005 measles mortality reduction goal (7). First, measles mortality reduction activities need to be implemented in several large countries with high measles burden, such as Nigeria, India, and Pakistan. Second, to sustain the gains in reduced measles deaths in the 45 priority countries, enhanced efforts are needed to improve immunization systems to ensure that >90% of infants are vaccinated against measles before their first birthdays. Finally, the priority countries will need to continue to conduct follow-up SIAs every 3--4 years until their routine vaccination systems are capable of providing two opportunities for measles immunization to a very high proportion (i.e., >90%) of every birth cohort. References
* Afghanistan, Angola, Bangladesh, Benin, Burkina Faso, Burundi, Cambodia, Cameroon, Central African Republic, Chad, Congo, Côte d'Ivoire, Democratic Republic of the Congo, Djibouti, Equatorial Guinea, Eritrea, Ethiopia, Gabon, Ghana, Guinea, Guinea-Bissau, India, Indonesia, Kenya, Lao People's Democratic Republic, Liberia, Madagascar, Mali, Mozambique, Myanmar, Nepal, Niger, Nigeria, Pakistan, Papua New Guinea, Rwanda, Senegal, Sierra Leone, Somalia, Sudan, Togo, Uganda, United Republic of Tanzania, Viet Nam, and Zambia. † Based on Monte Carlo simulations (6) that account for uncertainty in key input variables (i.e., vaccination coverage and case-fatality ratios). Figure 1  Return to top. Figure 2 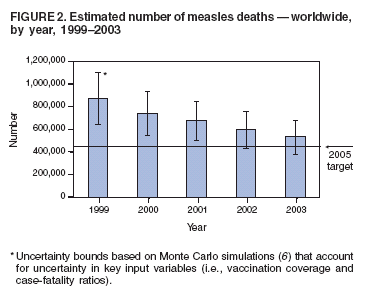 Return to top. Table  Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 3/3/2005 |
|||||||||
This page last reviewed 3/3/2005
|