Please note:
An
erratum has been published for this article. To view the erratum, please
click here.
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Guidelines for Environmental Infection Control in
Health-Care Facilities
Recommendations of CDC and the Healthcare Infection Control
Practices Advisory Committee (HICPAC)
Prepared by
Lynne Sehulster, Ph.D.1
Raymond Y.W. Chinn, M.D.2 1Division of Healthcare Quality Promotion
National Center for Infectious Diseases 2HICPAC member
Sharp Memorial Hospital
San Diego, California
The material in this report originated in the National Center for Infectious Diseases, James M. Hughes, M.D., Director; and the Division of Healthcare Quality Promotion, Steven L. Solomon, M.D., Acting Director.
Summary
The health-care facility environment is rarely implicated in disease transmission, except among patients who
are immunocompromised. Nonetheless, inadvertent exposures to environmental pathogens (e.g.,
Aspergillus spp. and Legionella spp.) or airborne pathogens (e.g.,
Mycobacterium tuberculosis and varicella-zoster virus) can result in adverse
patient outcomes and cause illness among health-care workers. Environmental infection-control strategies and engineering controls can effectively prevent these infections. The incidence of health-care--associated infections and pseudo-outbreaks can be minimized by 1) appropriate use of cleaners and disinfectants; 2) appropriate maintenance of medical equipment (e.g.,
automated endoscope reprocessors or hydrotherapy equipment); 3) adherence to water-quality standards for hemodialysis, and to ventilation standards for specialized care environments (e.g., airborne infection isolation rooms, protective environments, or operating rooms); and 4) prompt management of water intrusion into the facility. Routine environmental sampling is not
usually advised, except for water quality determinations in hemodialysis settings and other situations where sampling is directed by epidemiologic principles, and results can be applied directly to infection-control decisions.
This report reviews previous guidelines and strategies for preventing environment-associated infections in health-care facilities and offers recommendations. These include 1) evidence-based recommendations supported by studies; 2) requirements of federal agencies (e.g., Food and Drug Administration, U.S. Environmental Protection Agency, U.S. Department of
Labor, Occupational Safety and Health Administration, and U.S. Department of Justice); 3) guidelines and standards from
building and equipment professional organizations (e.g., American Institute of Architects, Association for the Advancement of
Medical Instrumentation, and American Society of Heating, Refrigeration, and Air-Conditioning Engineers); 4)
recommendations derived from scientific theory or rationale; and 5) experienced opinions based upon infection-control and engineering practices. The report also suggests a series of performance measurements as a means to evaluate infection-control efforts.
Introduction
Parameters of the Report
This report, which contains the complete list of recommendations with pertinent references, is Part II of Guidelines for Environmental Infection Control in Health-Care Facilities.
The full four-part guidelines will be available on CDC's Division
of Healthcare Quality Promotion (DHQP) website. Relative to previous CDC guidelines, this report
revises multiple sections (e.g., cleaning and disinfection of environmental surfaces, environmental sampling, laundry and bedding, and regulated medical waste) from previous editions of CDC's
Guideline for Handwashing and Hospital Environmental
Control;
incorporates discussions of air and water environmental concerns from CDC's
Guideline for Prevention of Nosocomial
Pneumonia;
consolidates relevant environmental infection-control measures from other CDC guidelines; and
includes two topics not addressed in previous CDC guidelines --- infection-control concerns related to animals in
health-care facilities and water quality in hemodialysis settings.
In the full guidelines, Part I, Background Information: Environmental Infection Control in Health-Care Facilities, provides
a comprehensive review of the relevant scientific literature. Attention is given to engineering and infection-control
concerns during construction, demolition, renovation, and repair of health-care facilities. Use of an infection-control risk assessment is strongly supported before the start of these or any other activities expected to generate dust or water aerosols. Also reviewed
in Part I are infection-control measures used to recover from catastrophic events (e.g., flooding, sewage spills, loss of electricity and ventilation, or disruption of water supply) and the limited effects of environmental surfaces, laundry, plants,
animals, medical wastes, cloth furnishings, and carpeting on disease transmission in health-care facilities. Part III and Part IV of the full guidelines provide references (for the complete guideline) and appendices, respectively.
Part II (this report) contains recommendations for environmental infection control in health-care facilities,
describing control measures for preventing infections associated with air, water, or other elements of the environment. These recommendations represent the views of different divisions within CDC's National Center for Infectious Diseases and the Healthcare Infection Control Practices Advisory Committee (HICPAC), a 12-member group that advises CDC on
concerns related to the surveillance, prevention, and control of health-care--associated infections, primarily in U.S. health-care facilities. In 1999, HICPAC's infection-control focus was expanded from acute-care hospitals to all venues where health care is
provided (e.g., outpatient surgical centers, urgent care centers, clinics, outpatient dialysis centers, physicians' offices, and skilled nursing facilities). The topics addressed in this report are applicable to the majority of health-care facilities in the United States. This report is intended for use primarily by infection-control practitioners, epidemiologists, employee health and safety
personnel, engineers, facility managers, information systems professionals, administrators, environmental service professionals, and architects. Key recommendations include
infection-control impact of ventilation system and water system performance;
establishment of a multidisciplinary team to conduct infection-control risk assessment;
use of dust-control procedures and barriers during construction, repair, renovation, or demolition;
environmental infection-control measures for special areas with patients at high risk;
use of airborne-particle sampling to monitor the effectiveness of air filtration and dust-control measures;
procedures to prevent airborne contamination in operating rooms when infectious tuberculosis (TB) patients
require surgery;
guidance regarding appropriate indications for routine culturing of water as part of a comprehensive control program
for legionellae;
guidance for recovering from water-system disruptions, water leaks, and natural disasters (e.g., flooding);
infection-control concepts for equipment using water from main lines (e.g., water systems for hemodialysis, ice
machines, hydrotherapy equipment, dental unit water lines, and automated endoscope reprocessors);
environmental surface cleaning and disinfection strategies with respect to antibiotic-resistant microorganisms;
infection-control procedures for health-care laundry;
use of animals in health care for activities and therapy;
managing the presence of service animals in health-care facilities;
infection-control strategies for when animals receive treatment in human health-care facilities; and
a call to reinstate the practice of inactivating amplified cultures and stocks of microorganisms onsite during medical
waste treatment.
Topics outside the scope of this report include 1) noninfectious adverse events (e.g., sick building syndrome),
2) environmental concerns in the home, 3) home health care, 4) terrorism, and 5) health-care--associated foodborne illness.
Wherever possible, the recommendations in this report are based on data from well-designed scientific studies.
However, certain of these studies were conducted by using narrowly defined patient populations or specific health-care settings (e.g., hospitals versus long-term care facilities), making generalization of findings potentially problematic. Construction
standards for hospitals or other health-care facilities may not apply to residential home-care units. Similarly, infection-control measures indicated for immunosuppressed patient care are usually not necessary in those facilities where such patients are not present.
Other recommendations were derived from knowledge gained during infectious disease investigations in
health-care facilities, where successful termination of the outbreak was often the result of multiple interventions, the majority of which cannot be independently and rigorously evaluated. This is especially true for construction situations involving air or water.
Other recommendations were derived from empiric engineering concepts and may reflect industry standards rather
than evidence-based conclusions. Where recommendations refer to guidance from the American Institute of Architects (AIA),
the statements reflect standards intended for new construction or renovation. Existing structures and engineered systems are expected to be in continued compliance with those standards in effect at the time of construction or renovation.
Also, in the absence of scientific confirmation, certain infection-control recommendations that cannot be
rigorously evaluated are based on strong theoretic rationale and suggestive evidence. Finally, certain recommendations are derived from existing federal regulations.
Performance Measurements
Infections caused by the microorganisms described in this guideline are rare events, and the effect of these
recommendations on infection rates in a facility may not be readily measurable. Therefore, the following steps to measure performance are suggested to evaluate these recommendations:
Document whether infection-control personnel are actively involved in all phases of a health-care facility's
demolition, construction, and renovation. Activities should include performing a risk assessment of the necessary types of construction barriers, and daily monitoring and documenting of the presence of negative airflow within the construction zone or renovation area.
Monitor and document daily the negative airflow in AII rooms and positive airflow in PE rooms, especially when patients are in these rooms.
Perform assays at least once a month by using standard quantitative methods for endotoxin in water used to reprocess hemodialyzers, and for heterotrophic and mesophilic bacteria in water used to prepare dialysate and for hemodialyzer reprocessing.
Evaluate possible environmental sources (e.g., water, laboratory solutions, or reagents) of specimen contamination when nontuberculous mycobacteria (NTM) of unlikely clinical importance are isolated from clinical cultures. If
environmental contamination is found, eliminate the probable mechanisms.
Document policies to identify and respond to water damage. Such policies should result in either repair and drying of wet structural or porous materials within 72 hours, or removal of the wet material if drying is unlikely within 72 hours.
Updates to Previous Recommendations
Contributors to this report reviewed primarily English-language manuscripts identified from reference searches using
the National Library of Medicine's MEDLINE, bibliographies of published articles, and infection-control textbooks. All
the recommendations may not reflect the opinions of all reviewers. This report updates the following published guidelines and recommendations:
CDC. Guideline for handwashing and hospital environmental control. MMWR 1998;37(No. 24). Replaces sections
on microbiologic sampling, laundry, infective waste, and housekeeping.
Tablan OC, Anderson LJ, Arden NH, et al., Hospital Infection Control Practices Advisory Committee. Guideline
for prevention of nosocomial pneumonia. Infect Control Hosp Epidemiol 1994;15:587--627. Updates and
expands environmental infection-control information for aspergillosis and Legionnaires
disease; online version incorporates Appendices B, C, and D addressing environmental control and detection of Legionella spp.
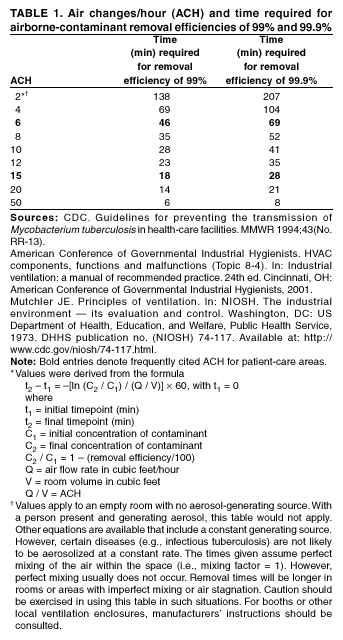
CDC. Guidelines for preventing the transmission of
mycobacterium tuberculosis in health-care facilities.
MMWR 1994;43(No. RR13). Provides supplemental information on engineering controls.
CDC. Recommendations for preventing the spread of vancomycin resistance: recommendations of the Hospital Infection Control Practices Advisory Committee (HICPAC). MMWR 1995;44(No. RR12). Supplements environmental infection-control information from the section, Hospitals with Endemic VRE or Continued VRE Transmission.
Garner JS, Hospital Infection Control Practices Advisory Committee. Guideline for isolation precautions in hospitals. Infect Control Hosp Epidemiol 1996;17:53--80. Supplements and updates topics in Part II --- Recommendations for Isolation Precautions in Hospitals (linen and laundry, routine and terminal cleaning, airborne precautions).
Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR, Hospital Infection Control Practices Advisory
Committee. Guideline for prevention of surgical site infection. Infect Control Hosp Epidemiol 1999;4:250--78. Updates operating room ventilation and surface cleaning/disinfection recommendations from the section, Intraoperative Issues: Operating
Room Environment.
U.S. Public Health Service, Infectious Diseases Society of America, Prevention of Opportunistic Infections Working
Group. USPHS/IDSA guidelines for the prevention of opportunistic infections in persons infected with human
immunodeficiency virus. Infect Dis Obstet Gynecol 2002; 10:3--64. Supplements information regarding patient interaction with pets and animals in the home.
CDC, Infectious Diseases Society of America, American Society of Blood and Marrow Transplantation. Guidelines
for preventing opportunistic infections among hematopoietic stem cell transplant recipients. Cytotherapy
2001;3:41--54. Supplements and updates the section, Hospital Infection Control.
Key Terms
Airborne infection isolation (AII) refers to the isolation of patients infected with organisms spread via airborne
droplet nuclei <5 µm in diameter. This isolation area receives numerous air changes per hour (ACH) (>12 ACH for new construction as of 2001;
>6 ACH for construction before 2001), and is under negative pressure, such that the direction of the air flow is from the outside adjacent space (e.g., the corridor) into the room. The air in an AII room is preferably exhausted to
the outside, but may be recirculated provided that the return air is filtered through a high-efficiency particulate air (HEPA) filter. The use of personal respiratory protection is also indicated for persons entering these rooms when caring for TB or
smallpox patients and for staff who lack immunity to airborne viral diseases (e.g., measles or varicella zoster virus [VZV] infection).
Protective environment (PE) is a specialized patient-care area, usually in a hospital, with a positive air flow relative to
the corridor (i.e., air flows from the room to the outside adjacent space). The combination of HEPA filtration, high numbers of air changes per hour (>12 ACH), and minimal leakage of air into the room creates an environment that can safely accommodate patients who have undergone allogeneic hematopoietic stem cell transplant (HSCT).
Immunocompromised patients are those patients whose immune mechanisms are deficient because of
immunologic disorders (e.g., human immunodeficiency virus [HIV] infection or congenital immune deficiency syndrome), chronic diseases (e.g., diabetes, cancer, emphysema, or cardiac failure), or immunosuppressive therapy (e.g., radiation, cytotoxic chemotherapy, anti-rejection medication, or steroids). Immunocompromised patients who are identified as high-risk patients have the greatest risk of infection caused by airborne or waterborne microorganisms. Patients in this subset include persons who are severely neutropenic for prolonged periods of time (i.e., an absolute neutrophil count [ANC] of
<500 cells/mL), allogeneic HSCT patients, and those who have received the most intensive chemotherapy (e.g., childhood acute myelogenous leukemia patients).
Abbreviations
AAMI Association for the Advancement of Medical Instrumentation
ACH air changes per hour
AER automated endoscope reprocessor
AHJ authority having jurisdiction
AIA American Institute of Architects
AII airborne infection isolation
ANSI American National Standards Institute
ASHRAE American Society of Heating, Refrigeration, and Air-Conditioning Engineers
BMBL Biosafety in Microbiological and Biomedical Laboratories (CDC/National Institutes of Health)
CFR Code of Federal Regulations
CJD Creutzfeldt-Jakob disease
CPL compliance document (OSHA)
DFA direct fluorescence assay
DHHS U.S. Department of Health and Human Services
DOT U.S. Department of Transportation
EC environment of care
EPA U. S. Environmental Protection Agency
FDA U.S. Food and Drug Administration
HBV hepatitis B virus
HEPA high efficiency particulate air
HIV human immunodeficiency virus
HSCT hematopoietic stem cell transplant
HVAC heating, ventilation, air conditioning
ICRA infection-control risk assessment
JCAHO Joint Commission on Accreditation of Healthcare Organizations
NaOH sodium hydroxide
NTM nontuberculous mycobacteria
OSHA Occupational Safety and Health Administration
PE protective environment
PPE personal protective equipment
TB tuberculosis
USC United States Code
USDA U.S. Department of Agriculture
UV ultraviolet
UVGI ultraviolet germicidal irradiation
VHF viral hemorrhagic fever
VRE vancomycin-resistant Enterococcus
VRSA vancomycin-resistant Staphylococcus aureus
VZV varicella zoster virus
Recommendations for Environmental Infection Control in Health-Care Facilities
Rationale for Recommendations
As in previous CDC guidelines, each recommendation is categorized on the basis of existing scientific data,
theoretic rationale, applicability, and possible economic effect. The recommendations are evidence-based wherever possible. However, certain recommendations are derived from empiric infection-control or engineering principles, theoretic rationale, or from experience gained from events that cannot be readily studied (e.g., floods).
The HICPAC system for categorizing recommendations has been modified to include a category for engineering
standards and actions required by state or federal regulations. Guidelines and standards published by the AIA, American Society of Heating, Refrigeration, and Air-Conditioning Engineers (ASHRAE), and the Association for the Advancement of
Medical Instrumentation (AAMI) form the basis of certain recommendations. These standards reflect a consensus of expert opinions and extensive consultation with agencies of the U.S. Department of Health and Human Services. Compliance with
these standards is usually voluntary. However, state and federal governments often adopt these standards as regulations. For example, the standards from AIA regarding construction and design of new or renovated health-care facilities, have been adopted by reference by >40 states. Certain recommendations have two category ratings (e.g., Categories IA and IC or Categories IB and IC), indicating the recommendation is evidence-based as well as a standard or regulation.
Rating Categories
Recommendations are rated according to the following categories:
Category IA. Strongly recommended for implementation and strongly supported by well-designed experimental, clinical,
or epidemiologic studies.
Category IB. Strongly recommended for implementation and supported by certain experimental, clinical, or
epidemiologic studies and a strong theoretic rationale.
Category IC. Required by state or federal regulation, or representing an established association standard.
(Note: Abbreviations for governing agencies and regulatory citations are listed where appropriate. Recommendations from
regulations adopted at state levels are also noted. Recommendations from AIA guidelines cite the appropriate sections of the standards.)
Category II.Suggested for implementation and supported by suggestive clinical or epidemiologic studies, or a
theoretic rationale.
Unresolved issue. No recommendation is offered. No consensus or insufficient evidence exists regarding efficacy.
Recommendations --- Air
I. Air-Handling Systems in Health-Care Facilities
Use AIA guidelines as minimum standards where state or local regulations are not in place for design
and construction of ventilation systems in new or renovated health-care facilities. Ensure that existing structures
continue to meet the specifications in effect at the time of construction
(1). Category IC (AIA: 1.1.A, 5.4)
Monitor ventilation systems in accordance with engineers' and manufacturers' recommendations to
ensure preventive engineering, optimal performance for removal of particulates, and elimination of excess moisture
(1--8). Category IB, IC (AIA: 7.2, 7.31.D, 8.31.D, 9.31.D, 10.31.D, 11.31.D, Environmental Protection Agency [EPA] guidance)
1. Ensure that heating, ventilation, air conditioning (HVAC) filters are properly installed and maintained
to prevent air leakages and dust overloads
(2,4,6,9). Category IB
2. Monitor areas with special ventilation requirements (e.g., AII or PE) for ACH, filtration, and
pressure differentials (1,7,8,10--26). Category IB, IC (AIA: 7.2.C7, 7.2.D6)
a. Develop and implement a maintenance schedule for ACH,
pressure differentials, and filtration efficiencies by using
facility-specific data as part of the multidisciplinary risk
assessment. Take into account the age
and reliability of the system.
b. Document these parameters, especially the pressure differentials.
3. Engineer humidity controls into the HVAC system and monitor the controls to ensure adequate
moisture removal (1). Category IC (AIA: 7.31.D9)
a. Locate duct humidifiers upstream from the final filters.
b. Incorporate a water-removal mechanism into the system.
c. Locate all duct takeoffs sufficiently downstream from the humidifier so that moisture is completely absorbed.
4. Incorporate steam humidifiers, if possible, to reduce potential for microbial proliferation within the system,
and avoid use of cool-mist humidifiers. Category II
5. Ensure that air intakes and exhaust outlets are located properly in construction of new facilities and renovation
of existing facilities (1,27). Category IC (AIA: 7.31.D3, 8.31.D3,
9.31.D3, 10.31.D3, 11.31.D3)
a. Locate exhaust outlets >25 ft from air-intake systems.
b. Locate outdoor air intakes >6 ft above ground or
>3 ft above roof level.
c. Locate exhaust outlets from contaminated areas above roof level to minimize recirculation of exhausted air.
6. Maintain air intakes and inspect filters periodically to ensure proper operation
(1,11--16,27). Category IC (AIA: 7.31.D8)
7. Bag dust-filled filters immediately upon removal to prevent dispersion of dust and fungal spores during
transport within the facility (4,28). Category IB
a. Seal or close the bag containing the discarded filter.
b. Discard spent filters as regular solid waste, regardless of the area from which they were removed
(28).
8. Remove bird roosts and nests near air intakes to prevent mites and fungal spores from entering the
ventilation system (27,29,30). Category IB
9. Prevent dust accumulation by cleaning air-duct grilles in accordance with facility-specific procedures
and schedules and when rooms are not occupied by patients
(1,10--16).
Category IC, II (AIA: 7.31.D10)
10. Periodically measure output to monitor system function; clean ventilation ducts as part of routine
HVAC maintenance to ensure optimum performance
(1,31,32). Category IC, II
(AIA: 7.31.D10)
Use portable, industrial-grade HEPA filter units capable of filtration rates in the range of 300--800
ft3/min to augment removal of respirable particles as needed
(33). Category II
1. Select portable HEPA filters that can recirculate all or nearly all of the room air and provide the equivalent of
>12 ACH (34). Category II
2. Portable HEPA filter units placed in construction zones can be used later in patient-care areas, provided
all internal and external surfaces are cleaned, and the filter replaced or its
performance verified by
appropriate particle testing. Category II
3. Situate portable HEPA units with the advice of facility engineers to ensure that all room air is filtered
(34). Category II
4. Ensure that fresh-air requirements for the area are met
(33,35). Category II
Follow appropriate procedures for use of areas with through-the-wall ventilation units
(1). Category IC (AIA: 8.31.D1, 8.31.D8, 9.31.D23, 10.31.D18, 11.31.D15)
1. Do not use such areas as PE rooms
(1). Category IC (AIA: 7.2.D3)
2. Do not use a room with a through-the-wall ventilation unit as an AII room unless it can be demonstrated that
all required AII engineering controls are met
(1,34). Category IC (AIA:
7.2.C3)
Conduct an infection-control risk assessment (ICRA) and provide an adequate number of AII and PE rooms
(if required) or other areas to meet the needs of the patient population
(1,2,7,8,17,19, 20,34,36--43). Category IA,
IC (AIA: 7.2.C, 7.2.D)
When ultraviolet germicidal irradiation (UVGI) is used as a supplemental engineering control, install fixtures 1)
on the wall near the ceiling or suspended from the ceiling as an upper air unit; 2) in the air-return duct of an AII
area; or 3) in designated enclosed areas or booths for sputum induction
(34). Category II
Seal windows in buildings with centralized HVAC systems, including PE areas
(1,3,44). Category IB, IC (AIA: 7.2.D3)
Keep emergency doors and exits from PE rooms closed except during an emergency; equip emergency doors
and exits with alarms. Category II
Develop a contingency plan for backup capacity in the event of a general power failure
(45). Category IC (Joint Commission on Accreditation of Healthcare Organizations [JCAHO]: Environment of Care [EC] 1.4)
1. Emphasize restoration of appropriate air quality and ventilation conditions in AII rooms, PE rooms,
operating rooms, emergency departments, and intensive care units
(1,45).
Category IC (AIA: 1.5.A1; JCAHO: EC 1.4)
2. Deploy infection-control procedures to protect occupants until power and systems functions are
restored (1,36,45). Category IC (AIA: 5.1, 5.2; JCAHO: EC 1.4)
Do not shut down HVAC systems in patient-care areas exept for maintenance, repair, testing of emergency
backup capacity, or new construction (1,46). Category IB, IC (AIA: 5.1, 5.2.B, C)
1. Coordinate HVAC system maintenance with infection-control staff and relocate immunocompromised
patients if necessary (1). Category IC (AIA: 5.1, 5.2)
2. Provide backup emergency power and air-handling and pressurization systems to maintain filtration,
constant ACH, and pressure differentials in PE rooms, AII rooms, operating
rooms, and other critical-care areas (1,37,47). Category IC (AIA: 5.1, 5.2)
3. For areas not served by installed emergency ventilation and backup systems, use portable units and
monitor ventilation parameters and patients in those areas
(33). Category II
4. Coordinate system startups with infection-control staff to protect patients in PE rooms from bursts of
fungal spores (1,3,37,47). Category IC (AIA: 5.1, 5.2)
5. Allow sufficient time for ACH to clean the air once the system is operational (Table 1)
(1,33). Category IC (AIA: 5.1, 5.2)
HVAC systems serving offices and administrative areas may be shut down for energy conservation purposes, but
the shutdown must not alter or adversely affect pressure differentials maintained in laboratories or critical-care areas with specific ventilation requirements (i.e., PE rooms, AII rooms, operating rooms). Category II
Whenever possible, avoid inactivating or shutting down the entire HVAC system, especially in acute-care
facilities. Category II
Whenever feasible, design and install fixed backup ventilation systems for new or renovated construction of
PE rooms, AII rooms, operating rooms, and other critical-care areas identified by ICRA
(1). Category IC (AIA: 1.5.A1)
II. Construction, Renovation, Remediation, Repair, and Demolition
Establish a multidisciplinary team that includes infection-control staff to coordinate demolition, construction,
and renovation projects and consider proactive preventive measures at the inception; produce and maintain
summary statements of the team's activities
(1,9,11--16,38,48--51). Category IB, IC (AIA: 5.1)
Educate both the construction team and health-care staff in immunocompromised patient-care areas regarding
the airborne infection risks associated with construction projects, dispersal of fungal spores during such activities, and methods to control the dissemination of fungal spores
(11--16,27,50,52--56). Category IB
Incorporate mandatory adherence agreements for infection control into construction contracts, with penalties
for noncompliance and mechanisms to ensure timely correction of problems
(1,11,13--16,27,50). Category IC (AIA: 5.1)
Establish and maintain surveillance for airborne environmental disease (e.g., aspergillosis) as appropriate
during construction, renovation, repair, and demolition activities to ensure the health and safety of
immunocompromised patients (27,57--59). Category IB
1. Using active surveillance, monitor for airborne infections in immunocompromised patients
(27,37,57,58). Category IB
2. Periodically review the facility's microbiologic, histopathologic, and postmortem data to identify additional
cases (27,37,57,58). Category IB
3. If cases of aspergillosis or other health-care--associated airborne fungal infections occur, aggressively pursue
the diagnosis with tissue biopsies and cultures as feasible
(11,13--
16,27,50,57--59). Category IB
Implement infection-control measures relevant to construction, renovation, maintenance, demolition, and
repair (1,16,49,50,60). Category IB, IC (AIA: 5.1, 5.2)
1. Before the project gets under way, perform an ICRA to define the scope of the activity and the need for
barrier measures (1,11,13--16,48--51,60). Category IB, IC (AIA: 5.1)
a. Determine if immunocompromised patients may be at risk for exposure to fungal spores from dust
generated during the project (13--16,48,51).
b. Develop a contingency plan to prevent such exposures
(13--16,48,51).
2. Implement infection-control measures for external demolition and construction activities
(11,13--16,50,61,62). Category IB
a. Determine if the facility can operate temporarily on recirculated air; if feasible, seal off adjacent air intakes.
b. If this is not possible or practical, check the low-efficiency (roughing) filter banks frequently and replace
as needed to avoid buildup of particulates.
c. Seal windows and reduce wherever possible other sources of outside air intrusion (e.g., open doors
in stairwells and corridors), especially in PE areas.
3. Avoid damaging the underground water system (i.e., buried pipes) to prevent soil and dust contamination of
the water (1,63). Category IB, IC (AIA: 5.1)
4. Implement infection-control measures for internal construction activities
(1,11,13--16,48-- 50,64). Category IB, IC (AIA: 5.1, 5.2)
a. Construct barriers to prevent dust from construction areas from entering patient-care areas; ensure
that barriers are impermeable to fungal spores and in compliance with local fire
codes (1,45,48,49,55,64--66).
b. Seal off and block return air vents if rigid barriers are used for containment
(1,16,50).
c. Implement dust-control measures on surfaces and divert pedestrian traffic away from work
zones (1,48,49,64).
d. Relocate patients whose rooms are adjacent to work zones, depending on their immune status, the scope
of the project, the potential for generation of dust or water aerosols, and
the methods used to control
these aerosols (1,64,65).
5. Perform those engineering and work-site related infection-control measures as needed for internal
construction, repairs, and renovations
(1,48,49,51,64,66). Category IB, IC (AIA:
5.1, 5.2)
a. Ensure proper operation of the air-handling system in the affected area after erection of barriers and
before the room or area is set to negative pressure
(39,47,50,64). Category
IB
b. Create and maintain negative air pressure in work zones adjacent to patient-care areas and ensure
that required engineering controls are maintained
(1,48,49,51,64,66).
c. Monitor negative airflow inside rigid barriers
(1,67).
d. Monitor barriers and ensure integrity of the construction barriers; repair gaps or breaks in barrier
joints (1,65,66,68).
e. Seal windows in work zones if practical; use window chutes for disposal of large pieces of debris as
needed, but ensure that the negative pressure differential for the area is
maintained
(1,13,48).
f. Direct pedestrian traffic from construction zones away from patient-care areas to minimize dispersion of
dust (1,13--16,44,48--51,64).
g. Provide construction crews with 1) designated entrances, corridors, and elevators wherever practical;
2) essential services (e.g., toilet facilities) and convenience services (e.g.,
vending machines); 3)
protective clothing (e.g., coveralls, footgear, and headgear) for travel to patient-care areas; and 4) a space or anteroom for changing clothing and storing
equipment
(1,11,13--16,50).
h. Clean work zones and their entrances daily by 1) wet-wiping tools and tool carts before their removal
from the work zone; 2) placing mats with tacky surfaces inside the entrance;
and 3) covering debris and
securing this covering before removing debris from the work zone
(1,11,13--16,50).
i. In patient-care areas, for major repairs that include removal of ceiling tiles and disruption of the space
above the false ceiling, use plastic sheets or prefabricated plastic units to
contain dust; use a negative pressure system within this enclosure to remove dust; and either pass air through an industrial-grade, portable HEPA
filter capable of filtration rates of
300--800
ft3/min., or exhaust air directly to the outside
(16,50,64,67,69).
j. Upon completion of the project, clean the work zone according to facility procedures, and install
barrier curtains to contain dust and debris before removing rigid barriers
(1,11,13-
-16,48--50).
k. Flush the water system to clear sediment from pipes to minimize waterborne microorganism
proliferation (1,63).
l. Restore appropriate ACH, humidity, and pressure differential; clean or replace air filters; dispose of
spent filters (3,4,28,47).
Use airborne-particle sampling as a tool to evaluate barrier integrity
(3,70). Category II
Commission the HVAC system for newly constructed health-care facilities and renovated spaces before
occupancy and use, with emphasis on ensuring proper ventilation for operating rooms, AII rooms, and PE areas (1,70--72). Category IC (AIA: 5.1; ASHRAE: 1-1996)
No recommendation is offered regarding routine microbiologic air sampling before, during, or after construction,
or before or during occupancy of areas housing immunocompromised patients
(9,48,49,51,64,73,74). Unresolved issue
If a case of health-care--acquired aspergillosis or other opportunistic environmental airborne fungal disease
occurs during or immediately after construction, implement appropriate follow-up measures
(40,48,75--78). Category IB
1. Review pressure-differential monitoring documentation to verify that pressure differentials in the
construction zone and in PE rooms are appropriate for their settings
(1,40,78).
Category IB, IC (AIA: 5.1)
2. Implement corrective engineering measures to restore proper pressure differentials as needed
(1,40,78). Category IB, IC (AIA: 5.1)
3. Conduct a prospective search for additional cases and intensify retrospective epidemiologic review of
the hospital's medical and laboratory records
(27,48,76,79,80). Category IB
4. If no epidemiologic evidence of ongoing transmission exists, continue routine maintenance in the area to
prevent health-care--acquired fungal disease
(27,75). Category IB
If no epidemiologic evidence exists of ongoing transmission of fungal disease, conduct an environmental
assessment to find and eliminate the source
(11,13--16,27,44,49--51,60,81). Category IB
1. Collect environmental samples from potential sources of airborne fungal spores, preferably by using a
high-volume air sampler rather than settle plates (2,4,11,13--
16,27,44,49,50,64,65,81--86). Category IB
2. If either an environmental source of airborne fungi or an engineering problem with filtration or
pressure differentials is identified, promptly perform corrective measures to eliminate the
source and route of entry (49,60). Category IB
3. Use an EPA-registered antifungal biocide (e.g., copper-8-quinolinolate) for decontaminating structural
materials (16,61,66,87). Category IB
4. If an environmental source of airborne fungi is not identified, review infection-control measures,
including engineering controls, to identify potential areas for correction or improvement
(88,89). Category IB
5. If possible, perform molecular subtyping of
Aspergillus spp. isolated from patients and the environment to compare their strain identities (90--94). Category II
If air-supply systems to high-risk areas (e.g., PE rooms) are not optimal, use portable, industrial-grade HEPA
filters on a temporary basis until rooms with optimal air-handling systems become available
(1,13--16,27,50). Category II
III. Infection Control and Ventilation Requirements for PE rooms
Minimize exposures of severely immunocompromised patients (e.g., solid-organ transplant patients or
allogeneic neutropenic patients) to activities that might cause aerosolization of fungal spores (e.g., vacuuming or disruption of ceiling tiles) (37,48,51,73). Category IB
Minimize the length of time that immunocompromised patients in PE are outside their rooms for
diagnostic procedures and other activities
(37,62). Category IB
Provide respiratory protection for severely immunocompromised patients when they must leave PE for
diagnostic procedures and other activities; consult the most recent revision of CDC's
Guideline for Prevention of Health-Care--Associated
Pneumonia for information regarding the appropriate type of respiratory protection.
(27,37). Category II
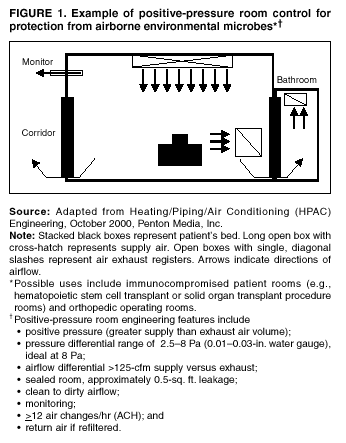
Incorporate ventilation engineering specifications and dust-controlling processes into the planning and
construction of new PE units (Figure 1). Category IB, IC
1. Install central or point-of-use HEPA filters for supply (incoming) air
(1,2,27,48,56,70, 80,82,85,95--102). Category IB, IC (AIA: 5.1, 5.2, 7.2.D)
2. Ensure that rooms are well-sealed by 1) properly constructing windows, doors, and intake and exhaust ports;
2) maintaining ceilings that are smooth and free of fissures, open joints,
and crevices; 3) sealing walls above
and below the ceiling; and 4) monitoring for leakage and making any necessary repairs
(1,27,44,100,101). Category IB, IC (AIA: 7.2.D3)
3. Ventilate the room to maintain
>12 ACH (1,27,37,100,101,103). Category IC (AIA: 7.2.D)
4. Locate air supply and exhaust grilles so that clean, filtered air enters from one side of the room, flows across
the patient's bed, and exits from the opposite side of the room
(1,27,100,101). Category IC (AIA: 7.31.D1)
5. Maintain positive room air pressure
(>2.5 Pa [0.01-inch water gauge]) in relation to the corridor (1,3,27,100,101). Category IB, IC (AIA: Table 7.2)
6. Maintain airflow patterns and monitor these on a daily basis by using permanently installed visual means
of detecting airflow in new or renovated construction, or by using other visual
methods (e.g., flutter strips or smoke tubes) in existing PE units. Document the monitoring results
(1,13). Category IC (AIA: 7.2.D6)
7. Install self-closing devices on all room exit doors in PE rooms
(1). Category IC (AIA: 7.2.D4)
Do not use laminar air flow systems in newly constructed PE rooms
(99,101). Category II
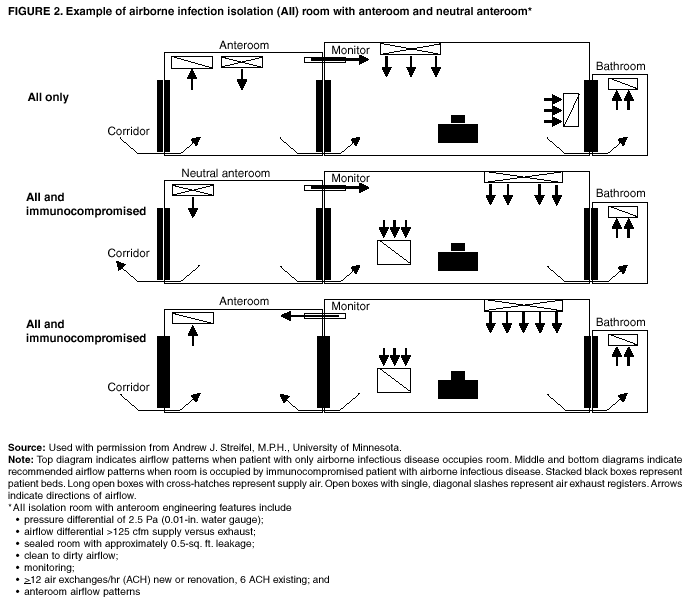
Take measures to protect immunocompromised patients who would benefit from a PE room and who also have
an airborne infectious disease (e.g., acute VZV infection or tuberculosis).
1. Ensure that the patient's room is designed to maintain positive pressure.
2. Use an anteroom to ensure appropriate air-balance relationships and provide independent exhaust
of contaminated air to the outside, or place a HEPA filter in the exhaust duct if the
return air must be recirculated (1,100) (Figure 2).
Category IC (AIA: 7.2.D1, A7.2.D)
3. If an anteroom is not available, place the patient in AII and use portable, industrial-grade HEPA filters
to enhance filtration of spores in the room
(33). Category II
Maintain backup ventilation equipment (e.g., portable units for fans or filters) for emergency provision of
required ventilation for PE areas and take immediate steps to restore the fixed ventilation system
(1,37,47). Category IC (AIA: 5.1)
IV. Infection-Control and Ventilation Requirements for AII Rooms
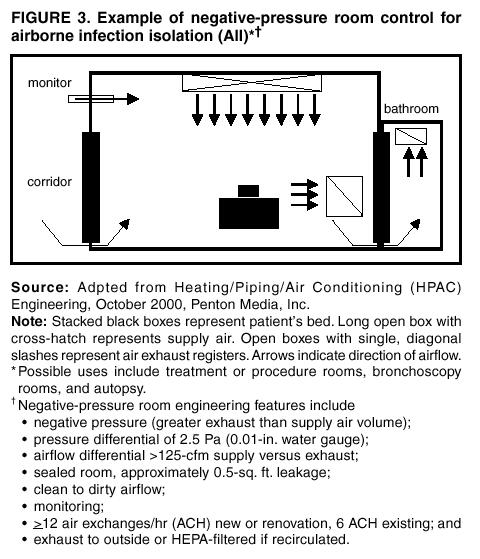
Incorporate certain specifications into the planning and construction or renovation of AII units
(1,34,100,101,104) (Figure 3). Category IB, IC
1. Maintain continuous negative air pressure (2.5 Pa [0.01 inch water gauge]) in relation to the air pressure in
the corridor; monitor air pressure periodically, preferably daily, with
audible manometers or smoke tubes at the
door (for existing AII rooms), or with a permanently installed visual monitoring mechanism. Document the results of monitoring
(1,100,101). Category IC (AIA: 7.2.C7, Table 7.2)
2. Ensure that rooms are well-sealed by properly constructing windows, doors, and air-intake and exhaust
ports; when monitoring indicates air leakage, locate the leak and make
necessary repairs
(1,99,100). Category IB, IC (AIA: 7.2.C3)
3. Install self-closing devices on all AII room exit doors
(1). Category IC (AIA: 7.2.C4)
4. Provide ventilation to ensure
>12 ACH for renovated rooms and new rooms, and >6 ACH for existing AII rooms (1,34,104). Category IB, IC (AIA: Table 7.2)
5. Direct exhaust air to the outside, away from air-intake and populated areas. If this is not practical, air from
the room can be recirculated after passing through a HEPA filter
(1,34).
Category IC (AIA: Table 7.2)
Where supplemental engineering controls for air cleaning are indicated from a risk assessment of the AII area,
install UVGI units in the exhaust air ducts of the HVAC system to supplement HEPA filtration or install UVGI fixtures
on or near the ceiling to irradiate upper room air
(34). Category II
Implement environmental infection-control measures for persons with diagnosed or suspected airborne
infectious diseases.
1. Use AII rooms for patients with or suspected of having an airborne infection who also require
cough-inducing procedures, or use an enclosed booth that is engineered to provide 1) >12 ACH; 2) air supply and exhaust rate sufficient to maintain a 2.5 Pa (0.01-inch water gauge) negative pressure difference with respect to all surrounding spaces with an exhaust
rate of
>50 ft3/min; and 3) air exhausted directly outside away from
air intakes and traffic or exhausted after HEPA filtration before recirculation (1,34,105--107). Category IB, IC
(AIA: 7.15.E, 7.31.D23, 9.10, Table 7.2)
2. Although airborne spread of viral hemorrhagic fever (VHF) has not been documented in a health-care
setting, prudence dictates placing a VHF patient in an AII room, preferably
with an anteroom, to reduce the risk of occupational exposure to aerosolized infectious material in blood, vomitus, liquid stool, and
respiratory secretions present in large amounts
during the end stage of a patient's illness
(108--110). Category II
a. If an anteroom is not available, use portable, industrial-grade HEPA filters in the patient's room to
provide additional ACH equivalents for removing airborne particulates.
b. Ensure that health-care workers wear face shields or goggles with appropriate respirators when entering
the rooms of VHF patients with prominent cough, vomiting, diarrhea, or
hemorrhage
(109).
3. Place smallpox patients in negative pressure rooms at the onset of their illness, preferably using a room with
an anteroom, if available (36). Category II
No recommendation is offered regarding negative pressure or isolation for patients with
Pneumocystis carinii pneumonia
(111--113). Unresolved issue.
Maintain backup ventilation equipment (e.g., portable units for fans or filters) for emergency provision of
ventilation requirements for AII rooms, and take immediate steps to restore the fixed ventilation system (1,34,47). Category IC (AIA: 5.1)
V. Infection-Control and Ventilation Requirements for Operating Rooms
Implement environmental infection-control and ventilation measures for operating rooms.
1. Maintain positive-pressure ventilation with respect to corridors and adjacent areas
(1,114,115). Category IB, IC (AIA: Table 7.2)
2. Maintain >15 ACH, of which
>3 ACH should be fresh air (1,116,117). Category IC (AIA: Table 7.2)
3. Filter all recirculated and fresh air through the appropriate filters, providing 90% efficiency (dust-spot testing)
at a minimum (1,118). Category IC (AIA: Table 7.3)
4. In rooms not engineered for horizontal laminar airflow, introduce air at the ceiling and exhaust air near the
floor (1,115,119). Category IC (AIA: 7.31.D4)
5. Do not use ultraviolet (UV) lights to prevent surgical-site infections
(115,120--126). Category IB
6. Keep operating room doors closed except for the passage of equipment, personnel, and patients, and limit
entry to essential personnel (127,128). Category IB
Follow precautionary procedures for infectious TB patients who also require emergency surgery
(34,129,130). Category IB, IC
1. Use an N95 respirator approved by the National Institute for Occupational Safety and Health without
exhalation valves in the operating room
(129,131). Category IC (Occupational
Safety and Health Administration
[OSHA]; 29 Code of Federal Regulations [CFR] 1910.134,139)
2. Intubate the patient in either the AII room or the operating room; if intubating the patient in the
operating room, do not allow the doors to open until 99% of the airborne contaminants
are removed (Table 1) (34,117). Category IB
3. When anesthetizing a patient with confirmed or suspected TB, place a bacterial filter between the
anesthesia circuit and patient's airway to prevent contamination of anesthesia
equipment or discharge of tubercle bacilli into the ambient air (130,132). Category IB
4. Extubate and allow the patient to recover in an AII room
(34,117). Category IB
5. If the patient has to be extubated in the operating room, allow adequate time for ACH to clean
99% of airborne particles from the air (Table 1), because extubation is a cough-
producing procedure
(34,117). Category IB
Use portable, industrial-grade HEPA filters temporarily for supplemental air cleaning during intubation
and extubation for TB patients who require surgery
(33,34,117). Category II
1. Position the units appropriately so that all room air passes through the filter; obtain engineering consultation
to determine the appropriate placements (34). Category II
2. Switch the portable unit off during the surgical procedure. Category II
3. Provide fresh air as per ventilation standards for operating rooms; portable units do not meet the
requirements for the number of fresh ACH
(1,33,133). Category II
If possible, schedule TB patients as the last surgical cases of the day to maximize the time available for removal
of airborne contamination. Category II
No recommendation is offered for performing orthopedic implant operations in rooms supplied with
laminar airflow (118,120). Unresolved issue
Maintain backup ventilation equipment (e.g., portable units for fans or filters) for emergency ventilation
of operating rooms, and take immediate steps to restore the fixed ventilation system
(1,47,131,134). Category IB, IC (AIA: 5.1)
VI. Other Potential Infectious Aerosol Hazards in Health-Care Facilities
In settings where surgical lasers are used, wear appropriate personal protective equipment (PPE), including N95
or N100 respirators, to minimize exposure to laser plumes
(129,135,136). Category IC (OSHA; 29 CFR 1910.134,139)
Use central wall suction units with in-line filters to evacuate minimal laser plumes
(135--138). Category II
Use a mechanical smoke evacuation system with a high-efficiency filter to manage the generation of large amounts
of laser plume, when ablating tissue infected with human papilloma virus (HPV) or performing procedures on a
patient with extrapulmonary TB
(34,136,137,139--141). Category II
Recommendations --- Water
I. Controlling the Spread of Waterborne Microorganisms
Practice hand hygiene to prevent the hand transfer of waterborne pathogens, and use barrier precautions (e.g.,
gloves) as defined by other guidelines
(36,142--146). Category IA
Eliminate contaminated water or fluid environmental reservoirs (e.g., in equipment or solutions) wherever
possible (142,147). Category IB
Clean and disinfect sinks and wash basins on a regular basis by using an EPA-registered product as set by
facility policies. Category II
Evaluate for possible environmental sources (e.g., potable water) of specimen contamination when
waterborne microorganisms (e.g., NTM) of unlikely clinical importance are isolated from clinical cultures (e.g.,
specimens collected aseptically from sterile sites or, if postprocedural, colonization after use of tap water in patient care) (148--151). Category IB
Avoid placing decorative fountains and fish tanks in patient-care areas; ensure disinfection and fountain
maintenance if decorative fountains are used in public areas of the health-care facility
(152). Category IB
II. Routine Prevention of Waterborne Microbial
Contamination Within the Distribution System
Maintain hot water temperature at the return at the highest temperature allowable by state regulations or
codes, preferably >124ºF
(>51ºC), and maintain cold water temperature at <68ºF (<20ºC)
(27,153). Category IC (States; ASHRAE: 12:2000)
If the hot water temperature can be maintained at
>124ºF
(>51ºC), explore engineering options (e.g.,
installing preset thermostatic valves in point-of-use fixtures) to help minimize the risk of scalding (153). Category II
When state regulations or codes do not allow hot water temperatures above the range of
105ºF--120ºF
(40.6ºC--49ºC) for hospitals or 95ºF--110ºF
(35ºC--43.3ºC) for nursing care facilities or when buildings cannot be
retrofitted for thermostatic mixing valves, follow either of these alternative preventive measures to minimize the growth of Legionella spp. in water systems. Category II
1. Periodically increase the hot water temperature to
>150ºF
(>66ºC) at the point of use
(153). Category II
2. Alternatively, chlorinate the water and then flush it through the system
(153--155). Category II
Maintain constant recirculation in hot-water distribution systems serving patient-care areas
(1). Category IC (AIA: 7.31.E.3)
III. Remediation Strategies for Distribution System Repair or Emergencies
Whenever possible, disconnect the ice machine before planned water disruptions. Category II
Prepare a contingency plan to estimate water demands for the entire facility in advance of significant
water disruptions (i.e., those expected to result in extensive and heavy microbial or chemical contamination of the potable water), sewage intrusion, or flooding
(45,156). Category IC (JCAHO: EC 1.4)
When a significant water disruption or an emergency occurs, adhere to any advisory to boil water issued by
the municipal water utility (157). Category IB, IC (Municipal order)
1. Alert patients, families, staff, and visitors not to consume water from drinking fountains, ice, or drinks
made from municipal tap water, while the advisory is in effect, unless the water
has been disinfected (e.g., by bringing to a rolling boil for >1 minute)
(157). Category IB, IC (Municipal order)
2. After the advisory is lifted, run faucets and drinking fountains at full flow for
>5minutes, or use high-temperature water flushing or chlorination (153,157). Category IC, II (Municipal
order; ASHRAE: 12:2000)
Maintain a high level of surveillance for waterborne disease among patients after a boil water advisory is
lifted. Category II
Corrective decontamination of the hot water system might be necessary after a disruption in service or a
cross-connection with sewer lines has occurred.
1. Decontaminate the system when the fewest occupants are present in the building (e.g., nights or
weekends) (27,153). Category IC (ASHRAE: 12:2000)
2. If using high-temperature decontamination, raise the hot-water temperature to
160ºF--170ºF
(71ºC--77ºC) and maintain that level while progressively flushing each outlet around the
system for >5 minutes (27,153). Category IC (ASHRAE: 12:2000)
3. If using chlorination, add enough chlorine, preferably overnight, to achieve a free chlorine residual of
>2 mg/L (>2 ppm) throughout the system
(153). Category IC (ASHRAE:
12:2000)
a. Flush each outlet until chlorine odor is detected.
b. Maintain the elevated chlorine concentration in the system for
>2 (but <24 hrs).
4. Use a thorough flushing of the water system instead of chlorination if a highly chlorine-resistant
microorganism (e.g., Cryptosporidium spp.) is suspected as the water contaminant.
Category II
Flush and restart equipment and fixtures according to manufacturer's instructions. Category II
Change the pretreatment filter and disinfect the dialysis water system with an EPA-registered product to
prevent colonization of the reverse osmosis membrane and downstream microbial contamination
(158). Category II
Run water softeners through a regeneration cycle to restore their capacity and function. Category II
If the facility has a water-holding reservoir or water-storage tank, consult the facility engineer or local
health department to determine whether this equipment needs to be drained, disinfected with an EPA-registered
product, and refilled. Category II
Implement facility procedures to manage a sewage system failure or flooding (e.g., arranging with other
health-care facilities for temporary transfer of patients or provision of services), and establish communications with the local municipal water utility and the local health department to ensure that advisories are received in a timely manner after release (45,156). Category IC (JCAHO: EC 1.4; Municipal order)
Implement infection-control measures during sewage intrusion, flooding, or other water-related emergencies.
1. Relocate patients and clean or sterilize supplies from affected areas. Category II
2. If hands are not visibly soiled or contaminated with proteinaceous material, include an alcohol-based hand
rub in the hand hygiene process 1) before performing invasive procedures;
2) before and after each patient
contact; and 3) whenever hand hygiene is indicated
(146). Category II
3. If hands are visibly soiled or contaminated with proteinaceous material, use soap and bottled water
for handwashing (146). Category II
4. If the potable water system is not affected by flooding or sewage contamination, process surgical instruments
for sterilization according to standard procedures. Category II
5. Contact the manufacturer of the automated endoscope reprocessor (AER) for specific instructions on the use
of this equipment during a water advisory. Category II
Remediate the facility after sewage intrusion, flooding, or other water-related emergencies.
1. Close off affected areas during cleanup procedures. Category II
2. Ensure that the sewage system is fully functional before beginning remediation so contaminated solids
and standing water can be removed. Category II
3. If hard-surfaced equipment, floors, and walls remain in good repair, ensure that these are dry
within 72 hours; clean with detergent according to standard cleaning procedures.
Category II
4. Clean wood furniture and materials (if still in good repair); allow them to dry thoroughly before
restoring varnish or other surface coatings. Category II
5. Contain dust and debris during remediation and repair as outlined in air recommendations (Air: IIG 4,
5). Category II
Regardless of the original source of water damage (e.g., flooding versus water leaks from point-of-use fixtures
or roofs), remove wet, absorbent structural items (e.g., carpeting, wallboard, and wallpaper) and cloth furnishings
if they cannot be easily and thoroughly cleaned and dried within 72 hours (e.g., moisture content
<20% as determined by moisture meter readings); replace with new materials as soon as the underlying structure is declared by the facility engineer to be thoroughly dry
(2,47,159,160). Category IB
IV. Additional Engineering Measures as Indicated by Epidemiologic Investigation for Controlling Waterborne, Health-Care--Associated Legionnaires Disease
When using a pulse or one-time decontamination method, superheat the water by flushing each outlet for
>5 minutes with water at
160ºF--170ºF
(71ºC--77ºC) or hyperchlorinate the system by flushing all outlets for
>5 minutes with water containing
>2 mg/L (>2 ppm) free residual chlorine using a chlorine-based product registered
by the EPA for water treatment (e.g., sodium hypochlorite [chlorine bleach])
(153,155,161--164). Category IB
After a pulse treatment, maintain both the heated water temperature at the return and the cold water temperature
per the recommendation (Water: II A) wherever practical and permitted by state codes, or chlorinate heated water
to achieve 1--2 mg/L (1--2 ppm) free residual chlorine at the tap by using a chlorine-based product registered by
the EPA for water treatment (e.g., sodium hypochlorite [bleach])
(153,165--169). Category IC (States;
ASHRAE: 12:2000)
Explore engineering or educational options (e.g., install preset thermostatic mixing valves in point-of-use fixtures
or post warning signs at each outlet) to minimize the risk of scalding for patients, visitors, and staff. Category II
No recommendation is offered for treating water in the facility's distribution system with chlorine dioxide,
heavy-metal ions (e.g., copper or silver), monochloramines, ozone, or UV light
(170--188). Unresolved issue
V. General Infection-Control Strategies for Preventing Legionnaires Disease
Conduct an infection-control risk assessment of the facility to determine if patients at risk or
severely immunocompromised patients are present
(27,189,190). Category IB
Implement general strategies for detecting and preventing Legionnaires disease in facilities that do not provide
care for severely immunocompromised patients (i.e., facilities that do not have HSCT or solid-organ
transplant programs) (see Appendix)
(27,189,190). Category IB
1. Establish a surveillance process to detect health-care--associated Legionnaires disease
(27,189,190). Category IB
2. Inform health-care personnel (e.g., infection control, physicians, patient-care staff, engineering) regarding
the potential for Legionnaires disease to occur and measures to prevent and
control
health-care--associated legionellosis
(166,191). Category IB
3. Establish mechanisms to provide clinicians with laboratory tests (e.g., culture, urine antigen, direct
fluorescence assay [DFA], and serology) for the diagnosis of Legionnaires disease
(27,189). Category IB
Maintain a high index of suspicion for health-care--associated Legionnaires disease, and perform
laboratory diagnostic tests for legionellosis on suspected cases, especially in patients at risk who do not require a PE for care (e.g., patients receiving systemic steroids; patients aged
>65 years; or patients with chronic underlying disease
(e.g., diabetes mellitus, congestive heart failure, or chronic obstructive lung disease)
(27,166,190,192--198). Category IA
Periodically review the availability and clinicians' use of laboratory diagnostic tests for Legionnaires disease in
the facility; if clinicians' use of the tests on patients with diagnosed or suspected pneumonia is limited,
implement measures (e.g., an educational campaign) to enhance clinicians' use of the test(s)
(193). Category IB
If one case of laboratory-confirmed, health-care--associated Legionnaires disease is identified, or if two or more
cases of laboratory-suspected, health-care-associated Legionnaires disease occur during a 6-month period, certain
activities should be initiated
(181,189,191,193,199,200). Category IB
1. Report the cases to state and local health departments where required. Category IC (States)
2. If the facility does not treat severely immunocompromised patients, conduct an epidemiologic
investigation, including retrospective review of microbiologic, serologic, and postmortem
data to look for
previously unidentified cases of health-care--associated Legionnaires disease, and begin intensive prospective surveillance for additional cases
(27,181,189,191,193,199,200). Category IB
3. If no evidence of continued health-care--associated transmission exists, continue intensive
prospective surveillance for >2 months after the initiation of surveillance
(27,181,
189,191,193,199,200). Category IB
If there is evidence of continued health-care--associated transmission (i.e., an outbreak), conduct an
environmental assessment to determine the source of
Legionella spp. (199--207). Category IB
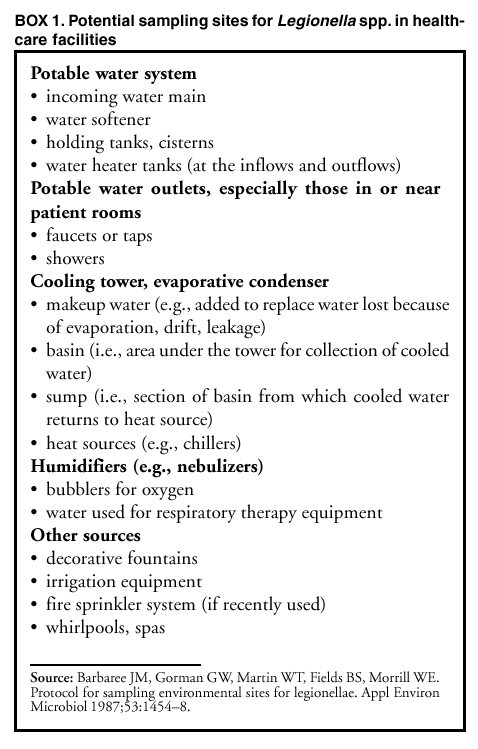
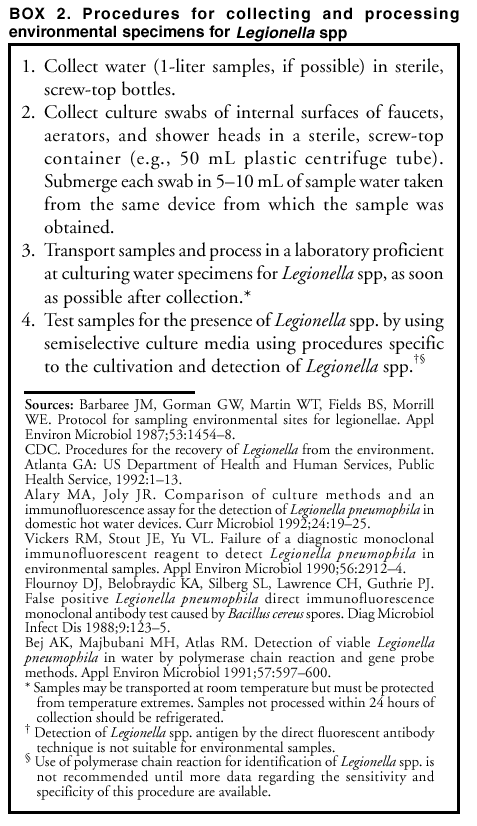
1. Collect water samples from potential aerosolized water sources (Box 1 and Box 2)
(208). Category IB
2. Save and subtype isolates of
Legionella spp. obtained from patients and the environment
(163,199--207,209). Category IB
3. If a source is identified, promptly institute water system decontamination measures per recommendations
(see Water IV) (164,210). Category IB
4. If Legionella spp. are detected in
>1 culture (e.g., conducted at 2-week intervals during 3 months), reassess
the control measures, modify them accordingly, and repeat the
decontamination procedures; consider intensive
use of techniques used in the initial decontamination, or a combination of superheating and hyperchlorination (27,210,211). Category
IB
If an environmental source is not identified during a Legionnaires disease outbreak, continue surveillance for
new cases for >2 months. Either defer decontamination pending identification of the source of
Legionella spp. or proceed with decontamination of the hospital's water distribution system, with special attention to areas involved in the outbreak. Category II
No recommendation is offered regarding routine culturing of water systems in health-care facilities that do not
have patient-care areas (i.e., PE or transplant units) for persons at high risk for
Legionella spp. infection (see Appendix)
(161,165,167, 198,212--214). Unresolved issue
No recommendation is offered regarding the removal of faucet aerators in areas for immunocompetent
patients. Unresolved issue
Keep adequate records of all infection-control measures and environmental test results for potable water
systems. Category II
VI. Preventing Legionnaires Disease in Protective Environments and Transplant Units
When implementing strategies for preventing Legionnaires disease among severely immunocompromised
patients housed in facilities with HSCT or solid-organ transplant programs, incorporate these specific surveillance and epidemiologic measures in addition to the steps outlined previously (see Appendix).
1. Maintain a high index of suspicion for legionellosis in transplant patients even when environmental
surveillance cultures do not yield legionellae
(189,215). Category IB
2. If a case occurs in a severely immunocompromised patient, or if severely immunocompromised patients
are present in high-risk areas of the hospital (e.g., PE or transplant units) and
cases are identified elsewhere in
the facility, conduct a combined epidemiologic and environmental investigation to determine the source
of Legionella spp. (189,210). Category IB
Implement culture strategies and potable water and fixture treatment measures in addition to those previous
outlined (Water: V). Category II
1. Depending on state regulations on potable water temperature in public buildings
(216), hospitals housing patients at high risk for health-care--associated legionellosis should either
maintain heated water with a minimum return temperature of
>124ºF
(>51ºC) and cold water at
<68ºF (<20ºC), or chlorinate heated water to achieve 1--2 mg/L (1--2 ppm) of free
residual chlorine at the tap (153--155,165,167--169,217). Category II
2. Periodic culturing for legionellae in potable water samples from HSCT or solid-organ transplant units can
be performed as part of a comprehensive strategy to prevent Legionnaires
disease in these units (37,154,189,218). Category II
3. No recommendation is offered regarding the optimal methodology (i.e., frequency or number of sites)
for environmental surveillance cultures in HSCT or solid-organ transplant units.
Unresolved issue
4. In areas with patients at risk, when
Legionella spp. are not detectable in unit water, remove, clean, and
disinfect shower heads and tap aerators monthly by using a chlorine-based,
EPA-registered product. If an EPA-registered chlorine disinfectant is not available, use a chlorine bleach solution (500--615 ppm [1:100 v/v dilution]) (153,187). Category II
If Legionella spp. are determined to be present in the water of a transplant unit, implement certain measures
until Legionella spp. are no longer detected by culture.
1. Decontaminate the water supply as outlined previously (Water: IV)
(27,37,153,164,210). Category IB
2. Do not use water from the faucets in patient-care rooms to avoid creating infectious aerosols
(37,219). Category IB
3. Restrict severely immunocompromised patients from taking showers
(37,219). Category IB
4. Use water that is not contaminated with
Legionella spp. for HSCT patients' sponge baths
(37,219). Category IB
5. Provide patients with sterile water for tooth brushing, drinking, and for flushing nasogastric tubing
during legionellosis outbreaks (37,219). Category IB
Do not use large-volume room air humidifiers that create aerosols (e.g., by Venturi principle, ultrasound, or
spinning disk) unless they are subjected to high-level disinfection and filled only with sterile water (27,37,201,220). Category IB
VII. Cooling Towers and Evaporative Condensers
When planning construction of new health-care facilities, locate cooling towers so that the drift is directed
away from the air-intake system, and design the towers to minimize the volume of aerosol drift
(153,203,221). Category IC (ASHRAE 12-2000)
Implement infection-control procedures for operational cooling towers
(153,203,222). Category IC (ASHRAE 12-2000)
1. Install drift eliminators
(153,203,222). Category IC (ASHRAE 12-2000)
2. Use an effective EPA-registered biocide on a regular basis
(153). Category IC (ASHRAE 12-2000)
3. Maintain towers according to manufacturers' recommendations, and keep detailed maintenance and
infection-control records, including environmental test results from legionellosis
outbreak investigations (153). Category IC (ASHRAE 12-2000)
If cooling towers or evaporative condensers are implicated in health-care--associated legionellosis, decontaminate
the cooling-tower system (199,203,221,223). Category IB
VIII. Dialysis Water Quality and Dialysate
Adhere to current AAMI standards for quality-assurance performance of devices and equipment used to treat,
store, and distribute water in hemodialysis centers (both acute and maintenance [chronic] settings) and for the preparation of concentrates and dialysate
(224--235). Category IA, IC (AAMI: American National Standards Institute
[ANSI]/AAMI RD5:1992, ANSI/AAMI RD47:1993)
No recommendation is offered regarding whether more stringent requirements for water quality should be
imposed in hemofiltration and hemodiafiltration. Unresolved issue
Conduct microbiologic testing specific to water in dialysis settings
(229,230,236--238). Category IA, IC (AAMI: ANSI/AAMI RD5:1992, ANSI/AAMI RD47:1993, RD62:2001)
1. Perform bacteriologic assays of water and dialysis fluids at least once a month and during outbreaks by
using standard quantitative methods
(236--238). Category IA, IC (AAMI:
ANSI/AAMI RD62:2001)
a. Assay for heterotrophic, mesophilic bacteria (e.g.,
Pseudomonas spp).
b. Do not use nutrient-rich media (e.g., blood agar or chocolate agar).
2. In conjunction with microbiologic testing, perform endotoxin testing on product water used to
reprocess dialyzers for multiple use
(229,230,239--242). Category IA, IC (AAMI:
ANSI/AAMI RD5:1992,
ANSI/AAMI RD47:1993)
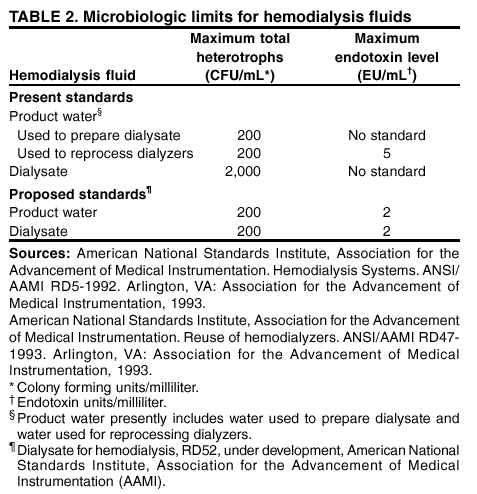
3. Ensure that water does not exceed the limits for microbial counts and endotoxin concentrations (Table 2)
(229--231). Category IA, IC (AAMI: ANSI/AAMI RD5:1992,
ANSI/AAMI RD47:1993)
Disinfect water distribution systems in dialysis settings at least weekly
(226--228,231,236). Category IA, IC (AAMI: ANSI/AAMI RD62:2001)
Wherever practical, design and engineer water systems in dialysis settings to avoid incorporating joints,
dead-end pipes, and unused branches and taps that can harbor bacteria
(226-- 228,231,236). Category IA, IC (AAMI:
ANSI/AAMI RD62:2001)
When storage tanks are used in dialysis systems, they should be routinely drained, disinfected with an
EPA-registered product, and fitted with an ultrafilter or pyrogenic filter (membrane filter with a pore size sufficient to remove particles and molecules >1 kilodalton) installed in the water line distal to the storage tank (236). Category IC (AAMI: ANSI/AAMI RD62:2001)
IX. Ice Machines and Ice
Do not handle ice directly by hand, and wash hands before obtaining ice. Category II
Use a smooth-surface ice scoop to dispense ice
(243,244). Category II
1. Keep the ice scoop on a chain short enough that the scoop cannot touch the floor or keep the scoop on a
clean, hard surface when not in use
(243,244). Category II
2. Do not store the ice scoop in the ice bin. Category II
Do not store pharmaceuticals or medical solutions on ice intended for consumption; use sterile ice to keep
medical solutions cold, or use equipment specifically manufactured for this purpose
(244,245). Category IB
Machines that dispense ice are preferred to those that require ice to be removed from bins or chests with a
scoop (246,247). Category II
Limit access to ice-storage chests, and keep container doors closed except when removing ice
(244). Category II
Clean, disinfect, and maintain ice-storage chests on a regular basis. Category II
1. Follow the manufacturer's instructions for cleaning. Category II
2. Use an EPA-registered disinfectant suitable for
use on ice machines, dispensers, or storage chests in accordance
with label instructions. Category II
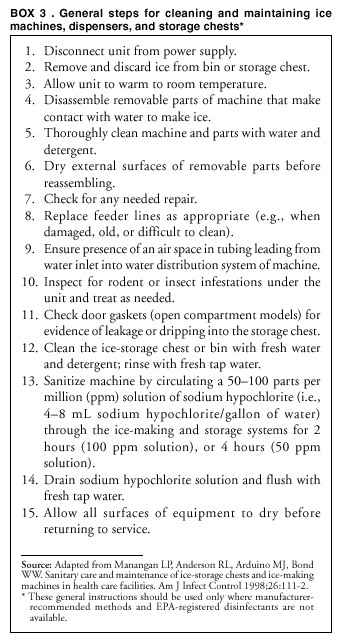
3. If instructions and EPA-registered disinfectants suitable for use on ice machines are not available, use a
general cleaning/disinfecting regimen (Box 3)
(244). Category II
4. Flush and clean ice machines and dispensers if they have not been disconnected before anticipated lengthy
water disruptions. Category II
Install proper air gaps where the condensate lines meet the waste lines. Category II.
Conduct microbiologic sampling of ice, ice chests, and ice-making machines and dispensers where indicated
during an epidemiologic investigation
(244,248,249). Category IB
X. Hydrotherapy Tanks and Pools
Drain and clean hydrotherapy equipment (e.g., Hubbard tanks, tubs, whirlpools, whirlpool spas, or birthing
tanks) after each patient's use, and disinfect equipment surfaces and components by using an EPA-registered product in accordance with the manufacturer's instructions. Category II
In the absence of an EPA-registered product for water treatment, add sodium hypochlorite to the water:
1. Maintain a 15-ppm chlorine residual in the water of small hydrotherapy tanks, Hubbard tanks, and tubs
(250). Category II
2. Maintain a 2--5-ppm chlorine residual in the water of whirlpools and whirlpool spas
(251). Category II
3. If the pH of the municipal water is in the basic range (e.g., when chloramine is used as the primary
drinking water disinfectant in the community), consult the facility engineer regarding
the possible need to adjust the
pH of the water to a more acidic level before disinfection, to enhance the biocidal activity of the chlorine (252). Category II
Clean and disinfect hydrotherapy equipment after using tub liners. Category II
Clean and disinfect inflatable tubs unless they are single-use equipment. Category II
No recommendation is offered regarding the use of antiseptic chemicals (e.g., chloramine-T) in the water
during hydrotherapy sessions. Unresolved issue
Conduct a risk assessment of patients before their use of large hydrotherapy pools, deferring patients with
draining wounds or fecal incontinence from pool use until their condition resolves. Category II
For large hydrotherapy pools, use pH and chlorine residual levels appropriate for an indoor pool as provided by
local and state health agencies. Category IC (States)
No recommendation is offered regarding the use in health-care settings of whirlpool or spa equipment
manufactured for home or recreational use. Unresolved issue
XI. Miscellaneous Medical Equipment Connected to Water Systems
Clean, disinfect, and maintain AER equipment according to the manufacturer's instructions and
relevant scientific literature to prevent inadvertent contamination of endoscopes and bronchoscopes with waterborne microorganisms (253--257). Category IB
1. To rinse disinfected endoscopes and bronchoscopes, use water of the highest quality practical for the
system's engineering and design (e.g., sterile water or bacteriologically filtered
water [water filtered through 0.1--0.2-µm filters]) (254,256--258). Category IB
2. Dry the internal channels of the reprocessed endoscope or bronchoscope by using a proven method (e.g.,
70% alcohol followed by forced-air treatment) to lessen the potential for
proliferation of waterborne microorganisms and to help prevent biofilm formation
(259--263). Category IB
Use water that meets nationally recognized standards set by the EPA for drinking water (<500 CFU/mL
for heterotrophic plate count) for routine dental treatment output water
(264--267). Category IC (EPA: 40 CFR 1 Part 141, Subpart G)
Take precautions to prevent waterborne contamination of dental unit water lines and instruments.
1. After each patient, discharge water and air for a minimum of 20--30 seconds from any dental device
connected to the dental water system that enters a patient's mouth (e.g.,
handpieces, ultrasonic scalers, or air/water syringes) (265,268). Category II
2. Consult with dental water-line manufacturers to 1) determine suitable methods and equipment to obtain
the recommended water quality; and 2) determine appropriate methods for
monitoring the water to ensure quality
is maintained (265,269). Category II
3. Consult with the dental unit manufacturer regarding the need for periodic maintenance of antiretraction
mechanisms (268,269). Category IB
Recommendations ---Environmental Services
I. Cleaning and Disinfecting Strategies for Environmental Surfaces in Patient-Care Areas
Select EPA-registered disinfectants, if available, and use them in accordance with the manufacturer's
instructions (270--272). Category IC (EPA: 7 United States Code [USC] § 136 et seq.)
Do not use high-level disinfectants/liquid chemical sterilants for disinfection of either noncritical instruments
and devices or any environmental surfaces; such use is counter to label instructions for these toxic chemicals (273--278). Category IC (Food and Drug Administration [FDA]: 21 CFR 801.5, 807.87.e)
Follow manufacturers' instructions for cleaning and maintaining noncritical medical equipment. Category II
In the absence of a manufacturer's cleaning instructions, follow certain procedures.
1. Clean noncritical medical equipment surfaces with a detergent/disinfectant. This may be followed by
an application of an EPA-registered hospital disinfectant with or without a
tuberculocidal claim (depending on
the nature of the surface and the degree of contamination), in accordance with germicide label instructions (274). Category II
2. Do not use alcohol to disinfect large environmental surfaces
(273). Category II
3. Use barrier protective coverings as appropriate for noncritical surfaces that are 1) touched frequently with
gloved hands during the delivery of patient care; 2) likely to become
contaminated with blood or body substances; or 3) difficult to clean (e.g., computer keyboards)
(265). Category II
Keep housekeeping surfaces (e.g., floors, walls, tabletops) visibly clean on a regular basis and clean up spills
promptly (279). Category II
1. Use a one-step process and an EPA-registered hospital detergent/disinfectant designed for general
housekeeping purposes in patient-care areas where 1) uncertainty exists as to the
nature of the soil on the surfaces (e.g., blood or body fluid contamination versus routine dust or dirt); or 2) uncertainty exists regarding the presence
of multidrug resistant organisums
on such surfaces (272,274,280,281). Category II
2. Detergent and water are adequate for cleaning surfaces in nonpatient-care areas (e.g., administrative
offices). Category II
3. Clean and disinfect high-touch surfaces (e.g., doorknobs, bed rails, light switches, and surfaces in and
around toilets in patients' rooms) on a more frequent schedule than minimal-
touch housekeeping surfaces. Category II
4. Clean walls, blinds, and window curtains in patient-care areas when they are visibly dusty or soiled
(270,282--284). Category II
Do not perform disinfectant fogging in patient-care areas
(270,285). Category IB
Avoid large-surface cleaning methods that produce mists or aerosols, or disperse dust in patient-care
areas (37,48,51,73). Category IB
Follow proper procedures for effective uses of mops, cloths, and solutions. Category II
1. Prepare cleaning solutions daily or as needed, and replace with fresh solution frequently according to
facility policies and procedures (280,281). Category II
2. Change the mop head at the beginning of each day and also as required by facility policy, or after cleaning
up large spills of blood or other body substances. Category II
3. Clean mops and cloths after use and allow to
dry before reuse; or use single-use, disposable mop heads and
cloths (282,286--288). Category II
After the last surgical procedure of the day or night, wet vacuum or mop operating room floors with a
single-use mop and an EPA-registered hospital disinfectant
(114). Category IB
Do not use mats with tacky surfaces at the entrances to operating rooms or infection-control suites
(114). Category IB
Use appropriate dusting methods for patient-care areas designated for immunocompromised patients (e.g.,
HSCT patients) (37,40,280). Category IB
1. Wet-dust horizontal surfaces daily by moistening a cloth with a small amount of an EPA-registered
hospital detergent/disinfectant (37,40,280). Category IB
2. Avoid dusting methods that disperse dust (e.g., feather-dusting)
(40). Category IB
Keep vacuums in good repair and equip vacuums with HEPA filters for use areas with patients at
risk (37,40,280,289). Category IB
Close the doors of immunocompromised patients' rooms when vacuuming, waxing, or buffing corridor floors
to minimize exposure to airborne dust
(37,40,289). Category IB
When performing low- or intermediate-level disinfection of environmental surfaces in nurseries and neonatal
units, avoid unnecessary exposure of neonates to disinfectant residues on these surfaces by using EPA-registered germicides in accordance with manufacturers' instructions and safety advisories
(271,290--292). Category IB, IC (EPA: 7 USC § 136 et seq.)
1. Do not use phenolics or any other chemical germicide to disinfect bassinets or incubators during an infant's
stay (271,290--292). Category IB
2. Rinse disinfectant-treated surfaces, especially those treated with phenolics, with water
(290--292). Category IB
When using phenolic disinfectants in neonatal units, prepare solutions to correct concentrations in accordance
with manufacturers' instructions, or use premixed formulations
(271,290--292). Category IB, IC (EPA: 7 USC § 136
et seq.)
II. Cleaning Spills of Blood and Body Substances
Promptly clean and decontaminate spills of blood or other potentially infectious materials
(293--300). Category IB, IC (OSHA: 29 CFR 1910.1030 § d.4.ii.A)
Follow proper procedures for site decontamination of spills of blood or blood-containing body fluids
(293--300). Category IC (OSHA: 29 CFR 1910.1030 § d.4.ii.A)
1. Use protective gloves and other PPE appropriate for this task
(293). Category IC (OSHA: 29 CFR 1910.1030
§ d.3.i, ii)
2. If the spill contains large amounts of blood or body fluids, clean the visible matter with disposable
absorbent material, and discard the used cleaning materials in appropriate, labeled
containers
(293,298,299,301,302). Category IC (OSHA: 29 CFR 1910.1030 § d.4.iii.B)
3. Swab the area with a cloth or paper towels moderately wetted with disinfectant, and allow the surface to
dry (293,301). Category IC (OSHA: 29 CFR 1910.1030 § d.4.ii.A)
Use germicides registered by the EPA for use as hospital disinfectants and labeled tuberculocidal or
registered germicides on the EPA Lists D and E (i.e., products with specific label claims for HIV or hepatitis B virus [HBV])
in accordance with label instructions to decontaminate spills of blood and other body fluids
(293,301,303). Category IC (OSHA 29 CFR 1910.1030 § d.4.ii. A memorandum 2/28/97; compliance document [CPL] 2-2.44D [11/99])
An EPA-registered sodium hypochlorite product is preferred, but if such products are not available, generic
sodium hypochlorite solutions (e.g., household chlorine bleach) may be used.
1. Use a 1:100 dilution (500--615 ppm available chlorine) to decontaminate nonporous surfaces
after cleaning a spill of either blood or body fluids in patient-care settings
(301,304).
Category IB
2. If a spill involves large amounts of blood or body fluids, or if a blood or culture spill occurs in the laboratory,
use a 1:10 dilution (5,000--6,150 ppm available chlorine) for the first
application of germicide before
cleaning (279,301). Category IB
III. Carpeting and Cloth Furnishings
Vacuum carpeting in public areas of health-care facilities and in general patient-care areas regularly with
well-maintained equipment designed to minimize dust dispersion
(280). Category II
Periodically perform a thorough, deep cleaning of carpeting as determined by facility policy by using a method
that minimizes the production of aerosols and leaves little or no residue
(44). Category II
Avoid use of carpeting in high-traffic zones in patient-care areas or where spills are likely (e.g., burn therapy
units, operating rooms, laboratories, or intensive care units)
(44,305,306). Category IB
Follow appropriate procedures for managing spills on carpeting.
1. Spot-clean blood or body substance spills promptly
(293,301,304,307). Category IC (OSHA: 29
CFR 1910.1030 § d.4.ii.A, interpretation)
2. If a spill occurs on carpet tiles, replace any tiles contaminated by blood and body fluids or body substances
(307). Category IC (OSHA 29 CFR 1910.1030 § d.4.ii interpretation)
Thoroughly dry wet carpeting to prevent the growth of fungi; replace carpeting that remains wet after 72
hours (37,160). Category IB
No recommendation is offered regarding the routine use of fungicidal or bactericidal treatments for carpeting
in public areas of a health-care facility or in general patient-care areas. Unresolved issue
Do not use carpeting in hallways and patient rooms in areas housing immunosuppressed patients (e.g., PE
areas) (37,44). Category IB
Avoid using upholstered furniture and furnishings in high-risk patient-care areas and in areas with
increased potential for body substance contamination (e.g., pediatrics units)
(37). Category II
No recommendation is offered regarding whether upholstered furniture and furnishings should be avoided in
general patient-care areas. Unresolved issue
1. Maintain upholstered furniture in good repair. Category II
2. Maintain the surface integrity of the upholstery by repairing tears and holes. Category II
3. If upholstered furniture in a patient's room requires cleaning to remove visible soil or body
substance contamination, move that item to a maintenance area where it can be adequately
cleaned with a process appropriate for the type of upholstery and nature of the soil. Category II
IV. Flowers and Plants in Patient-Care Areas
Flowers and potted plants need not be restricted from areas for immunocompetent patients
(308--311). Category II
Designate care and maintenance of flowers and potted plants to staff not directly involved with patient care
(309). Category II
If plant or flower care by patient-care staff is unavoidable, instruct the staff to wear gloves when handling plants
and flowers and perform hand hygiene after glove removal
(309). Category II
Do not allow fresh or dried flowers, or potted plants, in patient-care areas for immunosuppressed
patients (37,51,308,312). Category II
V. Pest Control
Develop pest-control strategies, with emphasis on kitchens, cafeterias, laundries, central sterile supply
areas, operating rooms, loading docks, construction activities, and other areas prone to infestations
(313--315). Category II
Install screens on all windows that open to the outside; keep screens in good repair
(314). Category IB
Contract for routine pest control service by a credentialed pest-control specialist who will tailor the application
to the needs of a health-care facility (315). Category II
Place laboratory specimens (e.g., fixed sputum smears) in covered containers for overnight storage
(316,317). Category II
VI. Special Pathogens
Use appropriate hand hygiene, PPE (e.g., gloves),
and isolation precautions during cleaning and
disinfecting procedures (146,274,318,319). Category IB
Use standard cleaning and disinfection protocols to control environmental contamination with
antibiotic-resistant, gram-positive cocci (e.g., methicillin-resistant Staphylococcus aureus, vancomycin intermediate sensitive Staphylococcus aureus, or vancomycin-resistant Enterococcus [VRE]) (318,320--322). Category IB
1. Pay close attention to cleaning and disinfection of high-touch surfaces in patient-care areas (e.g., bed rails,
carts, charts, bedside commodes, bed rails, doorknobs, or faucet handles)
(318,320--322). Category IB
2. Ensure compliance by housekeeping staff with cleaning and disinfection procedures
(318,320--322). Category IB
3. Use EPA-registered chemical germicides appropriate for the surface to be disinfected (e.g., either low-
or intermediate-level disinfection) as specified by the manufacturer's
instructions
(271,322--327). Category IB, IC (EPA: 7 USC § 136 et seq.)
4. When contact precautions are indicated for patient care, use disposable patient-care items (e.g., blood
pressure cuffs) wherever possible to minimize cross-contamination with
multiple-resistant microorganisms
(328). Category IB
5. Follow these same surface-cleaning and disinfecting measures for managing the environment of VRSA
patients (320--322,327). Category II
Environmental-surface culturing can be used to
verify the efficacy of hospital policies and procedures before and
after cleaning and disinfecting rooms that house patients with VRE
(318,329--333). Category II
1. Obtain prior approval from infection-control staff and the clinical laboratory before performing
environmental-surface culturing. Category II
2. Infection-control staff, with clinical laboratory staff consultation, must supervise all environmental
culturing. Category II
Thoroughly clean and disinfect environmental and medical equipment surfaces on a regular basis by using
EPA-registered disinfectants in accordance with manufacturers' instructions
(271,274,319, 334). Category IB, IC (EPA: 7 USC § 136 et seq.)
Advise families, visitors, and patients regarding the importance of hand hygiene to minimize the spread of
body substance contamination (e.g., respiratory secretions or fecal matter) to surfaces
(274). Category II
Do not use high-level disinfectants (i.e., liquid chemical sterilants) on environmental surfaces; such use
is inconsistent with label instructions because of the toxicity of the chemicals
(270,273,274,278). Category IC (FDA: 21 CFR 801.5, 807.87.e)
Because no EPA-registered products are specific for inactivating
Clostridium difficile spores, use
hypochlorite-based products for disinfection of environmental surfaces in accordance with guidance from the scientific literature in those patient-care areas where surveillance and epidemiology indicate ongoing transmission of
C. difficile (274,319,334). Category II
No recommendation is offered regarding the use of specific EPA-registered hospital disinfectants with respect
to environmental control of C. difficile. Unresolved issue
Apply standard cleaning and disinfection procedures to control environmental contamination with respiratory
and enteric viruses in pediatric-care units and care areas for immunocompromised patients
(280,335). Category IC (EPA: 7 USC § 136 et seq.)
Clean surfaces that have been contaminated with body substances; perform low- to intermediate-level
disinfection on cleaned surfaces with an EPA-registered disinfectant in accordance with the manufacturer's instructions (271,293,335). Category IC (OSHA: 29 CFR 1910.1030 § d.4.ii.A; EPA: 7 USC § 136 et seq.)
Use disposable barrier coverings as appropriate to minimize surface contamination. Category II
Develop and maintain cleaning and disinfection procedures in patient-care areas to control
environmental contamination with agents of Creutzfeldt-Jakob disease (CJD), for which no EPA-registered product exists. Category II
1. In the absence of contamination with central nervous system tissue, extraordinary measures (e.g., use of
2N sodium hydroxide [NaOH] or applying full-strength sodium hypochlorite)
are not needed for routine cleaning
or terminal disinfection of a room housing a confirmed or suspected CJD patient
(273,336). Category II
2. After removing gross tissue from the surface, use either 1N NaOH or a sodium hypochlorite solution
containing approximately 10,000--20,000 ppm available chlorine (dilutions of
1:5 to 1:3 v/v, respectively, of U.S.
household chlorine bleach; contact the manufacturers of commercially available sodium hypochlorite products for advice) to decontaminate
operating room or autopsy surfaces with central nervous system or cerebral spinal
fluid contamination from a diagnosed or suspected CJD patient
(273,337--342). Category II
a. The contact time for the chemical used during this process should be 30 min--1 hour
(339,340,342).
b. Blot up the chemical with absorbent material and rinse the treated surface thoroughly with water.
c. Discard the used, absorbent material into appropriate waste containers.
3. Use disposable, impervious covers to minimize body substance contamination to autopsy tables and
surfaces (340,342). Category II
Use standard procedures for containment, cleaning, and decontamination of blood spills on surfaces as
previously described (Environmental Services: II)
(293). Category IC (OSHA: 29 CFR 1910.1030 § d.4.ii.A)
1. Wear PPE appropriate for a surface decontamination and cleaning task
(293,336). Category IC (OSHA 29 CFR 1910.1030 § d.3.i, ii)
2. Discard used PPE by using routine disposal procedures or decontaminate reusable PPE as appropriate
(293,336). Category IC (OSHA 29 CFR 1910.1030 § d.3.viii)
Recommendations ---Environmental Sampling
I. General Information
Do not conduct random, undirected, microbiologic sampling of air, water, and environmental surfaces in
health-care facilities (270,343). Category IB
When indicated, conduct microbiologic sampling as part of an epidemiologic investigation or during assessment
of hazardous environmental conditions to detect contamination or verify abatement of a hazard
(270,343). Category IB
Limit microbiologic sampling for quality assurance purposes to 1) biologic monitoring of sterilization processes;
2) monthly cultures of water and dialysate in hemodialysis units; and 3) short-term evaluation of the impact
of infection-control measures or changes in infection-control protocols
(270,343). Category IB
II. Air, Water, and Environmental Surface Sampling
When conducting any form of environmental sampling, identify existing comparative standards and fully
document departures from standard methods
(343--347). Category II
Select a high-volume air sampling device if anticipated levels of microbial airborne contamination are expected to
be low (345,346,348,349). Category II
Do not use settle plates to quantify the concentration of airborne fungal spores
(348). Category II
When sampling water, choose growth media and incubation conditions that will facilitate recovery of
waterborne organisms (344). Category II
When using a sample/rinse method for sampling an environmental surface, develop and document a procedure
for manipulating the swab, gauze, or sponge in a reproducible manner so that results are comparable
(347). Category II
When environmental samples and patient specimens are available for comparison, perform the laboratory analysis
on the recovered microorganisms down to the species level at a minimum, and beyond the species level if possible (343). Category II
Recommendations ---Laundry and Bedding
I. Employer Responsibilities
Employers must launder workers' personal protective garments or uniforms that are contaminated with blood
or other potentially infectious materials
(293). Category IC (OSHA: 29 CFR 1910.1030 § d.3.iv)
II. Laundry Facilities and Equipment
Maintain the receiving area for contaminated textiles at negative pressure compared with the clean areas of
the laundry in accordance with AIA construction standards in effect during the time of facility construction (1,350--352). Category IC (AIA: 7.23.B1, B2)
Ensure that laundry areas have handwashing facilities and products and appropriate PPE available for
workers (1,293). Category IC (AIA: 7.23.D4; OSHA: 29 CFR 1910.1030 § d.2.iii)
Use and maintain laundry equipment according to manufacturers' instructions
(353,354). Category II
Do not leave damp textiles or fabrics in machines overnight
(353). Category II
Disinfection of washing and drying machines in residential care is not needed as long as gross soil is
removed from items before washing and proper washing and drying procedures are used. Category II
III. Routine Handling of Contaminated Laundry
Handle contaminated textiles and fabrics with minimum agitation to avoid contamination of air, surfaces,
and persons (36,293,355,356). Category IC (OSHA: 29 CFR 1910.1030 § d.4.iv)
Bag or otherwise contain contaminated textiles and fabrics at the point of use
(293). Category IC (OSHA: 29 CFR 1910.1030 § d.4.iv)
1. Do not sort or prerinse contaminated textiles or fabrics in patient-care areas
(293). Category IC (OSHA: 29 CFR 1910.1030 § d.4.iv)
2. Use leak-resistant containment for textiles and fabrics contaminated with blood or body substances
(293,355). Category IC (OSHA: 29 CFR 1910.1030 § d.4.iv)
3. Identify bags or containers for contaminated textiles with labels, color coding, or other alternative means
of communication as appropriate (293). Category IC (OSHA: 29 CFR
1910.1030 § d.4.iv)
Covers are not needed on contaminated textile hampers in patient-care areas. Category II
If laundry chutes are used, ensure that they are properly designed, maintained, and used in a manner to
minimize dispersion of aerosols from contaminated laundry
(357--361). Category IC (AAMI: ANSI/AAMI ST65:2000)
1. Ensure that laundry bags are closed before tossing the filled bag into the chute. Category II
2. Do not place loose items in the laundry chute. Category II
Establish a facility policy to determine when textiles or fabrics should be sorted in the laundry facility (i.e., before
or after washing) (362,363). Category II
IV. Laundry Process
If hot-water laundry cycles are used, wash with detergent in water
>160ºF
(>71ºC) for >25 minutes
(1,270). Category IC (AIA: 7.31.E3)
No recommendation is offered regarding a hot-water temperature setting and cycle duration for items laundered
in residence-style health-care facilities. Unresolved issue
Follow fabric-care instructions and special laundering requirements for items used in the facility
(364). Category II
Choose chemicals suitable for low-temperature washing at proper use concentration if low-temperature
(<160ºF
[<70ºC ]) laundry cycles are used
(365--370). Category II
Package, transport, and store clean textiles and fabrics by methods that will ensure their cleanliness and
protect them from dust and soil during interfacility loading, transport, and unloading
(270). Category II
V. Microbiologic Sampling of Textiles
Do not conduct routine microbiologic sampling of clean textiles
(270,371). Category IB
Use microbiologic sampling during outbreak investigations if epidemiologic evidence indicates a role for
health-care textiles and clothing in disease transmission
(371). Category IB
VI. Special Laundry Situations
Use sterilized textiles, surgical drapes, and gowns for situations requiring sterility in patient care
(114). Category IB
Use hygienically clean textiles (i.e., laundered, but not sterilized) in neonatal intensive care units
(292,372). Category IB
Follow manufacturers' recommendations for cleaning fabric products, including those with coated or
laminated surfaces. Category II
Do not use dry cleaning for routine laundering in health-care facilities
(373--375). Category II
Use caution when considering use of antimicrobial mattresses, textiles, and clothing as replacements for
standard bedding and other fabric items; EPA has not approved public health claims asserting protection against human pathogens for such treated items (376). Category II
No recommendation is offered regarding using disposable fabrics and textiles versus durable goods. Unresolved issue
VII. Mattresses and Pillows
Keep mattresses dry; discard them if they remain wet or stained, particularly in burn units
(377--382). Category IB
Clean and disinfect mattress covers by using EPA-registered disinfectants that are compatible with the materials
to prevent the development of tears, cracks, or holes in the covers
(377--382). Category IB
Maintain the integrity of mattress and pillow covers. Category II
1. Replace mattress and pillow covers if they become torn or otherwise in need of repair. Category II
2. Do not stick needles into a mattress through the cover. Category II
Clean and disinfect moisture-resistant mattress covers between patient use by using an EPA-registered product
(377--382). Category IB
If using a mattress cover completely made of fabric, change these covers and launder between patient use
(377--382). Category IB
Launder pillow covers and washable pillows in the hot-water cycle between patients or when they
become contaminated with body substances
(382). Category IB
VIII. Air-Fluidized Beds
Follow manufacturers' instructions for air-fluidized bed maintenance and decontamination. Category II
Change the polyester filter sheet at least weekly or as indicated by the manufacturer
(383--386). Category II
Clean and disinfect the polyester filter sheet thoroughly, especially between patients, using an EPA-registered
product (383--386). Category IB
Consult the facility engineer to determine the proper placement of air-fluidized beds in negative-pressure
rooms (387). Category II
Recommendations --- Animals in Health-Care Facilities
I. General Infection-Control Measures for Animal Encounters
Minimize contact with animal saliva, dander, urine, and feces
(388--390). Category II
Practice hand hygiene after any animal contact
(146,270). Category II
1. Wash hands with soap and water, especially if hands are visibly soiled or contaminated with
proteinaceous material (146). Category II
2. Use either soap and water or alcohol-based hand rubs when hands are not visibly soiled or contaminated
(146). Category II
II. Animal-Assisted Activities and Resident Animal Programs
Avoid selection of nonhuman primates and reptiles
in animal-assisted activities, animal-assisted therapy, or
resident animal programs (391--393). Category IB
Enroll animals that are fully vaccinated for zoonotic diseases and that are healthy, clean, well-groomed, and
negative for enteric parasites or otherwise have completed recent anthelmintic treatment under the regular care of a veterinarian (391,394). Category II
Enroll animals that are trained with the assistance or under the direction of persons who are experienced in this
field (391). Category II
Ensure that animals are controlled by persons trained in providing activities or therapies safely, and who know
the animal's health status and behavior traits
(391,394). Category II
Take prompt action when an incident of biting or scratching by an animal occurs during an animal-assisted
activity or therapy.
1. Remove the animal permanently from these programs
(391). Category II
2. Report the incident promptly to appropriate authorities (e.g., infection-control staff, animal
program coordinator, or local animal control personnel)
(391). Category II
3. Promptly clean and treat scratches, bites, or other breaks in the skin. Category II
Perform an ICRA and work actively with the animal handler before conducting an animal-assisted activity or
therapy to determine whether the session should be held in a public area of the facility or in individual patient
rooms (391,394). Category II
Take precautions to mitigate allergic responses to animals. Category II
1. Minimize shedding of animal dander by bathing animals <24 hours before a visit
(391). Category II
2. Groom animals to remove loose hair before a visit, or use a therapy animal cape
(395). Category II
Use routine cleaning protocols for housekeeping surfaces after therapy sessions. Category II
Restrict resident animals, including fish in tanks, from access to patient-care areas, food-preparation areas,
dining areas, laundry, central sterile supply areas, sterile and clean supply storage areas, medication preparation areas, operating rooms, isolation areas, and PE areas. Category II
Establish a facility policy for regular cleaning of fish tanks, rodent cages, and bird cages, and any other
animal dwellings and assign this cleaning task to a nonpatient-care staff member; avoid splashing tank water
or contaminating environmental surfaces with animal bedding. Category II
III. Protective Measures for Immunocompromised Patients
Advise patients to avoid contact with animal feces, saliva, urine, or solid litter box material
(396). Category II
Promptly clean and treat scratches, bites, or other wounds that break the skin
(396). Category II
Advise patients to avoid direct or indirect contact with reptiles
(397). Category IB
Conduct a case-by-case assessment to determine if animal-assisted activities or animal-assisted therapy programs
are appropriate for immunocompromised patients
(394). Category II
No recommendation is offered regarding permitting pet visits to terminally ill immunocompromised patients
outside their PE units. Unresolved issue.
IV. Service Animals
Avoid providing facility access to nonhuman primates and reptiles as service animals
(393,397). Category IB
Allow service animals access to the facility in accordance with the Americans with Disabilities Act of 1990, unless
the presence of the animal creates a direct threat to other persons or a fundamental alteration in the nature of
services (389,398). Category IC (U.S. Department of Justice: 28 CFR § 36.302)
When a decision must be made regarding a service animal's access to any particular area of the health-care
facility, evaluate the service animal, patient, and health-care situation on a case-by-case basis to determine whether significant risk of harm exists and whether reasonable modifications in policies and procedures will mitigate this risk (398). Category IC (U.S. Department of Justice: 28 CFR § 36.208)
If a patient must be separated from his or her service animal while in the health-care facility 1) ascertain from
the person what arrangements have been made for supervision or care of the animal during this period of separation;
and 2) make appropriate arrangements to address the patient's needs in the absence of the service animal. Category II
V. Animals as Patients in Human Health-Care Facilities
Develop health-care facility policies to address the treatment of animals in human health-care facilities.
1. Use the multidisciplinary team approach to policy development, including public media relations efforts
to disclose and discuss these activities. Category II
2. Exhaust all veterinary facility, equipment, and instrument options before undertaking the procedure. Category II
3. Ensure that the care of the animal is supervised by a licensed veterinarian. Category II
When animals are treated in human health-care facilities, avoid treating animals in operating rooms or other
patient-care areas where invasive procedures are performed (e.g., cardiac catheterization laboratories or invasive nuclear medicine areas). Category II
Schedule the animal procedure for the last procedure of the day in the area, at a time when human patients are
not scheduled to be in the vicinity. Category II
Adhere strictly to standard precautions. Category II
Clean and disinfect environmental surfaces thoroughly by using an EPA-registered product in the room after the
animal has been removed. Category II
Allow sufficient ACH to clean the air and help remove airborne dander, microorganisms, and allergens (Table 1). Category II
Clean and disinfect using EPA-registered products or sterilize equipment that has been in contact with
the animal; or use disposable equipment. Category II
If reusable medical or surgical instruments are used in an animal procedure, restrict future use of these
instruments to animals only. Category II
VI. Research Animals in Health-Care Facilities
Use animals obtained from quality stock, or quarantine incoming animals to detect zoonotic diseases. Category II
Treat sick animals or remove them from the facility. Category II
Provide prophylactic vaccinations, as available, to animal handlers and contacts at high risk. Category II
Ensure proper ventilation through appropriate facility design and location
(399). Category IC (U.S. Department of Agriculture [USDA]: 7 USC 2131)
1. Keep animal rooms at negative pressure relative to corridors
(399). Category IC (USDA: 7 USC 2131)
2. Prevent air in animal rooms from recirculating elsewhere in the health-care facility
(399). Category IC (USDA: 7 USC 2131)
Keep doors to animal research rooms closed. Category II
Restrict access to animal facilities to essential personnel. Category II
Establish employee occupational health programs specific to the animal research facility, and coordinate
management of postexposure procedures specific to zoonoses with occupational health clinics in the health-care facility (400,401). Category IC (U.S. Department of Health and Human Services [DHHS]: Biosafety in Microbiological
and Biomedical Laboratories [BMBL]; OSHA: 29 CFR 1910.1030.132-139)
Document standard operating procedures for the unit
(400). Category IC (DHHS: BMBL)
Conduct routine employee training on worker safety concerns relevant to the animal research facility (e.g.,
working safely with animals, animal handling)
(400,401). Category IC (DHHS: BMBL; OSHA: 29 CFR
1910.1030.132--139)
Use precautions to prevent development of animal-induced asthma in animal workers
(400). Category IC (DHHS: BMBL)
Recommendations --- Regulated Medical Wastes
I. Categories of Regulated Medical Waste
Designate the following as major categories of medical waste that require special handling and disposal
precautions: 1) microbiology laboratory wastes [e.g., cultures and stocks of microorganisms]; 2) bulk
blood, blood products, blood, and bloody body fluid specimens; 3) pathology and anatomy waste; and 4) sharps [e.g., needles and scalpels] (270). Category II
Consult federal, state, and local regulations to determine if other waste items are considered regulated medical
wastes (293,402,403). Category IC (States; OSHA: 29 CFR 1910.1030 § g.2.1; Department of Transportation [DOT]:
49 CFR 171-180; U.S. Postal Service: CO23.8)
II. Disposal Plan for Regulated Medical Wastes
Develop a plan for the collection, handling, predisposal treatment, and terminal disposal of regulated medical
wastes (293,404). Category IC (States; OSHA: 29 CFR 1910.1030 § g.2.i)
Designate a person or persons as responsible for establishing, monitoring, reviewing, and administering the
plan. Category II
III. Handling, Transporting, and Storing Regulated Medical Wastes
Inform personnel involved in handling and disposal of potentially infective waste of possible health and
safety hazards; ensure that they are trained in appropriate handling and disposal methods
(293). Category IC (OSHA: 29 CFR 1910.1030 § g.2.i)
Manage the handling and disposal of regulated medical wastes generated in isolation areas by using the
same methods used for regulated medical wastes from other patient-care areas
(270). Category II
Use proper sharps disposal strategies (293). Category
IC (OSHA: 29 CFR 1910.1030 § d.4.iii.A)
1. Use a sharps container capable of maintaining its
impermeability after waste treatment to avoid subsequent
physical injuries during final disposal (293). Category
IC (OSHA: 29 CFR
1910.1030 § d.4.iii.A)
2. Place disposable syringes with needles, including sterile
sharps that are being discarded, scalpel blades, and other sharp
items into puncture-resistant containers located as close as
practical to the point of use (293). Category IC (OSHA:
29 CFR 1910.1030 § d.4.iii.A)
3. Do not bend, recap, or break used syringe needles before
discarding them into a container (36,293,405). Category
IC (OSHA: 29 CFR 1910.1030 § d.2.vii and § d.2.vii.A)
Store regulated medical wastes awaiting treatment in a
properly ventilated area inaccessible to vertebrate pests; use
waste containers that prevent development of noxious odors.
Category IC (States)
If treatment options are not available at the site where the
medical waste is generated, transport regulated medical wastes
in closed, impervious containers to the on-site treatment
location or to another facility for treatment as appropriate.
Category IC (States)
IV. Treatment and Disposal of Regulated Medical Wastes
Treat regulated medical wastes by using a method (e.g., steam sterilization, incineration, interment, or an
alternative treatment technology) approved by the appropriate authority having jurisdiction (AHJ) (e.g., state, Indian Health Service, or Veterans Administration) before disposal in a sanitary landfill. Category IC (States, AHJ)
Follow precautions for treating microbiologic wastes (e.g., amplified cultures and stocks of microorganisms)
(400). Category IC (DHHS: BMBL)
1. Biosafety level 4 laboratories must inactivate microbiologic wastes in the laboratory by using an
approved inactivation method (e.g., autoclaving) before transport to and disposal in a
sanitary landfill
(400). Category IC (DHHS: BMBL)
2. Biosafety level 3 laboratories must inactivate microbiologic wastes in the laboratory by using an
approved inactivation method (e.g., autoclaving) or incinerate them at the facility
before transport to and disposal in a sanitary landfill (400). Category IC (DHHS: BMBL)
Biosafety levels 1 and 2 laboratories should develop strategies to inactivate amplified microbial cultures and
stocks onsite by using an approved inactivation method (e.g., autoclaving) instead of packaging and shipping
untreated wastes to an offsite facility for treatment and disposal
(400,406--408). Category II
Laboratories that isolate select agents from clinical specimens must comply with federal regulations for
receipt, transfer, management, and appropriate disposal of these agents
(409). Category IC (DHHS: 42 CFR 72 § 72.6.i.1.iii)
Sanitary sewers may be used for safe disposal of blood, suctioned fluids, ground tissues, excretions, and
secretions, provided that local sewage discharge requirements are met and that the state has declared this to be an acceptable method of disposal (410). Category II
V. Special Precautions for Wastes Generated During Care of Patients with Rare Diseases
When discarding items contaminated with blood and body fluids from VHF patients, contain these
regulated medical wastes with minimal agitation during handling
(36,109). Category II
Manage properly contained wastes from areas providing care to VHF patients in accordance with
recommendations for other isolation areas (Regulated Medical Waste: III B)
(36,109,270). Category II
Decontaminate bulk blood and body fluids from VHF patients by using approved inactivation methods
(e.g., autoclaving or chemical treatment) before disposal
(36,109). Category IC, II (States)
When discarding regulated medical waste generated during the routine (i.e., nonsurgical) care of CJD
patients, contain these wastes and decontaminate them by using approved inactivation methods (e.g., autoclaving or incineration) appropriate for the medical waste category (e.g., blood, sharps, or pathological
waste) (36,270,273,336). Category IC, II (States)
Incinerate medical wastes (e.g., central nervous system tissues or contaminated disposable materials) from
brain autopsy or biopsy procedures of diagnosed or suspected CJD patients
(340,342). Category IB
References
The American Institute of Architects and The Facilities Guidelines Institute. Guidelines for design and construction of hospital and health
care facilities, 2001. Washington, DC: American Institute of Architects Press, 2001.
Arnow PM, Sadigh M, Costas C, Weil D, Chudy R. Endemic and epidemic aspergillosis associated with in-hospital replication of
Aspergillus organisms. J Infect Dis 1991;164:998--1002.
Streifel AJ. Design and maintenance of hospital ventilation systems and the prevention of airborne nosocomial infections [Chapter 80]. In:
Mayhall, CG, ed. Hospital epidemiology and infection control.
2nd ed. Philadelphia, PA: Lippincott Williams and Wilkins, 1999.
Pittet D, Huguenin T, Dharan S, et al. Unusual cause of lethal pulmonary aspergillosis in patients with chronic obstructive pulmonary disease. Am
J Respir Crit Care Med 1996;154(2 Pt 1):541--4.
US Environmental Protection Agency, Office of Air and Radiation, and US Department of Health and Human Services, National Institute
of Occupational Safety and Health. Building air quality: a guide for building owners and facility managers. Washington, DC: 1991; DHHS
publication (NIOSH)91-114 and EPA/400/1--91/033. Available at
http://www.cdc.gov/niosh/baqtoc.html.
Rao CY, Burge HA, Chang JC. Review of quantitative standards and guidelines for fungi in indoor air. J Air & Waste Manage Assoc
1996;46:899--908.
Beck-Sagué CM, Dooley SW, Hutton MD, et al. Hospital outbreak of
multidrug-resistant Mycobacterium tuberculosis
infections: factors in transmission to staff and HIV-infected patients. JAMA 1992;268:1280--6.
Dooley SW, Villarino ME, Lawrence M, et al. Nosocomial transmission of tuberculosis in a hospital unit for HIV-infected patients.
JAMA 1992;267:2632--4.
Sarubbi FA Jr, Kopf HB, Wilson MB, McGinnis MR, Rutala WA. Increased recovery of
Aspergillus flavus from respiratory specimens during
hospital construction. Am Rev Respir Dis 1982;125:33--8.
Streifel AJ, Stevens PP, Rhame FS. In-hospital source of airborne
Penicillium species spores. J Clin Microbiol 1987;25:1--4.
Hansen W. The need for an integrated indoor air quality program. In: Hansen W, ed. A guide to managing indoor air quality in health
care organizations. Oakbrook Terrace, IL: Joint Commission on Accreditation of Healthcare Organizations, 1997:xiii-- xviii.
Bartley J. Ventilation. In: Pfeiffer J, ed. APIC text of infection control and epidemiology. Washington, DC: Association for Professionals in
Infection Control and Epidemiology, Inc (APIC), 2000:77.1--77.11.
Bartley J. Construction and renovation. In: Pfeiffer J, ed. APIC text of infection control and epidemiology. Washington DC: Association
for Professionals in Infection Control and Epidemiology, Inc (APIC), 2000:72.1--77.11.
Harvey MA. Critical-care--unit bedside design and furnishing: impact on nosocomial infections. Infect Control Hosp Epidemiol 1998;19:597--601.
Infection Control Focus Group. Patient care focus groups 1998: assessing organizational readiness for infection control issues related to
construction, renovation, and physical plant projects. National Association of Children's Hospitals and Related Institutions.
Carter CD, Barr BA. Infection control issues in construction and renovation. Infect Control Hosp Epidemiol 1997;18:587--96.
Coronado VG, Beck-Sagué CM, Hutton MD, et al. Transmission of multidrug-resistant
Mycobacterium tuberculosis among persons with
human immunodeficiency virus infection in an urban hospital: epidemiologic and restriction fragment length polymorphism analysis. J Infect
Dis 1993;168:1052--5.
Coronado VG, Valway S, Finelli L, et al. Nosocomial transmission of multidrug-resistant
Mycobacterium tuberculosis among intravenous drug
users with human immunodeficiency virus infection [Abstract S50]. In: Abstracts of the Third Annual Meeting of the Society for Hospital Epidemiology
of America. Chicago, IL. Infect Control Hosp Epidemiol 1993;14:428.
Edlin BR, Tokars JI, Grieco MH, et al. An outbreak of multidrug-resistant tuberculosis among hospitalized patients with the
acquired immunodeficiency syndrome. N Engl J Med 1992;326:1514--21.
Fischl MA, Uttamchandani RB, Daikos GL, et al. An outbreak of tuberculosis caused by multiple-drug--resistant tubercle bacilli among patients
with HIV infection. Ann Intern Med 1992;117:177--83.
Ikeda RM, Birkhead GS, DeFerdinando Jr GT, et al. Nosocomial tuberculosis: an outbreak of a strain resistant to seven drugs. Infect Control
Hosp Epidemiol 1995;16:152--9.
Jarvis WR. Nosocomial transmission of multidrug-resistant
Mycobacterium tuberculosis. Res Microbiol 1992;144:117--22.
Jarvis WR. Nosocomial transmission of multidrug-resistant
Mycobacterium tuberculosis. Am J Infect Control 1995;23:146--51.
Jereb JA, Klevens RM, Privett TD, et al. Tuberculosis in health care workers at a hospital with an outbreak of multidrug-resistant
Mycobacterium tuberculosis. Arch Intern Med 1995;155:854--9.
Moran GJ, McCabe F, Morgan MT, Talan DA. Delayed recognition and infection control for tuberculosis patients in the emergency department.
Ann Emerg Med 1995;26:283--9.
Pearson ML, Jereb JA, Frieden TR, et al. Nosocomial transmission of multidrug-resistant
Mycobacterium tuberculosis: a risk to patients and health
care workers. Ann Intern Med 1992;117:191--6.
Ko G, Burge HA, Muilenberg M, Rudnick S, First M. Survival of mycobacteria on HEPA filter material. J Am Biol Safety Assoc 1998;3:65--78.
Gage AA, Dean DC, Schimert G, Minsley N.
Aspergillus infection after cardiac surgery. Arch Surg 1970;101:384--7.
Vargo JA, Ginsberg MM, Mizrahi M. Human infestation by the pigeon mite: a case report. Am J Infect Control 1983;11:24--5.
National Air Duct Cleaners Association. NADCA general specifications for the cleaning of commercial HVAC systems. Publication
#NAD--06. Washington, DC: National Air Duct Cleaners Association, 2002. Available at
http://www.nadca.com/standards/standards.asp.
US Environmental Protection Agency, Office of Pesticide Progams. Use of disinfectants and sanitizers in heating, ventilation, air conditioning,
and refrigeration systems [Letter]. March 14, 2002. Available at
http://www.epa.gov/oppad001/hvac.htm.
Rutala WA, Jones SM, Worthington JM, Reist PC, Weber DJ. Efficacy of portable filtration units in reducing aerosolized particles in the size range
of Mycobacterium tuberculosis. Infect Control Hosp Epidemiol 1995;16:391--8.
American Society of Heating, Refrigerating and Air-Conditioning Engineers, Inc. Ventilation for acceptable indoor air quality. Atlanta, GA,
1999; ASHRAE Standard 62-1999.
Garner JS, Hospital Infection Control Practices Advisory Committee. Guideline for isolation precautions in hospitals. Infect Control Hosp Epidemiol 1996;17:53--80.
Flynn PM, Williams BG, Hethrington SV, Williams BF, Giannini MA, Pearson TA.
Aspergillus terreus during hospital renovation [Letter].
Infect Control Hosp Epidemiol 1993;14:363--5.
Tabbara KF, Al Jabarti A. Hospital construction-associated outbreak of ocular aspergillosis after cataract surgery. Ophthalmology 1998;105:522--6.
Rhame FS, Streifel AJ, Kersey JH Jr, McGlave PB. Extrinsic risk factors for pneumonia in the patient at high risk of infection. Am J Med
1984;76:42--52.
Wells WF. Aerodynamics of droplet nuclei [Chapter 3]. In: Wells WF. Airborne contagion and air hygiene. Cambridge, MA: Harvard
University Press, 1955:13--9.
Gerson SL, Parker P, Jacobs MR, Creger R, Lazarus HM. Aspergillosis due to carpet contamination [Letter]. Infect Control Hosp
Epidemiol 1994;15:221--3.
Joint Commission on Accreditation of Healthcare Organizations. 2001 hospital accreditation standards. Oakbrook Terrace, IL: JCAHO
Press, 2001:193--220.
Fridkin SK, Kremer FB, Bland LA, Padhye A, McNeil MM, Jarvis WR.
Acremonium kiliense endophthalmitis that occurred after cataract extraction
in an ambulatory surgical center and was traced to an environmental reservoir. Clin Infect Dis 1996;22:222--7.
Streifel AJ. Maintenance and engineering. In: Pfeiffer J, ed. APIC text of infection control and epidemiology. Washington, DC: Association
for Professionals in Infection Control and Epidemiology, Inc., 2000:76.1--76.8.
Weems JJ Jr, Davis BJ, Tablan OC, Kaufman L, Martone WJ. Construction activity: an independent risk factor for invasive aspergillosis
and zygomycosis in patients with hematologic malignancy. Infect Control 1987;8:71--5.
Krasinski K, Holzman RS, Hanna B, Greco MA, Graff M, Bhogal M. Nosocomial fungal infection during hospital renovation. Infect
Control 1985;6:278--82.
Bartley JM. APIC state-of-the-art report: the role of infection control during construction in health care facilities. Am J Infect Control
2000;28:156--69.
Johnson MW, Mitch WE, Heller AH, Spector R. The impact of an educational program on gentamicin use in a teaching hospital. Am J
Med 1982;73:9--14.
Soumerai SB, Salem-Schatz S, Avorn J, Casteris CS, Ross-Degnan D, Popovsky MA. A controlled trial of educational outreach to improve
blood transfusion practice. JAMA 1993;270:961--6.
Eisenberg JM. An educational program to modify laboratory use by house staff. J Med Educ 1977;52:578--81.
Rello J, Quintana E, Ausina V, Puzo V, Puzo C, Net A, Prats G. Risk factors for
Staphylococcus aureus nosocomial pneumonia in critically ill
patients. Am Rev Respir Dis 1990;142:1320--4.
McWhinney PHM, Kibbler CC, Hamon MD, et al. Progress in the diagnosis and management of aspergillosis in bone marrow transplantation:
13 years' experience. Clin Infect Dis 1993;17:397--404.
Pannuti CS, Gingrich RD, Pfaller MA, Wenzel RP. Nosocomial pneumonia in adult patients undergoing bone marrow transplantation: a 9-year
study. J Clin Oncol 1991;9:77--84.
Wingard JR, Beals SU, Santos GW, Mertz WG, Saral
R. Aspergillus infections in bone marrow transplant recipients. Bone Marrow
Transplant 1987;2:175--81.
Gerson SL, Talbot GH, Hurwitz S, Strom BL, Lusk EJ, Cassileth PA. Prolonged granulocytopenia: the major risk factor for invasive
pulmonary aspergillosis in patients with acute leukemia. Ann Intern Med 1984;100:345--51.
Lentino JR, Rosenkranz MA, Michaels JA, Kurup VP, Rose HD, Rytel MW. Nosocomial aspergillosis: a retrospective review of airborne
disease secondary to road construction and contaminated air conditioners. Am J Epidemiol 1982;116:430--7.
Streifel AJ, Lauer JL, Vesley D, Juni B, Rhame FS.
Aspergillus fumigatus and other thermotolerant fungi generated by hospital building
demolition. Appl Environ Microbiol 1983;46:375--8.
Thio CL, Smith D, Merz WG, et al. Refinements of environmental assessment during an outbreak investigation of invasive aspergillosis in a
leukemia and bone marrow transplant unit. Infect Control Hosp Epidemiol 2000;21:18--23.
Mermel LA, Josephson SL, Giorgio CH, Dempsey J, Parenteau S. Association of Legionnaires' disease with construction: contamination of
potable water? Infect Control Hosp Epidemiol 1995;16:76--81.
Arnow PM, Anderson RL, Mainous PD, Smith EJ. Pulmonary aspergillosis during hospital renovation. Am Rev Respir Dis 1978;118:49--53.
Kuehn TH, Gacek B, Yang CH, et al. Identification of contaminants, exposures, effects, and control options for construction/renovation
activities (RP-804). ASHRAE Transactions: Research, 1995.
Opal SM, Asp AA, Cannady PB Jr, Morse PL, Burton LJ, Hammer PG II. Efficacy of infection control measures during a nosocomial outbreak
of disseminated aspergillosis associated with hospital construction. J Infect Dis 1986;153:634--7.
Association for Professionals in Infection Control and Epidemiology, Education Committee 1998--99. Infection control tool kit series ---
construction and renovation. Bartley J, ed. Washington DC: Association for Professionals in Infection Control and Epidemiology, 1999.
Ottney TC. Particle management for HVAC systems. ASHRAE J 1993;35:26--34.
Finkelstein LE, Mendelson MH. Infection control challenges during hospital renovation. Am J Nursing 1997;97:60--1.
Overberger PA, Wadowsky RM, Schaper MM. Evaluation of airborne particulates and fungi during hospital renovation. Am Ind Hyg Assoc
J 1995;56:706--12.
Streifel AJ, Marshall JW. Parameters for ventilation controlled environments in hospitals. In: Design, construction, and operation of healthy
buildings (IAQ/1997). Atlanta, GA: ASHRAE Press, 1998.
American Society of Heating, Refrigerating, and Air-Conditioning Engineers (ASHRAE). The HVAC commissioning process. ASHRAE Guideline
1-1996. Atlanta, GA: ASHRAE Press, 1996.
Morey R, Williams C. Porous insulation in buildings: a potential source of microorganisms. In: Proceedings of Indoor Air '90,
5th International Conference. Toronto, Canada: International Society of Indoor Air Quality and Climate, 1990.
Aisner J, Murillo J, Schimpff SC, Steere AC. Invasive aspergillosis in acute leukemia: correlation with nose cultures and antibiotic use. Ann
Intern Med 1979;90:4--9.
McCarty JM, Flam MS, Pullen G, Jones R, Kassel SH. Outbreak of primary cutaneous aspergillosis related to intravenous arm boards. J
Pediatr 1986;108(Pt.1):721--4.
Klimowski LL, Rotstein C, Cummings KM. Incidence of nosocomial aspergillosis in patients with leukemia over a twenty-year period. Infect
Control Hosp Epidemiol 1989;10:299--305.
Pfundstein J. Aspergillus infection among solid organ transplant recipients: a case study. J Transpl Coord 1997;7:187--9.
Rhame FS, Streifel A, Stevens P, et al. Endemic
Aspergillus airborne spore levels are a major risk factor for aspergillosis in bone marrow
transplant (BMT) patients [Abstract]. In: Program and abstracts of the
25th Interscience Conference on Antimicrobial Agents and Chemotherapy.
Minneapolis, MN: American Society for Microbiology, 1985.
Walmsley S, Devi S, King S, Schneider R, Richardson S, Ford-Jones L. Invasive
Aspergillus infections in a pediatric hospital: a ten-year review.
Pediatr Infect Dis J 1993;12:673--82.
Kyriakides GK, Zinneman HH, Hall WH, et al. Immunologic monitoring and aspergillosis in renal transplant patients. Am J Surg
1976;131:246--52.
Sherertz RJ, Belani A, Kramer BS, et al. Impact of air filtration on nosocomial
Aspergillus infections: unique risk of bone marrow transplant
recipients. Am J Med 1987;83:709--18.
Aisner J, Schimpff SC, Bennett JE, Young VM, Wiernik PH.
Aspergillus infections in cancer patients: association with fireproofing materials in a
new hospital. JAMA 1976;235:411--2.
Fox BC, Chamberlin L, Kulich P, Rae EJ, Webster LR. Heavy contamination of operating room air by
Penicillium species: identification of the
source and attempts at decontamination. Am J Infect Control 1990;18:300--6.
Barnes RA, Rogers TR. Control of an outbreak of nosocomial aspergillosis by laminar air-flow isolation. J Hosp Infect 1989;14:89--94.
Leenders A, VanBelkum A, Janssen S, et al. Molecular epidemiology of apparent outbreaks of invasive aspergillosis in a hematology ward. J
Clin Microbiol 1996;34:345--51.
Yeager CC. Copper and zinc preservatives [Chapter 21]. In: Block SS, ed. Disinfection, sterilization, and preservation.
4th ed. Philadelphia, PA: Lea and Febiger, 1991.
Allo MD, Miller J, Townsend T, Tan C. Primary cutaneous aspergillosis associated with Hickman intravenous catheters. N Engl J
Med 1987;317:1105--8.
Schleupner CJ, Hamilton JR. A pseudoepidemic of pulmonary fungal infections related to fiberoptic bronchoscopy. Infect Control 1980;1:38--42.
Denning DW, Clemons KV, Hanson LH, Stevens DA. Restriction endonuclease analysis of total cellular DNA of
Aspergillus fumigatus isolates of geographically and epidemiologically diverse origin. J Infect Dis 1990;162:1151--8.
James MJ, Lasker BA, McNeil MM, Shelton M, Warnock DW, Reiss E. Use of a repetitive DNA probe to type clinical and environmental isolates
of Aspergillus flavus from a cluster of cutaneous infections in a neonatal intensive care unit. J Clin Microbiol 2000;38:3612--8.
Skladny H, Buchheidt D, Baust C, et al. Specific detection of
Aspergillus species in blood and bronchoalveolar lavage samples
of immunocompromised patients by two-step PCR. J Clin Microbiol 1999;37:3865--71.
Symoens F, Bouchara JP, Heinemann S, Nolard N. Molecular typing of
Aspergillus terreus isolates by random amplification of polymorphic DNA.
J Hosp Infect 2000;44:273--80.
Diaz-Guerra TM, Mellado E, Cuenca-Estrella M, Gaztelurrutia L, Navarro JI, Tudela JL. Genetic similarity among one
Aspergillus flavus strain isolated from a patient who underwent heart surgery and two environmental strains obtained from the operating room. J Clin Microbiol 2000;38:2419--22.
Siegler L, Kennedy MJ. Aspergillus,
Fusarium, and other opportunistic moniliaceous fungi. In: Murray PR, Baron EJ, Pfaller MA, Tenover
FC, Yolken RH, eds. Manual of clinical microbiology.
7th ed. Washington, DC: American Society for Microbiology Press. 1999:1212--41.
Breton P, Germaud P, Morin O, Audouin AF, Milpied N, Harousseau JL. Unusual pulmonary mycoses in patients with hematologic disease
[French]. Rev Pneumol Clin 1998;54:253--7.
Guarro J, Nucci M, Akiti T, Gené J, Barreiro MD, Gonçalves RT. Fungemia due to
Fusarium sacchari in an immunosuppressed patient. J
Clin Microbiol 2000;38:419--21.
Burton JR, Zachery JB, Bessin R, et al. Aspergillosis in four renal transplant patients: diagnosis and effective treatment with amphotericin B.
Ann Intern Med 1972;77:383--8.
Buckner CD, Clift RA, Sanders JE, et al. Protective environment for marrow transplant recipients: a prospective study. Ann Intern Med
1978;89:893--901.
Murray WA, Streifel AJ, O'Dea TJ, Rhame FS. Ventilation for protection of immune compromised patients. ASHRAE Transactions
1988;94:1185--91.
Streifel AJ, Vesley D, Rhame FS, Murray B. Control of airborne fungal spores in a university hospital. Environment International 1989;15: 221--7.
Rhame FS. Endemic nosocomial filamentous fungal disease: a proposed structure for conceptualizing and studying the environmental hazard.
Infect Control 1986;7(suppl 2):124--5.
American Society of Heating, Refrigerating, and Air-Conditioning Engineers, Inc. 1999 ASHRAE handbook: heating, ventilating, and
air-conditioning applications. Health care facilities [Chapter 7]. Atlanta GA: American Society of Heating, Refrigerating, and
Air-Conditioning Engineers, Inc., 1999.
Mahoney DH Jr, Steuber CP, Starling KA, Barrett FF, Goldberg J, Fernbach DJ. An outbreak of aspergillosis in children with acute leukemia.
J Pediatr 1979;95:70--2.
Ehrenkranz NJ, Kicklighter JL. Tuberculosis outbreak in a general hospital: evidence for airborne spread of infection. Ann Intern Med
1972;77:377--82.
Calder RA, Duclos P, Wilder MH, Pryor VL, Scheel, WJ.
Mycobacterium tuberculosis transmission in a health clinic. Bull Int Union Tuberc Lung
Dis 1991;66:103--6.
Jereb JA, Burwen DR, Dooley SW, et al. Nosocomial outbreak of tuberculosis in a renal transplant unit: application of a new technique for
restriction fragment length polymorphism analysis of
Mycobacterium tuberculosis isolates. J Infect Dis 1993;168:1219--24.
Monath TP. Yellow fever: Victor, Victoria? Conqueror, conquest? Epidemics and research in the last forty years and prospects for the future. Am
J Trop Med Hyg 1991;45:1--43.
Weber DJ, Rutala WA. Risks and prevention of nosocomial transmission of rare zoonotic diseases. Clin Infect Dis 2001;32:446--56.
Gerberding JL. Nosocomial transmission of opportunistic infections. Infect Control Hosp Epidemiol 1998;19:574--7.
Vargas SL, Ponce CA, Gigliotti F, et al. Transmission of
Pneumocystis carinii DNA from a patient with
P. carinii pneumonia to immunocompetent contact health care workers. J Clin Microbiol 2000;38:1536--8.
Walzer PD. Pneumocystis carinii
[Chapter 260]. In: Mandell GL, Bennett JE, Dolin R., eds. Principles and practice of infectious diseases.
5th ed. Philadelphia, PA: Churchill Livingstone, 2000:2781--95.
Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR, Hospital Infection Control Practices Advisory Committee. Guideline for prevention
of surgical site infection, 1999. Infect Control Hosp Epidemiol 1999;20:247--80.
Lidwell OM. Clean air at operation and subsequent sepsis in the joint. Clin Orthop 1986;211:91--102.
Nichols RL. The operating room [Chapter 22]. In: Bennett JV, Brachman PS, eds. Hospital infections.
3rd ed. Boston, MA: Little, Brown and Company, 1992:461--73.
Clark RP, Reed PJ, Seal DV, Stephenson ML. Ventilation conditions and air-borne bacteria and particles in operating theatres: proposed
safe economies. J Hyg (Lond) 1985;95:325--35.
Babb JR, Lynam P, Ayliffe GAJ. Risk of airborne transmission in an operating theater containing four ultraclean air units. J Hosp Infect
1995;31:159--68.
Laufman H. The operating room [Chapter 20]. In: Bennett JV, Brachman PS, eds. Hospital Infections.
2nd ed. Boston, MA: Little, Brown and Company,1986:315--23.
Ad Hoc Committee of the Committee on Trauma, Division of Medical Sciences, National Academy of Sciences --- National Research
Council. Postoperative wound infections: the influence of ultraviolet irradiation of the operating room and of various other factors. Ann Surg 1964;160(suppl):1--192.
Charnley J. A clean-air operating enclosure. Br J Surg 1964;51:202--5.
Lidwell OM, Lowbury EJ, Whyte W, Blowers R, Stanley SJ, Lowe D. Effect of ultraclean air in operating rooms on deep sepsis in the joint after
total hip or knee replacement: a randomised study. Br Med J 1982;285:10--4.
Hill C, Flamant R, Mazas F, Evrard J. Prophylactic cefazolin versus placebo in total hip replacement: report of a multicentre double-blind
randomised trial. Lancet 1981;1:795--6.
Ha'eri GB, Wiley AM. Total hip replacement in a laminar flow environment with special reference to deep infections. Clin Orthop 1980;148:163--8.
Collins DK, Steinhaus K. Total hip replacement without deep infection in a standard operating room. J Bone Joint Surg Am 1976;58:446--50.
Taylor GJ, Bannister GC, Leeming JP. Wound disinfection with ultraviolet radiation. J Hosp Infect 1995;30:85--93.
Ayliffe GA. Role of the environment of the operating suite in surgical wound infection. Rev Infect Dis 1991;13(suppl 10):S800--4.
Choux M, Genitori L, Lang D, Lena G. Shunt implantation: reducing the incidence of shunt infection. J Neurosurg 1992;77:875--80.
Occupational Safety and Health Administration. 29 CFR 1910.139. Respiratory Protection. Federal Register 1998;63:1152--300.
Langevin PB, Rand KH, Layton AJ. The potential for dissemination of
Mycobacterium tuberculosis through the anesthesia breathing circuit.
Chest 1999;115:1107--14.
Occupational Safety and Health Administration. 29 CFR 1910. Occupational exposure to tuberculosis proposed rule. Federal
Register 1997;62:54159--209.
Aranha-Creado H, Prince D, Greene K, Brandwein H. Removal of
Mycobacterium species by breathing circuit filters. Infect Control Hosp
Epidemiol 1997;18:252--4.
Burroughs HE. Sick building syndrome: fact, fiction, or facility? In: Hansen W., ed. A guide to managing indoor air quality in health
care organizations. Oakbrook Terrace, IL: Joint Commission on Accreditation of Health Care Organizations, 1997:3--13.
Anderson K, Morris G, Kennedy H, et al. Aspergillosis in immunocompromised paediatric patients: associations with building hygiene, design,
and indoor air. Thorax 1996;51:256--61.
National Institute for Occupational Safety and Health. Control of smoke from laser/electric surgical procedures, 1996; DHHS publication
no. (NIOSH) 96--128. Available at http://www.cdc.gov/niosh/hc11.html.
Association of Perioperative Registered Nurses. Recommended practices for laser safety in practice settings. AORN J 1998;67:263--4, 267--9.
Hughes PS, Hughes AP. Absence of human papillomavirus DNA in the plume of erbium: YAG laser-treated warts. J Am Acad
Dermatol 1998;38:426--8.
Capizzi PJ, Clay RP, Battey MJ. Microbiologic activity in laser resurfacing plume and debris. Lasers Surg Med 1998;23:172--4.
Emergency Care Research Institute (ECRI). Surgical smoke evacuation systems. Health Devices 1997;26:132--72.
ECRI. Update evaluation: surgical smoke evacuation systems. Health Devices 1999;28:333--62.
ECRI. Stationary surgical smoke evacuation systems. Health Devices 2001;30:73--86.
Villarino ME, Stevens LE, Schable B, et al. Risk factors for epidemic
Xanthomonas maltophilia infection/colonization in intensive care unit
patients. Infect Control Hosp Epidemiol 1992;13:201--6.
Seifert H, Strate A, Pulverer G. Nosocomial bacteremia due to
Acinetobacter baumannii: clinical features, epidemiology, and predictors of
mortality. Medicine (Baltimore) 1995;74:340--9.
Yu VL. Serratia marcescens: historical perspective and clinical review. N Engl J Med 1979;300:887--93.
Go ES, Urban C, Burns J, et al. Clinical and molecular epidemiology of
Acinetobacter infections sensitive only to polymyxin B and sulbactam.
Lancet 1994;344:1329--32.
Boyce JM, Pittet D. Guideline for hand hygiene in health-care settings: recommendations of the Healthcare Infection Control Practices
Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Infect Control Hosp Epidemiol 2002;23 (suppl):S3--40.
Burdge DR, Nakielna EM, Noble MA. Case-control and vector studies of nosocomial acquisition of
Pseudomonas cepacia in adult patients with
cystic fibrosis. Infect Control Hosp Epidemiol 1993;14:127--30.
Cox R, deBorja K, Bach MC. A pseudo-outbreak of
Mycobacterium chelonae infections related to bronchoscopy. Infect Control Hosp
Epidemiol 1997;18:136--7.
Hoy J, Rolston K, Hopfer RL. Pseudoepidemic of
Mycobacterium fortuitum in bone marrow cultures. Am J Infect Control 1987;15:268--71.
Stine TM, Harris AA, Levin S, Rivera N, Kaplan, RL. A pseudoepidemic due to atypical mycobacteria in a hospital water supply.
JAMA 1987;258:809--11.
Bennett SN, Peterson DE, Johnson DR, Hall WN, Robinson-Dunn B, Dietrich S. Bronchoscopy-associated
Mycobacterium xenopi pseudoinfections. Am J Respir Crit Care Med 1994;150:245--50.
Hlady WG, Mullen RC, Mintz CS, Shelton BG, Hopkins RS, Daikos GL. Outbreak of Legionnaire's disease linked to a decorative fountain
by molecular epidemiology. Am J Epidemiol 1993;138:555--62.
American Society of Heating, Refrigerating, and Air-Conditioning Engineers, Inc.. ASHRAE guideline 12--2000: minimizing the risk of
legionellosis associated with building water systems. Atlanta, GA: ASHRAE, Inc., 2000:1--6.
Snyder MB, Siwicki M, Wireman J, et al. Reduction of
Legionella pneumophila through heat flushing followed by continuous supplemental
chlorination of hospital hot water. J Infect Dis 1990;162:127--32.
Ezzeddine H, Van Ossel C, Delmée M, Wauters G.
Legionella spp. in a hospital hot water system: effect of control measures. J Hosp
Infect 1989;13:121--31.
Joint Commission on Accreditation of Healthcare Organizations. Comprehensive accreditation manual for hospitals: the official handbook.
Oakbrook Terrace, IL: JCAHO Press, 2000.
Juranek DD, Addiss DG, Bartlett ME, et al. Crytosporidiosis and public health: workshop report. Journal of the American Water Works
Association 1995;87:69--80.
Tokars JI, Miller ER, Alter MJ, Arduino MJ. National surveillance of dialysis-associated diseases in the United States, 1997. Semin Dial
2000;13:75-85.
Vujanovic V, Smoragiewicz W, Krzysztyniak K. Airborne fungal ecological niche determination as one of the possibilities for indirect
mycotoxin risk assessment in indoor air. Environ Toxicol 2001;16:1--8.
Vesper S, Dearborn DG, Yike I, et al. Evaluation of
Stachybotrys chartarum in the house of an infant with pulmonary hemorrhage: quantitative assessment before, during, and after remediation. J Urban Health 2000;77:68--85.
Best M, Yu VL, Stout J, Goetz A, Muder RR, Taylor F. Legionellaceae in the hospital water-supply: epidemiologic link with disease and evaluation
of a method for control of nosocomial Legionnaires' disease and Pittsburgh pneumonia. Lancet 1983;2:307--10.
Meenhorst PL, Reingold AL, Groothuis DG, et al. Water-related nosocomial pneumonia caused by
Legionella pneumophila serogroups 1 and 10.
J Infect Dis 1985;152:356--64.
Johnston JM, Latham RH, Meier FA, et al. Nosocomial outbreak of Legionnaires' disease: molecular epidemiology and disease control
measures. Infect Control 1987;8:53--8.
Muraca PW, Yu VL, Goetz A. Disinfection of water distribution systems for
Legionella: a review of application procedures and methodologies.
Infect Control Hosp Epidemiol 1990;11:79--88.
Johnson JT, Yu VL, Best MG, et al. Nosocomial legionellosis in surgical patients with head and neck cancer: implications for epidemiological
reservoir and mode of transmission. Lancet 1985;2:298--300.
Marrie TJ, MacDonald S, Clarke K, Haldane D. Nosocomial legionnaires' disease: lessons from a four-year prospective study. Am J Infect
Control 1991;19:79--85.
Marrie TJ, Haldane D, Bezanson G, Peppard R. Each water outlet is a unique ecological niche for Legionella pneumophila. Epidemiol
Infect 1992;108:261--70.
Department of Health and Social Security and the Welsh Office. The control of
Legionellae in health care premises: a code of practice. London:
Her Majesty's Stationery Office, 1991.
Helms CM, Massanari RM, Wenzel RP, et al. Legionnaires' disease associated with a hospital water system: a five-year progress report on
continuous hyperchlorination. JAMA 1988;259:2423--7.
Edelstein PH, Whittaker RE, Kreiling RL, Howell, CL. Efficacy of ozone in eradication of
Legionella pneumophila from hospital plumbing
fixtures. Appl Environ Microbiol 1982;44:1330--4.
Muraca P, Stout JE, Yu VL. Comparative assessment of chlorine, heat, ozone, and UV light for killing
Legionella pneumophila within a model plumbing system. Appl Environ Microbiol 1987;53:447--53.
Domingue EL, Tyndall RL, Mayberry WR, Pancorbo OC. Effects of three oxidizing biocides on
Legionella pneumophila serogroup 1. Appl
Environ Microbiol 1988;54:741--7.
Landeen LK, Yahya MT, Gerba CP. Efficacy of copper and silver ions and reduced levels of free chlorine in inactivation of
Legionella pneumophila. Appl Environ Microbiol 1989;55:3045--50.
Matulonis U, Rosenfeld CS, Shadduck RK. Prevention of
Legionella infections in bone marrow transplant unit: multifaceted approach to decontamination of a water system. Infect Control Hosp Epidemiol 1993;14:571--5.
Liu Z, Stout JE, Tedesco L, et al. Controlled evaluation of copper-silver ionization in eradicating
Legionella pneumophila from a hospital
water distribution system. J Infect Dis 1994;169:919--22.
Margolin AB. Control of microorganisms in source water and drinking water [Chapter 20]. In: Hurst CJ, Knudsen GR, McInerney MJ,
Stetzenback LD, Walter MV, eds. Manual of environmental microbiology. Washington, DC: American Society for Microbiology Press, 1997:195--202.
Freije MR. Legionella control in health care facilities: a guide for minimizing risk. Indianapolis,
In: HC Information Resources, Inc., 1996:65--75.
Lin YE, Vidic RD, Stout JE, Yu VL.
Legionella in water distribution systems: regular culturing of distribution system samples is the key to successful disinfection. Journal of the American Water Works Association 1998;90:112--21.
Biurrun A, Caballero L, Pelaz C, León E, Gago A. Treatment of a
Legionella pneumophila- colonized water distribution system using
copper-silver ionization and continuous chlorination. Infect Control Hosp Epidemiol 1999;20:426--8.
Goetz A, Yu VL. Copper-silver ionization: Cautious optimism for
Legionella disinfection and implications for environmental culturing. Am J
Infect Control 1997;25:449--451.
Stout JE, Lin EY, Goetz AM, Muder RR. Controlling
Legionella in hospital water systems: experience with the superheat-and-flush method and copper-silver ionization. Infect Control Hosp Epidemiol 1998;19:911--4.
Walker JT, Mackerness CW, Mallon D, Makin T, Williets T, Keevil CW. Control of
Legionella pneumophila in a hospital water system by
chlorine dioxide. J Ind Microbiol 1995;15:384--90.
Hambidge A. Reviewing efficacy of alternative water treatment techniques. Health Estate Journal 2001;55:23--5.
Rohr U, Senger M, Selenka F, Turley R, Wilhelm M. Four years of experience with silver-copper ionization for control of
Legionella in a German university hospital hot water plumbing system. Clin Infect Dis 1999;29:1507--11.
Cunliffe DA. Inactivation of Legionella
pneumophila by monochloramine. J Appl Bacteriol 1990;68:453--9.
Kirmeyer GJ, Foust GW, Pierson GL, Simmler JJ, LeChevalier MW. Optimizing chloramine treatment. Denver, CO; American Water
Works Research Foundation, 1993.
Kool JL, Carpenter JC, Fields BS. Effect of monochloramine disinfection of municipal drinking water on risk of nosocomial Legionnaires'
disease. Lancet 1999;353:272--7.
Kool JL, Bergmire-Sweat D, Butler JC, et al. Hospital characteristics associated with colonization of water systems by
Legionella and risk of nosocomial Legionnaires' disease: a cohort study of 15 hospitals. Infect Control Hosp Epidemiol 1999;20:798--805.
Kool JL, Fiore AE, Kioski CM, et al. More than 10 years of unrecognized nosocomial transmission of Legionnaires' disease among transplant
patients. Infect Control Hosp Epidemiol 1998;19:898--904.
Le Saux NM, Sekla L, McLeod J, et al. Epidemic of nosocomial Legionnaires' disease in renal transplant recipients: a case-control and
environmental study. CMAJ 1989;140:1047--53.
Kugler JW, Armitage JO, Helms CM, et al. Nosocomial Legionnaires' disease: occurrence in recipients of bone marrow transplants. Am J
Med 1983;74:281--8.
Marston BJ, Lipman HB, Breiman RF. Surveillance for Legionnaires' disease: risk factors for morbidity and
mortality. Arch Intern Med 1994;154:2417--22.
Haley CE, Cohen ML, Halter J, Meyer RD. Nosocomial Legionnaires' disease: a continuing common-source epidemic at Wadsworth Medical
Center. Ann Intern Med 1979;90:583--6.
Jimènez ML, Aspa J, Padilla B, et al. Fiberoptic bronchoscopic diagnosis of pulmonary disease in 151 HIV-infected patients with pneumonitis. Eur
J Clin Microbiol Infect Dis 1991; 10:491--7.
Bock BV, Kirby BD, Edelstein PH, et al. Legionnaires' disease in renal-transplant recipients. Lancet 1978;1:410--3.
Kirby BD, Snyder KM, Meyer RD, Finegold SM. Legionnaires' disease: report of sixty-five nosocomially acquired cases and review of the
literature. Medicine (Baltimore) 1980;59:188--205.
Brady MT. Nosocomial legionnaires disease in a children's hospital. J Pediatr 1989;115:46--50.
Muder RR, Yu VL, McClure JK, Kroboth FJ, Kominos SD, Lumish RM. Nosocomial Legionnaires' disease uncovered in a prospective
pneumonia study: implications for underdiagnosis. JAMA 1983;249:3184--8.
Garbe PL, Davis BJ, Weisfeld JS, et al. Nosocomial Legionnaires' disease: epidemiologic demonstration of cooling towers as a source.
JAMA 1985;254:521--4.
Hanrahan JP, Morse DL, Scharf VB, et al. A community hospital outbreak of legionellosis: transmission by potable hot water. Am J
Epidemiol 1987;125:639--49.
Arnow PM, Chou T, Weil D, Shapiro EN, Kretzschmar C. Nosocomial Legionnaires' disease caused by aerosolized tap water from respiratory
devices. J Infect Dis 1982;146:460--7.
Mastro TD, Fields BS, Breiman RF, Campbell J, Plikaytis BD, Spika JS. Nosocomial Legionnaires' disease and use of medication nebulizers. J
Infect Dis 1991;163:667--70.
Dondero TJ Jr, Rendtorff RC, Mallison GF, et al. An outbreak of Legionnaires' disease associated with a contaminated air-conditioning cooling
tower. N Engl J Med 1980;302:365--70.
O'Mahony MC, Stanwell-Smith RE, Tillett HE, et al. The Stafford outbreak of Legionnaires' disease. Epidemiol Infect 1990;104:361--80.
Breiman RF, Fields BS, Sanden G, Volmer L, Meier A, Spika JS. Association of shower use with Legionnaires' disease: possible role of amoebae.
JAMA 1990;263:2924--6.
Breiman RF, VanLoock FL, Sion JP, et al. Association of "sink bathing" and Legionnaires' disease [Abstract]. In: Program and abstracts of the
91st General Meeting of the American Society for Microbiology. Dallas, TX: American Society for Microbiology, 1991.
Struelens MJ, Maes N, Rost F, et al. Genotypic and phenotypic methods for the investigation of a nosocomial
Legionella pneumophila outbreak and efficacy of control measures. J Infect Dis 1992;166:22--30.
Barbaree JM, Gorman GW, Martin WT, Fields BS, Morrill WE. Protocol for sampling environmental sites for Legionellae. Appl Environ
Microbiol 1987;53:1454--8.
Schoonmaker D, Heimberger T, Birkhead G. Comparison of ribotyping and restriction enzyme analysis using pulsed-field gel electrophoresis
for distinguishing Legionella pneumophila isolates obtained during a nosocomial outbreak. J Clin Microbiol 1992;30:1491--8.
Knirsch CA, Jakob K, Schoonmaker D, et al. An outbreak of
Legionella micdadei pneumonia in transplant patients: evaluation, molecular epidemiology, and control. Am J Med 2000;108:290--5.
Alary M, Joly JR. Factors contributing to the contamination of hospital water distribution systems by Legionellae. J Infect Dis 1992;165:565--9.
Yu VL, Beam TR Jr, Lumish RM, et al. Routine culturing for
Legionella in the hospital environment may be a good idea: A three-hospital
prospective study. Am J Med Sci 1987;294:97--9.
Tobin JO, Swann RA, Bartlett CL. Isolation of
Legionella pneumophila from water systems: Methods and preliminary results. Br Med J
1981;282:515--7.
Chow JW, Yu VL. Legionella: a major opportunistic pathogen in transplant recipients. Semin Respir Infect 1998;13:132--9.
Mandel AS, Sprauer MA, Sniadack DH, Ostroff SM. State regulation of hospital water temperature. Infect Control Hosp Epidemiol 1993;14:642--5.
Hirani NA, Macfarlane JT. Impact of management guidelines on the outcome of severe community acquired pneumonia. Thorax 1997;52:17--21.
Patterson WJ, Hay J, Seal DV, McLuckie JC. Colonization of
transplant unit water supplies with Legionella and protozoa: precautions required
to reduce the risk of legionellosis. J Hosp Infect 1997;37:7--17.
Marrie TJ, Haldane D, MacDonald S, et al. Control of endemic nosocomial Legionnaires' disease by using sterile potable water for high risk
patients. Epidemiol Infect 1991;107:591--605.
Zuravleff JJ, Yu VL, Shonnard JW, Rihs JD, Best M.
Legionella pneumophila contamination of a hospital humidifier: demonstration of
aerosol transmission and subsequent subclinical infection in exposed guinea pigs. Am Rev Respir Dis 1983;128:657--61.
World Health Organization, Regional Office for Europe. Environmental aspects of the control of legionellosis [German]. Schriftenr Ver
Wasser Boden Lufthyg 1993;91:249--52.
Bhopal RS, Barr G. Maintenance of cooling towers following two outbreaks of Legionnaires' disease in a city. Epidemiol Infect 1990;104:29--38.
World Health Organization. Epidemiology, prevention, and control of legionellosis: memorandum from a WHO meeting. Bull World Health
Organ 1990;68:155--64.
Bolan G, Reingold AL, Carson LA, et al. Infections with
Mycobacterium chelonae in patients receiving dialysis and using processed hemodialyzers.
J Infect Dis 1985;152:1013--9.
Lowry PW, Beck-Saguè CM, Bland LA, et al.
Mycobacterium chelonae infection among patients receiving high-flux dialysis in a hemodialysis clinic
in California. J Infect Dis 1990;161:85--90.
Favero MS, Petersen NJ, Boyer KM, Carson LA, Bond WW. Microbial contamination of renal dialysis systems and associated health risks. Trans
Am Soc Artif Intern Organs 1974;20:175--83.
Favero MS, Petersen NJ, Carson LA, Bond WW, Hindman SH. Gram-negative water bacteria in hemodialysis systems. Health Lab Sci
1975;12:321--34.
Association for the Advancement of Medical Instrumentation and American National Standards Institute. Hemodialysis systems. ANSI/AAMI
RD5-1992. Arlington, VA: 1993.
Association for the Advancement of Medical Instrumentation, American National Standards Institute. Reuse of hemodialyzers. ANSI/AAMI
RD47-1993. Arlington, VA: 1993.
Petersen NJ, Boyer KM, Carson LA, Favero MS. Pyrogenic reactions from inadequate disinfection of a dialysis fluid distribution system.
Dialysis Transpl 1978;7:52--7.
Dawids SG, Vejlsgaard R. Bacteriological and clinical evaluation of different dialysate delivery systems. Acta Med Scand 1976;199:151--5.
Kidd EE. Bacterial contamination of dialyzing fluid of artificial kidney. Br Med J 1964;1:880--2.
Klein E, Pass T, Harding GB, Wright R, Million C. Microbial and endotoxin contamination in water and dialysate in the central United States.
Artif Organs 1990;14:85--94.
Man NK, Degremont A, Darbord JC, Collet M, Vaillant P. Evidence of bacterial biofilm in tubing from hydraulic pathway of hemodialysis
system. Artif Organs 1998;22:596--600.
Association for the Advancement of Medical Instrumentation. Water treatment equipment for hemodialysis applications. ANSI/AAMI
RD62--2001. American National Standards Institute, Inc. Arlington, VA: 2001.
Bland LA. Microbiological and endotoxin assays of hemodialysis fluids. Adv Renal Replace Ther 1995;2:70--9.
Arduino MJ, Bland LA, Aguero SM, Carson LA, Ridgeway M, Favero MS. Comparison of microbiologic assay methods for hemodialysis fluids.
J Clin Microbiol 1991;29:592--4.
Bland LA, Ridgeway MR, Aguero SM, Carson LA, Favero MS. Potential bacteriologic and endotoxin hazards associated with liquid
bicarbonate concentrate. ASAIO Trans 1987;33:542--5.
Raij L, Shapiro FL, Michael AF. Endotoxemia in febrile reactions during hemodialysis. Kidney Int 1973;4:57--60.
Bommer J, Becker KP, Urbaschek R. Potential transfer of endotoxin across high-flux polysulfone membranes. J Am Soc Nephrol 1996;7:883--8.
Arduino MJ, Favero MS. Microbiologic aspects of hemodialysis. Arlington, VA: Association for the Advancement of Medical Instrumentation,
1998. AAMI monograph WQD--1998.
Koepke GH, Christopher RP. Contamination of whirlpool baths during treatment of infected wounds. Arch Phys Med Rehabil 1965;46:261--3.
CDC. Epidemiologic notes and reports: outbreak of viral gastroenteritis --- Pennsylvania and Delaware. MMWR 1987;36:709--11.
Crow HE, Corpe RF, Smith CE. Is serious pulmonary disease caused by nonphotochromogenic ("atypical") acid-fast mycobacteria
communicable? Dis Chest 1961;39:372--81.
Stout JE, Yu VL, Muraca P. Isolation of
Legionella pneumophila from the cold water of hospital ice machines: implications for origin and
transmission of the organism. Infect Control 1985;6:141--6.
Manangan LP, Anderson RL, Arduino MJ, Bond WW. Sanitary care and maintenance of ice-storage chests and ice-making machines in health
care facilities. Am J Infect Control 1998;26:111--2.
Cannon RO, Poliner JR, Hirschhorn RB, et al. A multistate outbreak of Norwalk virus gastroenteritis associated with consumption of commercial
ice. J Infect Dis 1991;164:860--3.
Khan AS, Moe CL, Glass RI, et al. Norwalk virus-associated gastroenteritis traced to ice consumption aboard a cruise ship in Hawaii: comparison
and application of molecular method-based assays. J Clin Microbiol 1994;32:318--22.
Schmidt OW, Cooney MK, Foy HM. Adeno-associated virus in adenovirus type 3 conjunctivitis. Infect Immun 1975;11:1362--70.
McCandlish R, Renfrew M. Immersion in water during labor and birth: the need for evaluation. Birth 1993;20:79--85.
White CG. Chemistry of chlorination [Chapter 4]. In: Handbook of Chlorination and Alternative Disinfectants.
3rd ed. New York, NY: Van Nostrand Reinhold, 1992:184--249.
Muscarella LF. Automatic flexible endoscope reprocessors. Gastrointest Endosc Clin N Am 2000;10:245--57.
Muscarella LF. Anticipated reliability of liquid chemical sterilants [Letter]. Am J Infect Control 1998;26:155--6.
Muscarella LF. Déjà vu . . . all over again? The importance of instrument drying [Letter]. Infect Control Hosp Epidemiol 2000;21:628--9.
Gubler JG, Salfinger M, von Graevenitz A. Pseudoepidemic of nontuberculous mycobacteria due to a contaminated bronchoscope cleaning
machine: report of an outbreak and review of the literature. Chest 1992;101:1245--9.
Fraser VJ, Jones M, Murray PR, Medoff G, Zhang Y, Wallace RJ Jr. Contamination of flexible fiberoptic bronchoscopes with
Mycobacterium chelonae linked to an automated bronchoscope disinfection machine. Am Rev Respir Dis 1992;145:853--5.
Muscarella LF. Application of environmental sampling to flexible endoscope reprocessing: the importance of monitoring the rinse water.
Infect Control Hosp Epidemiol 2002; 23:285--9.
Cooke RP, Whymant-Morris A, Umasankar RS, Goddard SV. Bacteria-free water for automatic washer-disinfectors: an impossible dream? J
Hosp Infect 1998;39:63--5.
Allen JJ, Allen MO, Olsen MM, et al.
Pseudomonas infection of the biliary system resulting from the use of a contaminated
endoscope. Gastroenterology 1987;92:759--63.
Michele TM, Cronin WA, Graham NM, et al. Transmission
of Mycobacterium tuberculosis by a fiberoptic bronchoscope: identification by
DNA fingerprinting. JAMA 1997;278:1093--95.
US Food and Drug Administration, CDC. Public health advisory: infections from endoscopes inadequately reprocessed by an automated
endoscope reprocessing system. September 10, 1999. Available at
http://www.fda.gov/cdrh/safety/endoreprocess.pdf.
Alvarado CJ, Reichelderfer M. APIC guideline for infection prevention and control in flexible endoscopy. Am J Infect Control 2000;28:138--55.
CDC. Statement from CDC regarding biofilm and dental unit water quality. Atlanta GA: US Department of Health and Human Services,
Public Health Service, CDC, 1999.
Office of Safety and Asepsis Procedures Research Foundation. Dental unit waterlines. OSAP position paper. Annapolis, MD: 2000. Available at
http://www.osap.org/issues/pages/water/duwl.htm.
US Environmental Protection Agency. National Primary Drinking Water Regulations, 1999. 40 CFR 1, Part 141, Subpart G. Available at
http://www.epa.gov/safewater/mcl.html.
Bagga BS, Murphy RA, Anderson AW, Punwani I. Contamination of dental unit cooling water with oral microorganisms and its prevention.
JADA 1984;109:712--6.
Shearer BG. Biofilm and the dental office. JADA 1996;127:181--9.
Garner JS, Favero MS. CDC guideline for handwashing and hospital environmental control. Infect Control 1986;7:231--43.
Mallison GF. Hospital disinfectants for housekeeping: floors and tables. Infect Control 1984;5:537.
Favero MS, Bond WW. Chemical disinfection of medical and surgical materials [Chapter 43]. In: Block SS, ed. Disinfection, sterilization,
and preservation. 5th ed. Philadelphia, PA: Lippincott Williams and Wilkins, 2001.
Rutala WA. APIC guideline for selection and use of disinfectants. Am J Infect Control 1996;24:313--42.
Stingeni L, Lapomarda V, Lisi P. Occupational hand dermatitis in hospital environments. Contact Dermatitis 1995;33:172--6.
Busch A, Werner E. Animal tolerance to peracetic acid: experimental
results following the application of peracetic acid solutions on the skin of
pigs [German]. Monatshefte für Veterinaermedizin 1974;29:494--8.
US Food and Drug Administration. Medical devices: adequate directions for use. [21 CFR Part 801.5, 807.87.e].
Favero MS, Bond WW. Sterilization, disinfection, and antisepsis in
the hospital [Chapter 24]. In: Balows A, Hausler WJ Jr, Herrmann KL, Isenberg
HD, Shadomy HJ, eds. Manual of clinical microbiology.
5th ed.Washington, DC: American Society for Microbiology, 1991:183--200.
Chou T. Environmental Services. In: Pfeiffer J, ed. APIC text of infection control and epidemiology. Washington, DC: Association for Professionals
in Infection Control and Epidemiology, Inc., 2000;73.1--.8.
Rutala WA, Weber DJ. Cleaning, disinfection, and sterilization. In: Pfeiffer J, ed. APIC Text of Infection Control and Epidemiology.
Washington, DC: Association for Professionals in Infection Control and Epidemiology, Inc., 2000;55.1--.6.
Ayliffe GA, Collins BJ, Lowbury EJ, Babb JR, Lilly HA. Ward floors and other surfaces as reservoirs of hospital infection. J Hyg (Lond)
1967;65:515--37.
Dancer SJ. Mopping up hospital infection. J Hosp Infect 1999;43:85--100.
Schmidt EA, Coleman DL, Mallison GF. Improved system for floor cleaning in health care facilities. Appl Environ Microbiol 1984;47:942--6.
Mallison GF. Decontamination, disinfection, and sterilization. Nurs Clin North Am 1980;15:757--67.
Walter CW, Kundsin RB. The floor as a reservoir of hospital infections. Surg Gynec Obstet 1960;111:412--22.
Scott E, Bloomfield SF. The survival and transfer of microbial contamination via cloths, hands and utensils. J Appl Bacteriol 1990;68:271--8.
Scott E, Bloomfield SF. Investigations of the effectiveness of detergent washing, drying and chemical disinfection on contamination of cleaning
cloths. J Appl Bacteriol 1990;68:279--83.
Brown DG, Schatzle K, Gable T. The hospital vacuum cleaner: mechanism for redistributing microbial contaminants. J Environ Health
1980;42:192--6.
Wysowski DK, Flynt JW, Goldfield M, Altman R, Davis AT. Epidemic neonatal hyperbilirubinemia and use of a phenolic disinfectant
detergent. Pediatrics 1978;61:165--70.
Doan HM, Keith L, Shennan AT. Phenol and neonatal jaundice. Pediatrics 1979;64:324--5.
American Academy of Pediatrics, American College of Obstetricians and Gynecologists. Infection control. In: Guidelines for perinatal care.
4th ed. Washington, DC: 1997:269--74.
US Department of Labor, Occupational Safety and Health Administration: 29 CFR 1910.1030. Occupational exposure to bloodborne
pathogens; final rule. Federal Register 1991;56:64004--182.
Spire B, Montagnier L, Barré-Sinoussi F, Chermann JC. Inactivation of lymphadenopathy associated virus by chemical disinfectants.
Lancet 1984;2:899--901.
Martin LS, McDougal JS, Loskoski SL. Disinfection and inactivation of the human T lymphotrophic virus
type-III/lymphadenopathy-associated virus. J Infect Dis 1985;152:400--3.
Hanson PJ, Gor D, Jeffries DJ, Collins JV. Chemical inactivation of HIV on surfaces. Br Med J 1989;298:862--4.
Bloomfield SF, Smith-Burchnell CA, Dalgleish AG. Evaluation of hypochlorite-releasing disinfectants against the human immunodeficiency
virus (HIV). J Hosp Infect 1990;15:273--8.
Druce JD, Jardine D, Locarnini SA, Birch CJ. Susceptibility of HIV to inactivation by disinfectants and ultraviolet light. J Hosp Infect
1995;30:167--80.
Van Bueren J, Simpson RA, Salman H, Farrelly HD, Cookson BD. Inactivation of HIV--1 by chemical disinfectants: sodium hypochlorite.
Epidemiol Infect 1995;115:567--79.
Prince DL, Prince HN, Thraehart O, et al. Methodological approaches to disinfection of human hepatitis B viruses. J Clin Microbiol
1993;31:3296--3304.
CDC. Recommendations for prevention of HIV transmission in health-care settings. MMWR 1987;36(Suppl No. 2S).
Sattar SA, Springthorpe VS. Survival and disinfectant inactivation of the human immunodeficiency virus: a critical review. Rev Infect
Dis 1991;13:430--47.
Weber DJ, Barbee SL, Sobsey MD, Rutala WA. The effect of blood on the antiviral activity of sodium hypochlorite, a phenolic, and a
quaternary ammonium compound. Infect Control Hosp Epidemiol 1999;20:821--7.
Suzuki A, Namba Y, Matsuura M, Horisawa A. Bacterial contamination of floors and other surfaces in operating rooms: a five-year survey. J
Hyg (Lond) 1984;93:559--66.
Richet H, McNeil M, Peters W, et al.
Aspergillus flavus in a bone marrow transplant unit (BMTU): Pseudofungemia traced to hallway
carpeting [Abstract F-23]. In: Abstracts of the
89th Annual Meeting of the American Society for Microbiology. New Orleans, LA: American Society
for Microbiology, 1989:462.
Taplin D, Mertz PM. Flower vases in hospitals as reservoirs for pathogens. Lancet 1973;2:1279--81.
Kates SG, McGinley KJ, Larson EL, Leyden JJ. Indigenous multiresistant bacteria from flowers in hospital and nonhospital environments. Am
J Infect Control 1991;19:156--61.
Bartzokas CA, Holley MP, Sharp CA. Bacteria in flower vase water: incidence and significance in general ward practice. Br J Surg 1975;62:295--7.
Siegman-Igra Y, Shalem A, Berger SA, Livio S, Michaeli D. Should potted plants be removed from hospital wards? J Hosp Infect 1986;7:82--5.
Lass-Flörl C, Rath P, Niederwieser D, et al.
Aspergillus terreus infections in haematological malignancies: molecular epidemiology suggests
association with in-hospital plants. J Hosp Infect 2000;46:31--5.
Burgess NR. Hospital design and cockroach control. Trans R Soc Trop Med Hyg 1984;78:293--4.
Lukin LG. Human cutaneous myiasis in Brisbane: a prospective study. Med J Aust 1989;150:237--40.
Bruesch J. Institutional pest management: current trends. Exec Housekeep Today 1994;15:6--12.
Allen BW. Excretion of viable tubercle bacilli by
Blatta orientalis (the oriental cockroach) following ingestion of heat-fixed sputum smears: a
laboratory investigation. Trans R Soc Trop Med Hyg 1987;81:98--9.
Laszlo A. Technical guide: sputum examination for tuberculosis by direct microscopy in low income countries.
5th ed. Paris, France: International Union Against Tuberculosis and Lung Disease, 2000. Available at
http://www.iuatld.org/pdf/en/guides_publications/microscopy_guide.pdf.
Gerding DN, Johnson S, Peterson LR, Mulligan ME, Silva J
Jr. Clostridium difficile-associated diarrhea and colitis. Infect Control Hosp
Epidemiol 1995;16:459--77.
Weber DJ, Rutala WA. Role of environmental contamination in the transmission of vancomycin-resistant enterococci. Infect Control Hosp
Epidemiol 1997;18:306--9.
Lai KK, Kelley AL, Melvin ZS, Belliveau PP, Fontecchio SA. Failure to eradicate vacomycin-resistant enterococci in a university hospital and the
cost of barrier precautions. Infect Control Hosp Epidemiol 1998;19:647--52.
Byers KE, Durbin LJ, Simonton BM, Anglim AM, Adal KA, Farr BM. Disinfection of hospital rooms contaminated with
vancomycin-resistant Enterococcus faecium. Infect Control Hosp Epidemiol 1998;19:261--4.
Bradley CR, Fraise AP. Heat and chemical resistance of enterococci. J Hosp Infect 1996;34:191--6.
Anderson RL, Carr JH, Bond WW, Favero MS. Susceptibility of vancomycin-resistant enterococci to environmental disinfectants. Infect
Control Hosp Epidemiol 1997;18:195--9.
Saurina G, Landman D, Quale JM. Activity of disinfectants against vancomycin-resistant
Enterococcus faecium. Infect Control Hosp
Epidemiol 1997;18:345--7.
Rutala WA, Stiegel MM, Sarubbi FA, Weber DJ. Susceptibility of antibiotic-susceptible and antibiotic-resistant hospital bacteria to
disinfectants. Infect Control Hosp Epidemiol 1997;18:417--21.
Sehulster LM, Anderson RL. Susceptibility of glycopeptide-intermediate resistant
Staphylococcus aureus (GISA) to surface disinfectants, hand
washing chemicals, and a skin antiseptic [Abstract Y-3]. In: Abstracts of the
98th General Meeting, American Society for Microbiology. Atlanta, GA:
American Society for Microbiology, 1998.
Layton MC, Perez M, Heald P, Patterson JE. An outbreak of mupirocin-resistant
Staphylococcus aureus on a dermatology ward associated with
an environmental reservoir. Infect Control Hosp Epidemiol 1993; 14:369--75.
Karanfil LV, Murphy M, Josephson A, et al. A cluster of vancomycin-resistant
Enterococcus faecium in an intensive care unit. Infect Control
Hosp Epidemiol 1992;13:195--200.
Boyce JM, Opal SM, Chow JW, et al. Outbreak of multidrug-resistant
Enterococcus faecium with transferable
vanB class vancomycin resistance. J Clin Microbiol 1994;32:1148--53.
Rhinehart E, Smith NE, Wennersten C, et al. Rapid dissemination of beta-lactamase-producing, aminoglycoside-resistant
Enterococcus faecalis among patients and staff on an infant-toddler surgical ward. N Engl J Med 1990;323:1814--8.
Livornese LL Jr, Dias S, Samel C, et al. Hospital-acquired infection with vancomycin-resistant
Enterococcus faecium transmitted by
electronic thermometers. Ann Intern Med 1992;117:112--6.
Zervos MJ, Kauffman CA, Therasse PM, Bergman AG, Mikesell TS,
Schaberg DR. Nosocomial infection by gentamicin-resistant
Streptococcus faecalis: an epidemiologic study. Ann Intern Med 1987;106:687--91.
Worsley MA. Infection control and prevention of
Clostridium difficile infection. J Antimicrobial Chemother 1998;41(suppl C):59--66.
Lloyd-Evans N, Springthorpe VS, Sattar SA. Chemical disinfection of human rotavirus-contaminated inanimate surfaces. J Hyg (Lond)
1986;97:163--73.
Rutala WA, Weber DJ. Creutzfeldt-Jakob disease: recommendations for disinfection and sterilization. Clin Infect Dis 2001;32:1348--56.
Kimberlin RH, Walker CA, Millson GC, et al. Disinfection studies with two strains of mouse-passaged scrapie agent: guidelines for
Creutzfeldt-Jakob and related agents. J Neurol Sci 1983;59:355--69.
Rosenberg RN, White CL, Brown P, et al. Precautions in handling tissues, fluids, and other contaminated materials from patients with documented
or suspected Creutzfeldt-Jakob disease. Ann Neurol 1986;19:75--7.
Taylor DM. Inactivation of the unconventional agents of scrapie, bovine spongiform encephalopathy, and Creutzfeldt-Jakob disease. J Hosp
Infect 1991; 18(suppl A):141--6.
Budka H, Aguzzi A, Brown P, et al. Tissue handling in suspected Creutzfeldt-Jakob disease (CJD) and other human spongiform
encephalopathies (prion diseases). Brain Pathol 1995;5:319--22.
Ironside JW, Bell JE. The `high-risk' neuropathological autopsy in AIDS and Creutzfeldt-Jakob disease: principles and practice. Neuropathol
Appl Neurobiol 1996;22:388--93.
World Health Organization. WHO infection control guidelines for transmissible spongiform encephalopathies: report of a WHO
consultation. Geneva, Switzerland: World Health Organization, 1999.
Available at http://www.who.int/emc-documents/tse/whocdscsraph2003c.html.
Bond WW, Sehulster LM. Microbiological assay of environmental and medical-device surfaces [Section 11]. In: Isenberg HD, ed.
Clinical microbiology procedures.Washington, DC: American Society for Microbiology Press, 2003 (in press).
Clesceri LS, Greenberg AE, Eaton AD, eds. Standard methods for the examination of water and wastewater.
20th ed. Washington, DC: American Public Health Association, American Water Works Association, Water Environment Foundation, 1998:9-1--9-41.
Buttner MP, Willeke K, Grinshpun SA. Sampling and analysis of airborne microorganisms [Chapter 68]. In: Manual of environmental
microbiology. Hurst CJ, Knudsen GR, McInerney MJ, Stetzenbach LD, Walter MV, eds. Washington, DC: American Society for Microbiology Press, 1997:629--40.
Jensen PA, Schafer MP. Sampling and characterization of bioaerosols. In: NIOSH manual of analytical methods. Cincinnati, OH: US Department
of Health and Human Services, National Institute for Occupational Safety and Health, 1998:82--112. Available at
http://www.cdc.gov/niosh/nmam/pdfs/chapter-j.pdf.
International Organization for Standardization. Sterilization of medical devices---microbiological methods [Part 1]. Paramus, NJ:
International Organization for Standardization, 1995. ISO Standard 11737-1.
Streifel AJ. Air cultures for fungi. In: Isenberg HD, ed. Clinical microbiology procedures handbook. Washington, DC: American Society
for Microbiology Press, 1992:11.8.1--.7.
Wolf HW, Skaliy P, Hall LB, et al. Sampling microbiological aerosols. Washington, DC: US Department of Health, Education and Welfare,
Public Health Service, 1964. Public Health Service publication no. 686. (Monograph no. 60).
Hambraeus A, Malmborg AS. Is a bed centre in a hospital a hygienic hazard? J Hyg (Lond) 1982;88:143--7.
McDonald LL, Pugliese G. Textile processing service [Chapter 66]. In: Mayhall CG, ed. Hospital epidemiology and infection control.
2nd ed. Philadelphia, PA: Lippincott Williams and Wilkins, 1999:1031--4.
Barrie D, Hoffman PN, Wilson JA, Kramer JM. Contamination of hospital linen by
Bacillus cereus. Epidemiol Infect 1994;113:297--306.
Legnani PP, Leoni E. Factors affecting the bacteriological contamination of commercial washing machines [German]. Zentralbl Hyg
1997;200:319--33.
Joint Committee on Healthcare Laundry Guidelines. Guidelines for healthcare linen service. Hallendale, FL: Textile Rental Service Association
of America, 1999.
Greene VW. Microbiological contamination control in hospitals: part 6 --- roles of central service and the laundry. Hospitals JAHA 1970;44:98--103.
Association for the Advancement of Medical Instrumentation. Processing of reusable surgical textiles for use in health care facilities:
ANSI/AAMI Recommended Practice ST65:2000; Arlington, VA: Association for the Advancement of Medical Instrumentation, 2000:16.
Hughes HG. Chutes in hospitals. Can Hosp 1964;41:56--7,87.
Michaelsen GS. Designing linen chutes to reduce spread of infectious organisms. Hospitals JAHA 1965;39:116--9.
Hoch KW. Laundry chute cleaning recommendations [Letter]. Infect Control 1982;3:360.
Whyte W, Baird G, Annand R. Bacterial contamination on the surface of hospital linen chutes. J Hyg (Lond) 1969;67:427--35.
Taylor LJ. Segregation, collection, and disposal of hospital laundry and waste. J Hosp Infect 1988;11(suppl A):57--63.
Walter WG, Schillinger JE. Bacterial survival in laundered fabrics. Appl Microbiol 1975; 29:368--73.
Belkin NL. Aseptics and aesthetics of chlorine bleach: can its use in laundering be safely abandoned? Am J Infect Control 1998;26:149--51.
Blaser MJ, Smith PE, Cody HJ, Wang WL, LaForce FM. Killing of fabric-associated bacteria in hospital laundry by low-temperature washing. J
Infect Dis 1984;149:48--57.
Jaska JM, Fredell DL. Impact of detergent systems on bacterial survival on laundered fabrics. Appl Environ Microbiol 1980;39:743--8.
Battles DR, Vesley D. Wash water temperature and sanitation in the hospital laundry. J Environ Health 1981;43:244--50.
Christian RR, Manchester JT, Mellor MT. Bacteriological quality of fabrics washed at lower-than-standard temperatures in a hospital laundry
facility. Appl Environ Microbiol 1983;45:591--7.
Smith JA, Neil KR, Davidson CG, Davidson RW. Effect of water temperature on bacterial killing in laundry. Infect Control 1987;8:204--9.
Tompkins DS, Johnson P, Fittall BR. Low-temperature washing of patients' clothing: effects of detergent with disinfectant and a tunnel drier
on bacterial survival. J Hosp Infect 1988;12:51--8.
Ayliffe GA, Collins BJ, Taylor LJ. Laundering [Chapter 11]. In: Hospital-acquired infection: principles and prevention. Bristol, UK: John Wright
and Sons,1982:101--6.
Meyer CL, Eitzen HE, Schreiner RL, Gfell MA, Moye L, Kleiman MB. Should linen in newborn intensive care units be autoclaved?
Pediatrics 1981;67:362--4.
Wagg RE. Disinfection of textiles in laundering and dry cleaning. Chemistry and Industry 1965;44:1830--4.
Bates CJ, Wilcox MH, Smith TL, Spencer RC. The efficacy of a hospital dry cleaning cycle in disinfecting material contaminated with bacteria
and viruses. J Hosp Infect 1993;23:255--62.
Oehnel E. Drycleaning in the hospital laundry. Can Hosp 1971;48:66--7.
US Environmental Protection Agency. Consumer Products Treated with Pesticides. Office of Pesticide Programs. Available at
http://www.epa.gov/pesticides/factsheets/.
Fujita K, Lilly HA, Kidson A, Ayliffe GA.
Gentamicin-resistant Pseudomonas aeruginosa infection from mattresses in a burns unit. Br Med
J 1981;283:219--20.
Sherertz RJ, Sullivan ML. An outbreak of infections
with Acinetobacter calcoaceticus in burn patients: contamination of patients' mattresses. J Infect Dis 1985;151:252--8.
Ndawula EM, Brown L. Mattresses as reservoirs of epidemic methicillin-resistant
Staphylococcus aureus [Letter]. Lancet 1991;337:488.
O'Donoghue MA, Allen KD. Costs of an outbreak of wound infections in an orthopaedic ward. J Hosp Infect 1992;22:73--9.
Weernink A, Severin WP, Tjernberg I, Dijkshoorn L. Pillows, an unexpected source of
Acinetobacter. J Hosp Infect 1995;29:189--99.
Scheidt A, Drusin LM. Bacteriologic contamination in an air-fluidized bed. J Trauma 1983;23:241--2.
Freeman R, Gould FK, Ryan DW, Chamberlain J, Sisson PR. Nosocomial infection due to
Enterococci attributed to a fluidized microsphere bed.
The value of pyrolysis mass spectrometry. J Hosp Infect 1994;27:187--93.
Clancy MJ. Nosocomial infection and microsphere beds [Letter]. Lancet 1993;342:680--1.
Clancy MJ. Nosocomial infection due to
Enterococci attributed to a fluidized microsphere bed [Letter]. J Hosp Infect 1994;28:324--5.
Jacobsen E, Gurevich I, Cunha BA. Air-fluidized beds and negative-pressure isolation rooms [Letter]. Am J Infect Control 1993;21:217--8.
Duncan SL, APIC Guideline Committee. APIC state-of-the-art report: the implications of service animals in healthcare settings. Am J Infect
Control 2000;28:170--80.
Murray AB, Ferguson AC, Morrison BJ. The frequency and severity of cat allergy vs. dog allergy in atopic children. J Allergy Clin
Immunol 1983;72:145--9.
Delta Society. Standards of practice for animal-assisted activities and animal-assisted therapy. Renton, WA: Delta Society, 1996.
Fox JG. Transmissible drug resistance in
Shigella and Salmonella isolated from pet monkeys and their owners. J Med Primatol 1975;4:165--71.
Ostrowski SR, Leslie MJ, Parrott T, Abelt S, Piercy PE. B-virus from pet macaque monkeys: an emerging threat in the United States? Emerg
Infect Dis 1998;4:117--21.
Saylor K. Pet visitation program. J Gerontol Nurs 1998;24:36--8.
Draper RJ, Gerber GJ, Layng EM. Defining the role of pet animals in psychotherapy. Psychiatr J Univ Ottawa 1990;15:169--72.
US Department of Justice. Americans With Disabilities Act. Nondiscrimination on the basis of disability by public accommodations and
in commercial facilities. Public Law 101-336. Title III, Public accomodations operated by private entities, Sect. 302. Prohibition of discrimination
by public accomodations, 42 USC 12101 et seq., 1990.
US Department of Agriculture. Public Law 99-198. Food Security Act of 1985, Subtitle F --- Animal Welfare. Title 7, United States Code,
Chapter 54, Section 2131.
CDC, National Institutes of Health. Biosafety in microbiological and biomedical laboratories.
4th ed. Washington, DC: US Department of
Health and Human Services, Public Health Service, CDC; DHHS publication no. (CDC) 93-8395.
US Department of Labor, Occupational Safety and Health
Administration. Personal protective equipment for general industry; final rule. 29 CFR 1910
§ 1910.132, 1910.138. Federal Register 1994;59:16334--64.
US Department of Transportation. Hazardous Materials Regulations. 49 CFR Parts 171--180, Division 6.2; and Hazardous materials: revision
to standards for infectious substances and genetically-modified microorganisms; proposed rule. Federal Register 1998;63:46843--59.
US Postal Service. C 023.8.0 Hazardous materials: infectious substances (hazard class 6, division 6.2). Washington, D.C.: US Government
Printing Office. Available at http://pe.usps.gov/text/dmm/c023.htm.
Greene R, Miele DJ, Slavik NS. Technical assistance manual: state regulatory oversight of medical waste treatment technologies,
2nd ed. State and Territorial Association on Alternative Treatment Technologies, 1994.
National Institute for Occupational Safety and Health. NIOSH alert: preventing needlestick injuries in health care settings. Cincinnati, OH:
US Department of Health and Human Services, National Institute for Occupational Safety and Health, 1999. DHHS (NIOSH) publication no.
2000-108.
Weber AM, Boudreau Y, Mortimer VD. Health hazard evaluation report: Stericycle, Inc., Morton, WA. Cincinnati, OH: National Institute
for Occupational Safety and Health, Hazard Evaluations and Technical Assistance Branch, 1998. HETA 98-0027-2709.
Johnson KR, Braden CR, Cairns KL, et al. Transmission of
Mycobacterium tuberculosis from medical waste. JAMA 2000;284:1683--8.
Emery R, Sprau D, Lao YJ, Pryor W. Release of bacterial aerosols during infectious waste compaction: an initial hazard evaluation for
healthcare workers. Am Ind Hyg Assoc J 1992;53:339--45.
US Department of Health and Human Services, CDC. Additional requirements for facilities transferring or receiving select agents; final rule. 42 CFR Part 72. Federal Register 1996;61(207):55189--200.
CDC, Office of Biosafety, Hospital Infections Program. Recommendations on infective waste, Atlanta, GA: Department of Health and
Human Services, CDC, 1988:1--6.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
Disclaimer
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.