Guidelines for Preventing the Transmission of
Mycobacterium tuberculosis in Health-Care Facilities, 1994
Acknowledgments
Drafts of this document have been reviewed by leaders of numerous
medical,
scientific, public health, and labor organizations and others
expert in
tuberculosis, acquired immunodeficiency syndrome, infection
control, hospital
epidemiology, microbiology, ventilation, industrial hygiene,
nursing, dental
practice, or emergency medical services. We thank the many
organizations and
individuals for their thoughtful comments, suggestions, and
assistance.
TB Infection-Control Guidelines Work Group
Carmine J. Bozzi
Dale R. Burwen, M.D.
Samuel W. Dooley, M.D.
Patricia M. Simone, M.D.
National Center for Prevention Services
Consuelo Beck-Sague, M.D.
Elizabeth A. Bolyard, R.N., M.P.H.
William R. Jarvis, M.D.
National Center for Infectious Diseases
Philip J. Bierbaum
Christine A. Hudson, M.P.H.
Robert T. Hughes
Linda S. Martin, Ph.D.
Robert J. Mullan, M.D.
National Institute for Occupational Safety and Health
Brian M. Willis, J.D., M.P.H.
Office of the Director
Executive Summary
This document updates and replaces all previously published
guidelines for
the prevention of Mycobacterium tuberculosis transmission in
health-care
facilities. The purpose of this revision is to emphasize the
importance of a)
the hierarchy of control measures, including administrative and
engineering
controls and personal respiratory protection; b) the use of risk
assessments
for developing a written tuberculosis (TB) control plan; c) early
identifi-
cation and management of persons who have TB; d) TB screening
programs for
health-care workers (HCWs); e) HCW training and education; and f)
the
evaluation of TB infection-control programs.
Transmission of M. tuberculosis is a recognized risk to patients
and HCWs in
health-care facilities. Transmission is most likely to occur from
patients
who have unrecognized pulmonary or laryngeal TB, are not on
effective anti-TB
therapy, and have not been placed in TB isolation. Several recent
TB
outbreaks in health-care facilities, including outbreaks of
multidrug-
resistant TB, have heightened concern about nosocomial
transmission. Patients
who have multidrug-resistant TB can remain infectious for prolonged
periods,
which increases the risk for nosocomial and/or occupational
transmission of
M. tuberculosis. Increases in the incidence of TB have been
observed in some
geographic areas; these increases are related partially to the high
risk for
TB among immunosuppressed persons, particularly those infected with
human
immunodeficiency virus (HIV). Transmission of M. tuberculosis to
HIV-infected
persons is of particular concern because these persons are at high
risk for
developing active TB if they become infected with the bacteria.
Thus, health-
care facilities should be particularly alert to the need for
preventing
transmission of M. tuberculosis in settings in which HIV-infected
persons
work or receive care.
Supervisory responsibility for the TB infection-control program
should be
assigned to a designated person or group of persons who should be
given the
authority to implement and enforce TB infection-control policies.
An
effective TB infection-control program requires early
identification,
isolation, and treatment of persons who have active TB. The primary
emphasis
of TB infection-control plans in health-care facilities should be
achieving
these three goals by the application of a hierarchy of control
measures,
including a) the use of administrative measures to reduce the risk
for
exposure to persons who have infectious TB, b) the use of
engineering
controls to prevent the spread and reduce the concentration of
infectious
droplet nuclei, and c) the use of personal respiratory protective
equipment
in areas where there is still a risk for exposure to M.
tuberculosis (e.g.,
TB isolation rooms). Implementation of a TB infection-control
program
requires risk assessment and development of a TB infection-control
plan;
early identification, treatment, and isolation of infectious TB
patients;
effective engineering controls; an appropriate respiratory
protection
program; HCW TB training, education, counseling, and screening; and
evaluation of the program's effectiveness.
Although completely eliminating the risk for transmission of M.
tuberculosis
in all health-care facilities may not be possible at the present
time,
adherence to these guidelines should reduce the risk to persons in
these
settings. Recently, nosocomial TB outbreaks have demonstrated the
substantial
morbidity and mortality among patients and HCWs that have been
associated
with incomplete implementation of CDC's Guidelines for Preventing
the
Transmission of Tuberculosis in Health-Care Facilities, with
Special Focus on
HIV-Related Issues published in 1990. * Follow-up investigations at
some of
these hospitals have documented that complete implementation of
measures
similar or identical to those in the 1990 TB Guidelines
significantly reduced
or eliminated nosocomial transmission of M. tuberculosis to
patients and/or
HCWs.
Introduction
Purpose of Document
In April 1992, the National MDR-TB Task Force published the
National
Action Plan to Combat Multidrug-Resistant Tuberculosis (1).
The
publication was a response to reported nosocomial outbreaks
of
tuberculosis (TB), including outbreaks of
multidrug-resistant TB
(MDR-TB), and the increasing incidence of TB in some
geographic
areas. The plan called for the update and revision of the
guidelines
for preventing nosocomial transmission of Mycobacterium
tuberculosis
published December 7, 1990 (2).
Public meetings were held in October 1992 and January 1993
to discuss
revision of the 1990 TB Guidelines (2). CDC received
considerable
input on various aspects of infection control, including
health-care
worker (HCW) education; administrative controls (e.g.,
having
protocols for the early identification and management of
patients who
have TB); the need for more specific recommendations
regarding
ventilation; and clarification on the use of respiratory
protection
in health-care settings. On the basis of these events and
the input
received, on October 12, 1993, CDC published in the Federal
Register
the Draft Guidelines For Preventing the Transmission of
Tuberculosis
in Health-Care Facilities, Second Edition (3). During and
after the
90-day comment period following publication of this draft,
CDC's TB
Infection-Control Guidelines Work Group received and
reviewed more
than 2,500 comments.
The purpose of this document is to make recommendations for
reducing
the risk for transmitting M. tuberculosis to HCWs,
patients,
volunteers, visitors, and other persons in these settings.
The
information also may serve as a useful resource for
educating HCWs
about TB.
These recommendations update and replace all previously
published CDC
recommendations for TB infection control in health-care
facilities
(2,4). The recommendations in this document are applicable
primarily
to inpatient facilities in which health care is provided
(e.g.,
hospitals, medical wards in correctional facilities,
nursing homes,
and hospices). Recommendations applicable to
ambulatory-care
facilities, emergency departments, home-health-care
settings,
emergency medical services, medical offices, dental
settings, and
other facilities or residential settings that provide
medical care
are provided in separate sections, with cross-references to
other
sections of the guidelines if appropriate.
Designated personnel at health-care facilities should
conduct a risk
assessment for the entire facility and for each area ** and
occupa-
tional group, determine the risk for nosocomial or
occupational
transmission of M. tuberculosis, and implement an
appropriate TB
infection-control program. The extent of the TB
infection-control
program may range from a simple program emphasizing
administrative
controls in settings where there is minimal risk for
exposure to M.
tuberculosis, to a comprehensive program that includes
administrative
controls, engineering controls, and respiratory protection
in
settings where the risk for exposure is high. In all
settings,
administrative measures should be used to minimize the
number of HCWs
exposed to M. tuberculosis while still providing optimal
care for TB
patients. HCWs providing care to patients who have TB
should be
informed about the level of risk for transmission of M.
tuberculosis
and the appropriate control measures to minimize that risk.
In this document, the term "HCWs" refers to all the paid
and unpaid
persons working in health-care settings who have the
potential for
exposure to M. tuberculosis. This may include, but is not
limited to,
physicians; nurses; aides; dental workers; technicians;
workers in
laboratories and morgues; emergency medical service (EMS)
personnel;
students; part-time personnel; temporary staff not employed
by the
health-care facility; and persons not involved directly in
patient
care but who are potentially at risk for occupational
exposure to M.
tuberculosis (e.g., volunteer workers and dietary,
housekeeping,
maintenance, clerical, and janitorial staff).
Although the purpose of this document is to make
recommendations for
reducing the risk for transmission of M. tuberculosis in
health-care
facilities, the process of implementing these
recommendations must
safeguard, in accordance with applicable state and federal
laws, the
confidentiality and civil rights of persons who have TB.
Epidemiology, Transmission, and Pathogenesis of TB
The prevalence of TB is not distributed evenly throughout
all
segments of the U.S. population. Some subgroups or persons
have a
higher risk for TB either because they are more likely than
other
persons in the general population to have been exposed to
and
infected with M. tuberculosis or because their infection is
more
likely to progress to active TB after they have been
infected (5). In
some cases, both of these factors may be present. Groups of
persons
known to have a higher prevalence of TB infection include
contacts of
persons who have active TB, foreign-born persons from areas
of the
world with a high prevalence of TB (e.g., Asia, Africa, the
Caribbean, and Latin America), medically underserved
populations
(e.g., some African-Americans, Hispanics, Asians and
Pacific
Islanders, American Indians, and Alaskan Natives), homeless
persons,
current or former correctional-facility inmates,
alcoholics,
injecting-drug users, and the elderly. Groups with a higher
risk for
progression from latent TB infection to active disease
include
persons who have been infected recently (i.e., within the
previous 2
years), children less than 4 years of age, persons with
fibrotic
lesions on chest radiographs, and persons with certain
medical
conditions (i.e., human immunodeficiency virus {HIV}
infection,
silicosis, gastrectomy or jejuno-ileal bypass, being
greater than or
equal to 10% below ideal body weight, chronic renal failure
with
renal dialysis, diabetes mellitus, immunosuppression
resulting from
receipt of high-dose corticosteroid or other
immunosuppressive
therapy, and some malignancies) (5).
M. tuberculosis is carried in airborne particles, or
droplet nuclei,
that can be generated when persons who have pulmonary or
laryngeal TB
sneeze, cough, speak, or sing (6). The particles are an
estimated 1-5
um in size, and normal air currents can keep them airborne
for
prolonged time periods and spread them throughout a room or
building
(7). Infection occurs when a susceptible person inhales
droplet
nuclei containing M. tuberculosis, and these droplet nuclei
traverse
the mouth or nasal passages, upper respiratory tract, and
bronchi to
reach the alveoli of the lungs. Once in the alveoli, the
organisms
are taken up by alveolar macrophages and spread throughout
the body.
Usually within 2-10 weeks after initial infection with M.
tubercu-
losis, the immune response limits further multiplication
and spread
of the tubercle bacilli; however, some of the bacilli
remain dormant
and viable for many years. This condition is referred to as
latent TB
infection. Persons with latent TB infection usually have
positive
purified protein derivative (PPD)-tuberculin skin-test
results, but
they do not have symptoms of active TB, and they are not
infectious.
In general, persons who become infected with M.
tuberculosis have
approximately a 10% risk for developing active TB during
their
lifetimes. This risk is greatest during the first 2 years
after
infection. Immunocompromised persons have a greater risk
for the
progression of latent TB infection to active TB disease;
HIV
infection is the strongest known risk factor for this
progression.
Persons with latent TB infection who become coinfected with
HIV have
approximately an 8%-10% risk per year for developing active
TB (8).
HIV-infected persons who are already severely
immunosuppressed and
who become newly infected with M. tuberculosis have an even
greater
risk for developing active TB (9-12).
The probability that a person who is exposed to M.
tuberculosis will
become infected depends primarily on the concentration of
infectious
droplet nuclei in the air and the duration of exposure.
Character-
istics of the TB patient that enhance transmission include
a) disease
in the lungs, airways, or larynx; b) presence of cough or
other
forceful expiratory measures; c) presence of acid-fast
bacilli (AFB)
in the sputum; d) failure of the patient to cover the mouth
and nose
when coughing or sneezing; e) presence of cavitation on
chest
radiograph; f) inappropriate or short duration of
chemotherapy; and
g) administration of procedures that can induce coughing or
cause
aerosolization of M. tuberculosis (e.g., sputum induction).
Environ-
mental factors that enhance the likelihood of transmission
include a)
exposure in relatively small, enclosed spaces; b)
inadequate local or
general ventilation that results in insufficient dilution
and/or
removal of infectious droplet nuclei; and c) recirculation
of air
containing infectious droplet nuclei. Characteristics of
the persons
exposed to M. tuberculosis that may affect the risk for
becoming
infected are not as well defined. In general, persons who
have been
infected previously with M. tuberculosis may be less
susceptible to
subsequent infection. However, reinfection can occur among
previously
infected persons, especially if they are severely
immunocompromised.
Vaccination with Bacille of Calmette and Guerin (BCG)
probably does
not affect the risk for infection; rather, it decreases the
risk for
progressing from latent TB infection to active TB (13).
Finally,
although it is well established that HIV infection
increases the
likelihood of progressing from latent TB infection to
active TB, it
is unknown whether HIV infection increases the risk for
becoming
infected if exposed to M. tuberculosis.
Risk for Nosocomial Transmission of M. tuberculosis
Transmission of M. tuberculosis is a recognized risk in
health-care
facilities (14-22). The magnitude of the risk varies
considerably by
the type of health-care facility, the prevalence of TB in
the
community, the patient population served, the HCW's
occupational
group, the area of the health-care facility in which the
HCW works,
and the effectiveness of TB infection-control
interventions. The risk
may be higher in areas where patients with TB are provided
care
before diagnosis and initiation of TB treatment and
isolation
precautions (e.g., in clinic waiting areas and emergency
departments)
or where diagnostic or treatment procedures that stimulate
coughing
are performed. Nosocomial transmission of M. tuberculosis
has been
associated with close contact with persons who have
infectious TB and
with the performance of certain procedures (e.g.,
bronchoscopy {17},
endotracheal intubation and suctioning {18}, open abscess
irrigation
{20}, and autopsy {21,22}). Sputum induction and aerosol
treatments
that induce coughing may also increase the potential for
transmission
of M. tuberculosis (23,24). Personnel of health-care
facilities
should be particularly alert to the need for preventing
transmission
of M. tuberculosis in those facilities in which
immunocompromised
persons (e.g., HIV-infected persons) work or receive care
--
especially if cough-inducing procedures, such as sputum
induction and
aerosolized pentamidine treatments, are being performed.
Several TB outbreaks among persons in health-care
facilities have
been reported recently (11,24-28; CDC, unpublished data).
Many of
these outbreaks involved transmission of
multidrug-resistant strains
of M. tuberculosis to both patients and HCWs. Most of the
patients
and some of the HCWs were HIV-infected persons in whom new
infection
progressed rapidly to active disease. Mortality associated
with those
outbreaks was high (range: 43%-93%). Furthermore, the
interval
between diagnosis and death was brief (range of median
intervals:
4-16 weeks). Factors contributing to these outbreaks
included delayed
diagnosis of TB, delayed recognition of drug resistance,
and delayed
initiation of effective therapy -- all of which resulted in
prolonged
infectiousness, delayed initiation and inadequate duration
of TB
isolation, inadequate ventilation in TB isolation rooms,
lapses in TB
isolation practices and inadequate precautions for
cough-inducing
procedures, and lack of adequate respiratory protection.
Analysis of
data collected from three of the health-care facilities
involved in
the outbreaks indicates that transmission of M.
tuberculosis
decreased significantly or ceased entirely in areas where
measures
similar to those in the 1990 TB Guidelines were implemented
(2,29-
32). However, several interventions were implemented
simultaneously,
and the effectiveness of the separate interventions could
not be
determined.
Fundamentals of TB Infection Control
An effective TB infection-control program requires early
identifi-
cation, isolation, and effective treatment of persons who
have active
TB. The primary emphasis of the TB infection-control plan
should be
on achieving these three goals. In all health-care
facilities,
particularly those in which persons who are at high risk
for TB work
or receive care, policies and procedures for TB control
should be
developed, reviewed periodically, and evaluated for
effectiveness to
determine the actions necessary to minimize the risk for
transmission
of M. tuberculosis.
The TB infection-control program should be based on a
hierarchy of
control measures. The first level of the hierarchy, and
that which
affects the largest number of persons, is using
administrative
measures intended primarily to reduce the risk for exposing
uninfected persons to persons who have infectious TB. These
measures
include a) developing and implementing effective written
policies and
protocols to ensure the rapid identification, isolation,
diagnostic
evaluation, and treatment of persons likely to have TB; b)
imple-
menting effective work practices among HCWs in the
health-care
facility (e.g., correctly wearing respiratory protection
and keeping
doors to isolation rooms closed); c) educating, training,
and
counseling HCWs about TB; and d) screening HCWs for TB
infection and
disease.
The second level of the hierarchy is the use of engineering
controls
to prevent the spread and reduce the concentration of
infectious
droplet nuclei. These controls include a) direct source
control using
local exhaust ventilation, b) controlling direction of
airflow to
prevent contamination of air in areas adjacent to the
infectious
source, c) diluting and removing contaminated air via
general
ventilation, and d) air cleaning via air filtration or
ultraviolet
germicidal irradiation (UVGI).
The first two levels of the hierarchy minimize the number
of areas in
the health-care facility where exposure to infectious TB
may occur,
and they reduce, but do not eliminate, the risk in those
few areas
where exposure to M. tuberculosis can still occur (e.g.,
rooms in
which patients with known or suspected infectious TB are
being
isolated and treatment rooms in which cough-inducing or
aerosol-
generating procedures are performed on such patients).
Because
persons entering such rooms may be exposed to M.
tuberculosis, the
third level of the hierarchy is the use of personal
respiratory
protective equipment in these and certain other situations
in which
the risk for infection with M. tuberculosis may be
relatively higher.
Specific measures to reduce the risk for transmission of M.
tubercu-
losis include the following:
Assigning to specific persons in the health-care
facility the
supervisory responsibility for designing, implementing,
evaluating, and maintaining the TB infection-control
program
(Section II.A).
Conducting a risk assessment to evaluate the risk for
trans-
mission of M. tuberculosis in all areas of the
health-care
facility, developing a written TB infection-control
program based
on the risk assessment, and periodically repeating the
risk
assessment to evaluate the effectiveness of the TB
infection-
control program (Section II.B).
Developing, implementing, and enforcing policies and
protocols to
ensure early identification, diagnostic evaluation, and
effective
treatment of patients who may have infectious TB
(Section II.C;
Suppl. 2).
Providing prompt triage for and appropriate management
of
patients in the outpatient setting who may have
infectious TB
(Section II.D).
Promptly initiating and maintaining TB isolation for
persons who
may have infectious TB and who are admitted to the
inpatient
setting (Section II.E; Suppl. 1).
Effectively planning arrangements for discharge
(Section II.E).
Developing, installing, maintaining, and evaluating
ventilation
and other engineering controls to reduce the potential
for
airborne exposure to M. tuberculosis (Section II.F;
Suppl. 3).
Developing, implementing, maintaining, and evaluating a
respir-
atory protection program (Section II.G; Suppl. 4).
Using precautions while performing cough-inducing
procedures
(Section II.H; Suppl. 3).
Educating and training HCWs about TB, effective methods
for
preventing transmission of M. tuberculosis, and the
benefits of
medical screening programs (Section II.I).
Developing and implementing a program for routine
periodic
counseling and screening of HCWs for active TB and
latent TB
infection (Section II.J; Suppl. 2).
Promptly evaluating possible episodes of M.
tuberculosis
transmission in health-care facilities, including PPD
skin-test
conversions among HCWs, epidemiologically associated
cases among
HCWs or patients, and contacts of patients or HCWs who
have TB
and who were not promptly identified and isolated
(Section II.K).
Coordinating activities with the local public health
department,
emphasizing reporting, and ensuring adequate discharge
follow-up
and the continuation and completion of therapy (Section
II.L).
Recommendations
Assignment of Responsibility
Supervisory responsibility for the TB infection-control
program
should be assigned to a designated person or group of
persons
with expertise in infection control, occupational
health, and
engineering. These persons should be given the
authority to
implement and enforce TB infection-control policies.
If supervisory responsibility is assigned to a
committee, one
person should be designated as the TB contact person.
Questions
and problems can then be addressed to this person.
Risk Assessment, Development of the TB Infection-Control
Plan, and
Periodic Reassessment
Risk assessment
General
TB infection-control measures for each
health-care
facility should be based on a careful
assessment of the
risk for transmission of M. tuberculosis in
that
particular setting. The first step in
developing the TB
infection-control program should be to conduct
a baseline
risk assessment to evaluate the risk for
transmission of
M. tuberculosis in each area and occupational
group in
the facility (Table_1, Figure_1Figure_1aFigure_1c). Appropriate infection-control
inter-
ventions can then be developed on the basis of
actual
risk. Risk assessments should be performed for
all
inpatient and outpatient settings (e.g.,
medical and
dental offices).
Regardless of risk level, the management of
patients with
known or suspected infectious TB should not
vary.
However, the index of suspicion for infectious
TB among
patients, the frequency of HCW PPD skin
testing, the
number of TB isolation rooms, and other factors
will
depend on whether the risk for transmission of
M.
tuberculosis in the facility, area, or
occupational group
is high, intermediate, low, very low, or
minimal.
The risk assessment should be conducted by a
qualified
person or group of persons (e.g., hospital
epidemi-
ologists, infectious disease specialists,
pulmonary
disease specialists, infection-control
practitioners,
health-care administrators, occupational health
personnel, engineers, HCWs, or local public
health
personnel).
The risk assessment should be conducted for the
entire
facility and for specific areas within the
facility
(e.g., medical, TB, pulmonary, or HIV wards;
HIV,
infectious disease, or pulmonary clinics; and
emergency
departments or other areas where TB patients
might
receive care or where cough-inducing procedures
are
performed). This should include both inpatient
and
outpatient areas. In addition, risk assessments
should be
conducted for groups of HCWs who work
throughout the
facility rather than in a specific area (e.g.,
respir-
atory therapists; bronchoscopists;
environmental
services, dietary, and maintenance personnel;
and
students, interns, residents, and fellows).
Classification of risk for a facility, for a
specific
area, and for a specific occupational group
should be
based on a) the profile of TB in the community;
b) the
number of infectious TB patients admitted to
the area or
ward, or the estimated number of infectious TB
patients
to whom HCWs in an occupational group may be
exposed; and
c) the results of analysis of HCW PPD test
conversions
(where applicable) and possible
person-to-person
transmission of M. tuberculosis (Figure_1Figure_1aFigure_1c).
All TB infection-control programs should
include periodic
reassessments of risk. The frequency of repeat
risk
assessments should be based on the results of
the most
recent risk assessment (Table_2,
Figure_1Figure_1aFigure_1c).
The "minimal-risk" category applies only to an
entire
facility. A "minimal-risk" facility does not
admit TB
patients to inpatient or outpatient areas and
is not
located in a community with TB (i.e., counties
or
communities in which TB cases have not been
reported
during the previous year). Thus, there is
essentially no
risk for exposure to TB patients in the
facility. This
category may also apply to many outpatient
settings
(e.g., many medical and dental offices).
The "very low-risk" category generally applies
only to an
entire facility. A very low-risk facility is
one in which
patients with active TB are not admitted to
inpatient
areas but may receive initial assessment and
diagnostic
evaluation or outpatient management in
outpatient areas
(e.g., ambulatory-care and emergency
departments) and b)
patients who may have active TB and need
inpatient care
are promptly referred to a collaborating
facility. In
such facilities, the outpatient areas in which
exposure
to patients with active TB could occur should
be assessed
and assigned to the appropriate low-,
intermediate-, or
high-risk category. Categorical assignment will
depend on
the number of TB patients examined in the area
during the
preceding year and whether there is evidence of
noso-
comial transmission of M. tuberculosis in the
area. If TB
cases have been reported in the community, but
no
patients with active TB have been examined in
the
outpatient area during the preceding year, the
area can
be designated as very low risk (e.g., many
medical
offices).
The referring and receiving facilities should
establish
a referral agreement to prevent inappropriate
management
and potential loss to follow-up of patients
suspected of
having TB during evaluation in the triage
system of a
very low-risk facility.
In some facilities in which TB patients are
admitted to
inpatient areas, a very low-risk protocol may
be appro-
priate for areas (e.g., administrative areas)
or
occupational groups that have only a very
remote
possibility of exposure to M. tuberculosis.
The very low-risk category may also be
appropriate for
outpatient facilities that do not provide
initial
assessment of persons who may have TB, but do
screen
patients for active TB as part of a limited
medical
screening before undertaking specialty care
(e.g., dental
settings).
"Low-risk" areas or occupational groups are
those in
which a) the PPD test conversion rate is not
greater than
that for areas or groups in which occupational
exposure
to M. tuberculosis is unlikely or than previous
conversion rates for the same area or group, b)
no
clusters *** of PPD test conversions have
occurred, c)
person-to-person transmission of M.
tuberculosis has not
been detected, and d) fewer than six TB
patients are
examined or treated per year.
"Intermediate-risk" areas or occupational
groups are
those in which a) the PPD test conversion rate
is not
greater than that for areas or groups in which
occupa-
tional exposure to M. tuberculosis is unlikely
or than
previous conversion rates for the same area or
group, b)
no clusters of PPD test conversions have
occurred, c)
person-to-person transmission of M.
tuberculosis has not
been detected, and d) six or more patients with
active TB
are examined or treated each year. Survey data
suggest
that facilities in which six or more TB
patients are
examined or treated each year may have an
increased risk
for transmission of M. tuberculosis (CDC,
unpublished
data); thus, areas in which six or more
patients with
active TB are examined or treated each year (or
occupa-
tional groups in which HCWs are likely to be
exposed to
six or more TB patients per year) should be
classified as
"intermediate risk."
"High-risk" areas or occupational groups are
those in
which a) the PPD test conversion rate is
significantly
greater than for areas or groups in which
occupational
exposure to M. tuberculosis is unlikely or than
previous
conversion rates for the same area or group,
and epidemi-
ologic evaluation suggests nosocomial
transmission; or b)
a cluster of PPD test conversions has occurred,
and
epidemiologic evaluation suggests nosocomial
transmission
of M. tuberculosis; or c) possible
person-to-person
transmission of M. tuberculosis has been
detected.
If no data or insufficient data for adequate
determin-
ation of risk have been collected, such data
should be
compiled, analyzed, and reviewed expeditiously.
Community TB profile
A profile of TB in the community that is served
by the
facility should be obtained from the public
health
department. This profile should include, at a
minimum,
the incidence (and prevalence, if available) of
active TB
in the community and the drug-susceptibility
patterns of
M. tuberculosis isolates (i.e., the
antituberculous
agents to which each isolate is susceptible and
those to
which it is resistant) from patients in the
community.
Case surveillance
Data concerning the number of suspected and
confirmed
active TB cases among patients and HCWs in the
facility
should be systematically collected, reviewed,
and used to
estimate the number of TB isolation rooms
needed, to
recognize possible clusters of nosocomial
transmission,
and to assess the level of potential
occupational risk.
The number of TB patients in specific areas of
a facility
can be obtained from laboratory surveillance
data on
specimens positive for AFB smears or M.
tuberculosis
cultures, from infection-control records, and
from
databases containing information about hospital
discharge
diagnoses.
Drug-susceptibility patterns of M. tuberculosis
isolates
from TB patients treated in the facility should
be
reviewed to identify the frequency and patterns
of drug
resistance. This information may indicate a
need to
modify the initial treatment regimen or may
suggest
possible nosocomial transmission or increased
occupa-
tional risk.
Analysis of HCW PPD test screening data
Results of HCW PPD testing should be recorded
in the
individual HCW's employee health record and in
a
retrievable aggregate database of all HCW PPD
test
results. Personal identifying information
should be
handled confidentially. PPD test conversion
rates should
be calculated at appropriate intervals to
estimate the
risk for PPD test conversions for each area of
the
facility and for each specific occupational
group not
assigned to a specific area (Table_2). To
calculate
PPD test conversion rates, the total number of
previously
PPD-negative HCWs tested in each area or group
(i.e., the
denominator) and the number of PPD test
conversions among
HCWs in each area or group (the numerator) must
be
obtained.
PPD test conversion rates for each area or
occupational
group should be compared with rates for areas
or groups
in which occupational exposure to M.
tuberculosis is
unlikely and with previous conversion rates in
the same
area or group to identify areas or groups where
the risk
for occupational PPD test conversions may be
increased.
A low number of HCWs in a specific area may
result in a
greatly increased rate of conversion for that
area,
although the actual risk may not be
significantly greater
than that for other areas. Testing for
statistical
significance (e.g., Fisher's exact test or chi
square
test) may assist interpretation; however, lack
of
statistical significance may not rule out a
problem
(i.e., if the number of HCWs tested is low,
there may not
be adequate statistical power to detect a
significant
difference). Thus, interpretation of individual
situations is necessary.
An epidemiologic investigation to evaluate the
likelihood
of nosocomial transmission should be conducted
if PPD
test conversions are noted (Section II.K.1).
The frequency and comprehensiveness of the HCW
PPD
testing program should be evaluated
periodically to
ensure that all HCWs who should be included in
the
program are being tested at appropriate
intervals. For
surveillance purposes, earlier detection of
transmission
may be enhanced if HCWs in a given area or
occupational
group are tested on different scheduled dates
rather than
all being tested on the same date (Section
II.J.3).
Review of TB patient medical records
The medical records of a sample of TB patients
examined
at the facility can be reviewed periodically to
evaluate
infection-control parameters (Table_1).
Parameters to
examine may include the intervals from date of
admission
until a) TB was suspected, b) specimens for AFB
smears
were ordered, c) these specimens were
collected, d) tests
were performed, and e) results were reported.
Moreover,
the adequacy of the TB treatment regimens that
were used
should be evaluated.
Medical record reviews should note previous
hospital
admissions of TB patients before the onset of
TB
symptoms. Patient-to-patient transmission may
be
suspected if active TB occurs in a patient who
had a
prior hospitalization during which exposure to
another TB
patient occurred or if isolates from two or
more TB
patients have identical characteristic
drug-suscepti-
bility or DNA fingerprint patterns.
Data from the case review should be used to
determine if
there is a need to modify a) protocols for
identifying
and isolating patients who may have infectious
TB, b)
laboratory procedures, c) administrative
policies and
practices, or d) protocols for patient
management.
Observation of TB infection-control practices
Assessing adherence to the policies of the TB
infection-
control program should be part of the
evaluation process.
This assessment should be performed on a
regular basis
and whenever an increase occurs in the number
of TB
patients or HCW PPD test conversions. Areas at
high risk
for transmission of M. tuberculosis should be
monitored
more frequently than other areas. The review of
patient
medical records provides information on HCW
adherence to
some of the policies of the TB
infection-control program.
In addition, work practices related to TB
isolation
(e.g., keeping doors to isolation rooms closed)
should be
observed to determine if employers are
enforcing, and
HCWs are adhering to, these policies and if
patient
adherence is being enforced. If these policies
are not
being enforced or adhered to, appropriate
education and
other corrective action should be implemented.
Engineering evaluation
Results of engineering maintenance measures
should be
reviewed at regular intervals (Table_3).
Data from
the most recent evaluation and from maintenance
procedures and logs should be reviewed
carefully as part
of the risk assessment.
Development of the TB Infection-Control Plan
Based on the results of the risk assessment, a
written TB
infection-control plan should be developed and
implemented
for each area of the facility and for each
occupational group
of HCWs not assigned to a specific area of the
facility
(Table_2; Table_3).
The occurrence of drug-resistant TB in the facility
or the
community, or a relatively high prevalence of HIV
infection
among patients or HCWs in the community, may
increase the
concern about transmission of M. tuberculosis and
may
influence the decision regarding which protocol to
follow
(i.e., a higher-risk classification may be
selected).
Health-care facilities are likely to have a
combination of
low-, intermediate-, and high-risk areas or
occupational
groups during the same time period. The appropriate
protocol
should be implemented for each area or group.
Areas in which cough-inducing procedures are
performed on
patients who may have active TB should, at the
minimum,
implement the intermediate-risk protocol.
Periodic Reassessment
Follow-up risk assessment should be performed at
the interval
indicated by the most recent risk assessment
(Figure_1Figure_1aFigure_1c; Table_2). Based on
the
results of the follow-up assessment, problem
evaluation may
need to be conducted or the protocol may need to be
modified
to a higher- or lower-risk level.
After each risk assessment, the staff responsible
for TB
control, in conjunction with other appropriate
HCWs, should
review all TB control policies to ensure that they
are
effective and meet current needs.
Examples of Risk Assessment
Examples of six hypothetical situations and the means
by which
surveillance data are used to select a TB control
protocol are
described as follows:
Hospital A. The overall HCW PPD test conversion rate in
the
facility is 1.6%. No areas or HCW occupational groups
have a
significantly greater PPD test conversion rate than
areas or
groups in which occupational exposure to M.
tuberculosis is
unlikely (or than previous rates for the same area or
group). No
clusters of PPD test conversions have occurred.
Patient-to-
patient transmission has not been detected. Patients
who have TB
are admitted to the facility, but no area admits six or
more TB
patients per year. The low-risk protocol will be
followed in all
areas.
Hospital B. The overall HCW PPD test conversion rate in
the
facility is 1.8%. The PPD test conversion rate for the
medical
intensive-care unit rate is significantly higher than
all other
areas in the facility. The problem identification
process is
initiated (Section II.K). It is determined that all TB
patients
have been isolated appropriately. Other potential
problems are
then evaluated, and the cause for the higher rate is
not
identified. After consulting the public health
department TB
infection-control program, the high-risk protocol is
followed in
the unit until the PPD test conversion rate is similar
to areas
of the facility in which occupational exposure to TB
patients is
unlikely. If the rate remains significantly higher than
other
areas, further evaluation, including environmental and
procedural
studies, will be performed to identify possible reasons
for the
high conversion rate.
Hospital C. The overall HCW PPD test conversion rate in
the
facility is 2.4%. Rates range from 0 to 2.6% for the
individual
areas and occupational groups. None of these rates is
signifi-
cantly higher than rates for areas in which
occupational exposure
to M. tuberculosis is unlikely. No particular HCW group
has
higher conversion rates than the other groups. No
clusters of HCW
PPD test conversions have occurred. In two of the
areas, HCWs
cared for more than six TB patients during the
preceding year.
These two areas will follow the intermediate-risk
protocol, and
all other areas will follow the low-risk protocol. This
hospital
is located in the southeastern United States, and these
conversion rates may reflect cross-reactivity with
nontuberculous
mycobacteria.
Hospital D. The overall HCW PPD test conversion rate in
the
facility is 1.2%. In no area did HCWs care for six or
more TB
patients during the preceding year. Three of the 20
respiratory
therapists tested had PPD conversions, for a rate of
15%. The
respiratory therapists who had PPD test conversions had
spent all
or part of their time in the pulmonary function
laboratory, where
induced sputum specimens were obtained. A low-risk
protocol is
maintained for all areas and occupational groups in the
facility
except for respiratory therapists. A problem evaluation
is
conducted in the pulmonary function laboratory (Section
II.K). It
is determined that the ventilation in this area is
inadequate.
Booths are installed for sputum induction. PPD testing
and the
risk assessment are repeated 3 months later. If the
repeat
testing at 3 months indicates that no more conversions
have
occurred, the respiratory therapists will return to the
low-risk
protocol.
Hospital E. Hospital E is located in a community that
has a
relatively low incidence of TB. To optimize TB services
in the
community, the four hospitals in the community have
developed an
agreement that one of them (e.g., Hospital G) will
provide all
inpatient services to persons who have suspected or
confirmed TB.
The other hospitals have implemented protocols in their
ambulatory-care clinics and emergency departments to
identify
patients who may have active TB. These patients are
then
transferred to Hospital G for inpatient care if such
care is
considered necessary. After discharge from Hospital G,
they
receive follow-up care in the public health
department's TB
clinic. During the preceding year, Hospital E has
identified
fewer than six TB patients in its ambulatory-care and
emergency
departments and has had no PPD test conversions or
other evidence
of M. tuberculosis transmission among HCWs or patients
in these
areas. These areas are classified as low risk, and all
other
areas are classified as very low risk.
Hospital F. Hospital F is located in a county in which
no TB
cases have been reported during the preceding 2 years.
A risk
assessment conducted at the facility did not identify
any
patients who had suspected or confirmed TB during the
preceding
year. The facility is classified as minimal risk.
Identifying, Evaluating, and Initiating Treatment for
Patients Who
May Have Active TB
The most important factors in preventing transmission of M.
tuber-
culosis are the early identification of patients who may
have
infectious TB, prompt implementation of TB precautions for
such
patients, and prompt initiation of effective treatment for
those who
are likely to have TB.
Identifying patients who may have active TB
Health-care personnel who are assigned
responsibility for TB
infection control in ambulatory-care and inpatient
settings
should develop, implement, and enforce protocols
for the
early identification of patients who may have
infectious TB.
The criteria used in these protocols should be
based on the
prevalence and characteristics of TB in the
population served
by the specific facility. These protocols should be
evaluated
periodically and revised according to the results
of the
evaluation. Review of medical records of patients
who were
examined in the facility and diagnosed as having TB
may serve
as a guide for developing or revising these
protocols.
A diagnosis of TB may be considered for any patient
who has
a persistent cough (i.e., a cough lasting for
greater than or
equal to 3 weeks) or other signs or symptoms
compatible with
active TB (e.g., bloody sputum, night sweats,
weight loss,
anorexia, or fever). However, the index of
suspicion for TB
will vary in different geographic areas and will
depend on
the prevalence of TB and other characteristics of
the
population served by the facility. The index of
suspicion for
TB should be very high in geographic areas or among
groups of
patients in which the prevalence of TB is high
(Section I.B).
Appropriate diagnostic measures should be conducted
and TB
precautions implemented for patients in whom active
TB is
suspected.
Diagnostic evaluation for active TB
Diagnostic measures for identifying TB should be
conducted
for patients in whom active TB is being considered.
These
measures include obtaining a medical history and
performing
a physical examination, PPD skin test, chest
radiograph, and
microscopic examination and culture of sputum or
other
appropriate specimens (6,34,35). Other diagnostic
procedures
(e.g., bronchoscopy or biopsy) may be indicated for
some
patients (36,37).
Prompt laboratory results are crucial to the proper
treatment
of the TB patient and to early initiation of
infection
control. To ensure timely results, laboratories
performing
mycobacteriologic tests should be proficient at
both the
laboratory and administrative aspects of specimen
processing.
Laboratories should use the most rapid methods
available
(e.g., fluorescent microscopy for AFB smears;
radiometric
culture methods for isolation of mycobacteria;
r-nitro-a-
acetylamino-b-hydroxy-proprophenone {NAP} test,
nucleic acid
probes, or high-pressure liquid chromatography
{HPLC} for
species identification; and radiometric methods for
drug-
susceptibility testing). As other more rapid or
sensitive
tests become available, practical, and affordable,
such tests
should be incorporated promptly into the
mycobacteriology
laboratory. Laboratories that rarely receive
specimens for
mycobacteriologic analysis should refer the
specimens to a
laboratory that more frequently performs these
tests.
Results of AFB sputum smears should be available
within 24
hours of specimen collection (38).
The probability of TB is greater among patients who
have
positive PPD test results or a history of positive
PPD test
results, who have previously had TB or have been
exposed to
M. tuberculosis, or who belong to a group at high
risk for TB
(Section I.B). Active TB is strongly suggested if
the
diagnostic evaluation reveals AFB in sputum, a
chest
radiograph suggestive of TB, or symptoms highly
suggestive of
TB. TB can occur simultaneously in immunosuppressed
persons
who have pulmonary infections caused by other
organisms
(e.g., Pneumocystis carinii or Mycobacterium avium
complex)
and should be considered in the diagnostic
evaluation of all
patients who have symptoms compatible with TB
(Suppl. 1;
Suppl. 2).
TB may be more difficult to diagnose among persons
who have
HIV infection (or other conditions associated with
severe
suppression of cell-mediated immunity) because of a
nonclassical clinical or radiographic presentation
and/or the
simultaneous occurrence of other pulmonary
infections (e.g.,
P. carinii pneumonia and M. avium complex). The
difficulty in
diagnosing TB in HIV-infected persons may be
further
compounded by impaired responses to PPD skin tests
(39,40),
the possibly lower sensitivity of sputum smears for
detecting
AFB (41), or the overgrowth of cultures with M.
avium complex
in specimens from patients infected with both M.
avium
complex and M. tuberculosis (42).
Immunosuppressed patients who have pulmonary signs
or
symptoms that are ascribed initially to infections
or
conditions other than TB should be evaluated
initially for
coexisting TB. The evaluation for TB should be
repeated if
the patient does not respond to appropriate therapy
for the
presumed cause(s) of the pulmonary abnormalities
(Suppl. 1;
Suppl. 2).
Patients with suspected or confirmed TB should be
reported
immediately to the appropriate public health
department so
that standard procedures for identifying and
evaluating TB
contacts can be initiated.
Initiation of treatment for suspected or confirmed TB
Patients who have confirmed active TB or who are
considered
highly likely to have active TB should be started
promptly on
appropriate treatment in accordance with current
guidelines
(Suppl. 2) (43). In geographic areas or facilities
that have
a high prevalence of MDR-TB, the initial regimen
used may
need to be enhanced while the results of
drug-susceptibility
tests are pending. The decision should be based on
analysis
of surveillance data.
While the patient is in the health-care facility,
anti-TB
drugs should be administered by directly observed
therapy
(DOT), the process by which an HCW observes the
patient
swallowing the medications. Continuing DOT after
the patient
is discharged should be strongly considered. This
decision
and the arrangements for providing outpatient DOT
should be
made in collaboration with the public health
department.
Management of Patients Who May Have Active TB in
Ambulatory-Care
Settings and Emergency Departments
Triage of patients in ambulatory-care settings and
emergency
departments should include vigorous efforts to promptly
identify
patients who have active TB. HCWs who are the first
points of
contact in facilities that serve populations at risk
for TB
should be trained to ask questions that will facilitate
identi-
fication of patients with signs and symptoms suggestive
of TB.
Patients with signs or symptoms suggestive of TB should
be
evaluated promptly to minimize the amount of time they
are in
ambulatory-care areas. TB precautions should be
followed while
the diagnostic evaluation is being conducted for these
patients.
TB precautions in the ambulatory-care setting should
include a)
placing these patients in a separate area apart from
other
patients, and not in open waiting areas (ideally, in a
room or
enclosure meeting TB isolation requirements); b) giving
these
patients surgical masks **** to wear and instructing
them to keep
their masks on; and c) giving these patients tissues
and
instructing them to cover their mouths and noses with
the tissues
when coughing or sneezing.
TB precautions should be followed for patients who are
known to
have active TB and who have not completed therapy until
a
determination has been made that they are noninfectious
(Suppl.
1).
Patients with active TB who need to attend a
health-care clinic
should have appointments scheduled to avoid exposing
HIV-infected
or otherwise severely immunocompromised persons to M.
tubercu-
losis. This recommendation could be accomplished by
designating
certain times of the day for appointments for these
patients or
by treating them in areas where immunocompromised
persons are not
treated.
Ventilation in ambulatory-care areas where patients at
high risk
for TB are treated should be designed and maintained to
reduce
the risk for transmission of M. tuberculosis.
General-use areas
(e.g., waiting rooms) and special areas (e.g.,
treatment or TB
isolation rooms in ambulatory areas) should be
ventilated in the
same manner as described for similar inpatient areas
(Sections
II.E.3, II.F; Suppl. 3). Enhanced general ventilation
or the use
of air-disinfection techniques (e.g., UVGI or
recirculation of
air within the room through high-efficiency particulate
air
{HEPA} filters) may be useful in general-use areas of
facilities
where many infectious TB patients receive care (Section
II.F;
Suppl. 3).
Ideally, ambulatory-care settings in which patients
with TB are
frequently examined or treated should have a TB
isolation room(s)
available. Such rooms are not necessary in
ambulatory-care
settings in which patients who have confirmed or
suspected TB are
seen infrequently. However, these facilities should
have a
written protocol for early identification of patients
with TB
symptoms and referral to an area or a collaborating
facility
where the patient can be evaluated and managed
appropriately.
These protocols should be reviewed on a regular basis
and revised
as necessary. The additional guidelines in Section II.H
should be
followed in ambulatory-care settings where
cough-inducing
procedures are performed on patients who may have
active TB.
Management of Hospitalized Patients Who Have Confirmed or
Suspected
TB
Initiation of isolation for TB
In hospitals and other inpatient facilities, any
patient
suspected of having or known to have infectious TB
should be
placed in a TB isolation room that has currently
recommended
ventilation characteristics (Section II.E.3; Suppl.
3).
Written policies for initiating isolation should
specify a)
the indications for isolation, b) the person(s)
authorized to
initiate and discontinue isolation, c) the
isolation
practices to follow, d) the monitoring of
isolation, e) the
management of patients who do not adhere to
isolation
practices, and f) the criteria for discontinuing
isolation.
In rare circumstances, placing more than one TB
patient
together in the same room may be acceptable. This
practice is
sometimes referred to as "cohorting." Because of
the risk for
patients becoming superinfected with drug-resistant
organisms, patients with TB should be placed in the
same room
only if all patients involved a) have
culture-confirmed TB,
b) have drug-susceptibility test results available
on a
current specimen obtained during the present
hospitalization,
c) have identical drug-susceptibility patterns on
these
specimens, and d) are on effective therapy. Having
isolates
with identical DNA fingerprint patterns is not
adequate
evidence for placing two TB patients together in
the same
room, because isolates with the same DNA
fingerprint pattern
can have different drug-susceptibility patterns.
Pediatric patients with suspected or confirmed TB
should be
evaluated for potential infectiousness according to
the same
criteria as are adults (i.e., on the basis of
symptoms,
sputum AFB smears, radiologic findings, and other
criteria)
(Suppl. 1). Children who may be infectious should
be placed
in isolation until they are determined to be
noninfectious.
Pediatric patients who may be infectious include
those who
have laryngeal or extensive pulmonary involvement,
pronounced
cough, positive sputum AFB smears, or cavitary TB
or those
for whom cough-inducing procedures are performed
(44).
The source of infection for a child with TB is
often a member
of the child's family (45). Therefore, parents and
other
visitors of all pediatric TB patients should be
evaluated for
TB as soon as possible. Until they have been
evaluated, or
the source case is identified, they should wear
surgical
masks when in areas of the facility outside of the
child's
room, and they should refrain from visiting common
areas in
the facility (e.g., the cafeteria or lounge areas).
TB patients in intensive-care units should be
treated the
same as patients in noncritical-care settings. They
should be
placed in TB isolation and have respiratory
secretions
submitted for AFB smear and culture if they have
undiagnosed
pulmonary symptoms suggestive of TB.
If readmitted to a health-care facility, patients
who are
known to have active TB and who have not completed
therapy
should have TB precautions applied until a
determination has
been made that they are noninfectious (Suppl. 1).
TB isolation practices
Patients who are placed in TB isolation should be
educated
about the mechanisms of M. tuberculosis
transmission and the
reasons for their being placed in isolation. They
should be
taught to cover their mouths and noses with a
tissue when
coughing or sneezing, even while in the isolation
room, to
contain liquid drops and droplets before they are
expelled
into the air (46).
Efforts should be made to facilitate patient
adherence to
isolation measures (e.g., staying in the TB
isolation room).
Such efforts might include the use of incentives
(e.g.,
providing them with telephones, televisions, or
radios in
their rooms or allowing special dietary requests).
Efforts
should also be made to address other problems that
could
interfere with adherence to isolation (e.g.,
management of
the patient's withdrawal from addictive substances
{including
tobacco}).
Patients placed in isolation should remain in their
isolation
rooms with the door closed. If possible, diagnostic
and
treatment procedures should be performed in the
isolation
rooms to avoid transporting patients through other
areas of
the facility. If patients who may have infectious
TB must be
transported outside their isolation rooms for
medically
essential procedures that cannot be performed in
the
isolation rooms, they should wear surgical masks
that cover
their mouths and noses during transport. Persons
transporting
the patients do not need to wear respiratory
protection
outside the TB isolation rooms. Procedures for
these patients
should be scheduled at times when they can be
performed
rapidly and when waiting areas are less crowded.
Treatment and procedure rooms in which patients who
have
infectious TB or who have an undiagnosed pulmonary
disease
and are at high risk for active TB receive care
should meet
the ventilation recommendations for isolation rooms
(Section
II.E.3; Suppl. 3). Ideally, facilities in which TB
patients
are frequently treated should have an area in the
radiology
department that is ventilated separately for TB
patients. If
this is not possible, TB patients should wear
surgical masks
and should stay in the radiology suite the minimum
amount of
time possible, then be returned promptly to their
isolation
rooms.
The number of persons entering an isolation room
should be
minimal. All persons who enter an isolation room
should wear
respiratory protection (Section II.G; Suppl. 4).
The
patient's visitors should be given respirators to
wear while
in the isolation room, and they should be given
general
instructions on how to use their respirators.
Disposable items contaminated with respiratory
secretions are
not associated with transmission of M.
tuberculosis. However,
for general infection-control purposes, these items
should be
handled and transported in a manner that reduces
the risk for
transmitting other microorganisms to patients,
HCWs, and
visitors and that decreases environmental
contamination in
the health-care facility. Such items should be
disposed of in
accordance with hospital policy and applicable
regulations
(Suppl. 5).
The TB isolation room
TB isolation rooms should be single-patient rooms
with
special ventilation characteristics appropriate for
the
purposes of isolation (Suppl. 3). The primary
purposes of TB
isolation rooms are to a) separate patients who are
likely to
have infectious TB from other persons; b) provide
an environ-
ment that will allow reduction of the concentration
of
droplet nuclei through various engineering methods;
and c)
prevent the escape of droplet nuclei from the TB
isolation
room and treatment room, thus preventing entry of
M. tuber-
culosis into the corridor and other areas of the
facility.
To prevent the escape of droplet nuclei, the TB
isolation
room should be maintained under negative pressure
(Suppl. 3).
Doors to isolation rooms should be kept closed,
except when
patients or personnel must enter or exit the room,
so that
negative pressure can be maintained.
Negative pressure in the room should be monitored
daily while
the room is being used for TB isolation.
The American Society of Heating, Refrigerating and
Air-
Conditioning Engineers, Inc. (ASHRAE) (47), the
American
Institute of Architects (AIA) (48), and the Health
Resources
and Services Administration (49) recommend a
minimum of 6 air
changes per hour (ACH) for TB isolation and
treatment rooms.
This ventilation rate is based on comfort and odor
control
considerations. The effectiveness of this level of
airflow in
reducing the concentration of droplet nuclei in the
room,
thus reducing the transmission of airborne
pathogens, has not
been evaluated directly or adequately.
Ventilation rates of greater than 6 ACH are likely
to produce
an incrementally greater reduction in the
concentration of
bacteria in a room than are lower rates (50-52).
However,
accurate quantitation of decreases in risk that
would result
from specific increases in general ventilation
levels has not
been performed and may not be possible.
For the purposes of reducing the concentration of
droplet
nuclei, TB isolation and treatment rooms in
existing health-
care facilities should have an airflow of greater
than or
equal to 6 ACH. Where feasible, this airflow rate
should be
increased to greater than or equal to 12 ACH by
adjusting or
modifying the ventilation system or by using
auxiliary means
(e.g., recirculation of air through fixed HEPA
filtration
systems or portable air cleaners) (Suppl. 3,
Section
II.B.5.a) (53). New construction or renovation of
existing
health-care facilities should be designed so that
TB
isolation rooms achieve an airflow of greater than
or equal
to 12 ACH.
Air from TB isolation rooms and treatment rooms
used to treat
patients who have known or suspected infectious TB
should be
exhausted to the outside in accordance with
applicable
federal, state, and local regulations. The air
should not be
recirculated into the general ventilation. In some
instances,
recirculation of air into the general ventilation
system from
such rooms is unavoidable (i.e., in existing
facilities in
which the ventilation system or facility
configuration makes
venting the exhaust to the outside impossible). In
such
cases, HEPA filters should be installed in the
exhaust duct
leading from the room to the general ventilation
system to
remove infectious organisms and particulates the
size of
droplet nuclei from the air before it is returned
to the
general ventilation system (Section II.F; Suppl.
3). Air from
TB isolation and treatment rooms in new or
renovated
facilities should not be recirculated into the
general
ventilation system.
Although not required, an anteroom may increase the
effec-
tiveness of the isolation room by minimizing the
potential
escape of droplet nuclei into the corridor when the
door is
opened. To work effectively, the anteroom should
have
positive air pressure in relation to the isolation
room. The
pressure relationship between the anteroom and the
corridor
may vary according to ventilation design.
Upper-room air UVGI may be used as an adjunct to
general
ventilation in the isolation room (Section II.F;
Suppl. 3).
Air in the isolation room may be recirculated
within the room
through HEPA filters or UVGI devices to increase
the
effective ACH and to increase thermal efficiency.
Health-care facilities should have enough isolation
rooms to
appropriately isolate all patients who have
suspected or
confirmed active TB. This number should be
estimated using
the results of the risk assessment of the
health-care
facility. Except for minimal- and very low-risk
health-care
facilities, all acute-care inpatient facilities
should have
at least one TB isolation room (Section II.B).
Grouping isolation rooms together in one area of
the facility
may reduce the possibility of transmitting M.
tuberculosis to
other patients and may facilitate care of TB
patients and the
installation and maintenance of optimal engineering
(parti-
cularly ventilation) controls.
Discontinuation of TB isolation
TB isolation can be discontinued if the diagnosis
of TB is
ruled out. For some patients, TB can be ruled out
when
another diagnosis is confirmed. If a diagnosis of
TB cannot
be ruled out, the patient should remain in
isolation until a
determination has been made that the patient is
noninfec-
tious. However, patients can be discharged from the
health-
care facility while still potentially infectious if
appro-
priate postdischarge arrangements can be ensured
(Section
II.E.5).
The length of time required for a TB patient to
become
noninfectious after starting anti-TB therapy varies
consid-
erably (Suppl. 1). Isolation should be discontinued
only when
the patient is on effective therapy, is improving
clinically,
and has had three consecutive negative sputum AFB
smears
collected on different days.
Hospitalized patients who have active TB should be
monitored
for relapse by having sputum AFB smears examined
regularly
(e.g., every 2 weeks). Nonadherence to therapy
(i.e., failure
to take medications as prescribed) and the presence
of drug-
resistant organisms are the two most common reasons
why
patients remain infectious despite treatment. These
reasons
should be considered if a patient does not respond
clinically
to therapy within 2-3 weeks.
Continued isolation throughout the hospitalization
should be
strongly considered for patients who have MDR-TB
because of
the tendency for treatment failure or relapse
(i.e.,
difficulty in maintaining noninfectiousness) that
has been
observed in such cases.
Discharge planning
Before a TB patient is discharged from the
health-care
facility, the facility's staff and public health
authorities
should collaborate to ensure continuation of
therapy.
Discharge planning in the health-care facility
should
include, at a minimum, a) a confirmed outpatient
appointment
with the provider who will manage the patient until
the
patient is cured, b) sufficient medication to take
until the
outpatient appointment, and c) placement into case
management
(e.g., DOT) or outreach programs of the public
health
department. These plans should be initiated and in
place
before the patient's discharge.
Patients who may be infectious at the time of
discharge
should only be discharged to facilities that have
isolation
capability or to their homes. Plans for discharging
a patient
who will return home must consider whether all the
household
members were infected previously and whether any
uninfected
household members are at very high risk for active
TB if
infected (e.g., children less than 4 years of age
or persons
infected with HIV or otherwise severely
immunocompromised).
If the household does include such persons,
arrangements
should be made to prevent them from being exposed
to the TB
patient until a determination has been made that
the patient
is noninfectious.
Engineering Control Recommendations
General ventilation
This section deals only with engineering controls for
general-use
areas of health-care facilities (e.g., waiting-room
areas and
emergency departments). Recommendations for engineering
controls
for specific areas of the facility (e.g., TB isolation
rooms) are
contained in the sections encompassing those areas.
Details
regarding ventilation design, evaluation, and
supplemental
approaches are described in Supplement 3.
Health-care facilities should either a) include as
part of
their staff an engineer or other professional with
expertise
in ventilation or b) have this expertise available
from a
consultant who is an expert in ventilation
engineering and
who also has hospital experience. These persons
should work
closely with infection-control staff to assist in
controlling
airborne infections.
Ventilation system designs in health-care
facilities should
meet any applicable federal, state, and local
requirements.
The direction of airflow in health-care facilities
should be
designed, constructed, and maintained so that air
flows from
clean areas to less-clean areas.
Health-care facilities serving populations that
have a high
prevalence of TB may need to supplement the general
ventil-
ation or use additional engineering approaches
(i.e., HEPA
filtration or UVGI) in general-use areas where TB
patients
are likely to go (e.g., waiting-room areas,
emergency depart-
ments, and radiology suites). A single-pass,
nonrecirculating
system that exhausts air to the outside, a
recirculation
system that passes air through HEPA filters before
recir-
culating it to the general ventilation system, or
upper air
UVGI may be used in such areas.
Additional engineering control approaches
HEPA filtration
HEPA filters may be used in a number of ways to
reduce or
eliminate infectious droplet nuclei from room air
or exhaust
(Suppl. 3). These methods include placement of HEPA
filters
in exhaust ducts discharging air from booths or
enclosures
into the surrounding room; b) in ducts or in
ceiling- or
wall-mounted units, for recirculation of air within
an
individual room (fixed recirculation systems); c)
in portable
air cleaners; d) in exhaust ducts to remove droplet
nuclei
from air being discharged to the outside, either
directly or
through ventilation equipment; and e) in ducts
discharging
air from the TB isolation room into the general
ventilation
system. In any application, HEPA filters should be
installed
carefully and maintained meticulously to ensure
adequate
functioning.
The manufacturers of in-room air cleaning equipment
should
provide documentation of the HEPA filter efficiency
and the
efficiency of the device in lowering room air
contaminant
levels.
UVGI
For general-use areas in which the risk for
transmission of
M. tuberculosis is relatively high, UVGI lamps may
be used as
an adjunct to ventilation for reducing the
concentration of
infectious droplet nuclei (Suppl. 3), although the
effective-
ness of such units has not been evaluated
adequately. Ultra-
violet (UV) units can be installed in a room or
corridor to
irradiate the air in the upper portion of the room
(i.e.,
upper-room air irradiation), or they can be
installed in
ducts to irradiate air passing through the ducts.
UV units
installed in ducts should not be substituted for
HEPA filters
in ducts that discharge air from TB isolation rooms
into the
general ventilation system. However, UV units can
be used in
ducts that recirculate air back into the same room.
To function properly and decrease hazards to HCWs
and others
in the health-care facility, UV lamps should be
installed
properly and maintained adequately, which includes
the
monitoring of irradiance levels. UV tubes should be
changed
according to the manufacturer's instructions or
when meter
readings indicate tube failure. An employee trained
in the
use and handling of UV lamps should be responsible
for these
measures and for keeping maintenance records.
Applicable
safety guidelines should be followed. Caution
should be
exercised to protect HCWs, patients, visitors, and
others
from excessive exposure to UV radiation.
Respiratory Protection
Personal respiratory protection should be used by a)
persons
entering rooms in which patients with known or
suspected
infectious TB are being isolated, b) persons present
during
cough-inducing or aerosol-generating procedures
performed on such
patients, and c) persons in other settings where
administrative
and engineering controls are not likely to protect them
from
inhaling infectious airborne droplet nuclei (Suppl. 4).
These
other settings include transporting patients who may
have
infectious TB in emergency transport vehicles and
providing
urgent surgical or dental care to patients who may have
infectious TB before a determination has been made that
the
patient is noninfectious (Suppl. 1).
Respiratory protective devices used in health-care
settings for
protection against M. tuberculosis should meet the
following
standard performance criteria:
The ability to filter particles 1 um in size in the
unloaded
***** state with a filter efficiency of greater than or
equal to
95% (i.e., filter leakage of less than or equal to 5%),
given
flow rates of up to 50 L per minute.
The ability to be qualitatively or quantitatively
fit tested
in a reliable way to obtain a face-seal leakage of less
than or
equal to 10% (54,55).
The ability to fit the different facial sizes and
character-
istics of HCWs, which can usually be met by making the
respirators available in at least three sizes.
The ability to be checked for facepiece fit, in
accordance
with standards established by the Occupational Safety
and Health
Administration (OSHA) and good industrial hygiene
practice, by
HCWs each time they put on their respirators (54,55).
The facility's risk assessment may identify a limited
number of
selected settings (e.g., bronchoscopy performed on
patients
suspected of having TB or autopsy performed on deceased
persons
suspected of having had active TB at the time of death)
where the
estimated risk for transmission of M. tuberculosis may
be such
that a level of respiratory protection exceeding the
standard
performance criteria is appropriate. In such
circumstances, a
level of respiratory protection exceeding the standard
criteria
and compatible with patient-care delivery (e.g., more
protective
negative-pressure respirators; powered air-purifying
particulate
respirators {PAPRs}; or positive-pressure air-line,
half-mask
respirators) should be provided by employers to HCWs
who are
exposed to M. tuberculosis. Information on these and
other
respirators is in the NIOSH Guide to Industrial
Respiratory
Protection (55) and in Supplement 4 of this document.
In some settings, HCWs may be at risk for two types of
exposure:
inhalation of M. tuberculosis and b) mucous membrane
exposure
to fluids that may contain bloodborne pathogens. In
these
settings, protection against both types of exposure
should be
used.
When operative procedures (or other procedures
requiring a
sterile field) are performed on patients who may have
infectious
TB, respiratory protection worn by the HCW should serve
two
functions: a) it should protect the surgical field from
the
respiratory secretions of the HCW, and b) it should
protect the
HCW from infectious droplet nuclei that may be expelled
by the
patient or generated by the procedure. Respirators with
exhalation valves and most positive-pressure
respirators do not
protect the sterile field.
Health-care facilities in which respiratory protection
is used to
prevent inhalation of M. tuberculosis are required by
OSHA to
develop, implement, and maintain a respiratory
protection program
(Suppl. 4). All HCWs who use respiratory protection
should be
included in this program. Visitors to TB patients
should be given
respirators to wear while in isolation rooms, and they
should be
given general instructions on how to use their
respirators.
Facilities that do not have isolation rooms and do not
perform
cough-inducing procedures on patients who may have TB
may not
need to have a respiratory protection program for TB.
However,
such facilities should have written protocols for the
early
identification of patients who have signs or symptoms
of TB and
procedures for referring these patients to a facility
where they
can be evaluated and managed appropriately. These
protocols
should be evaluated regularly and revised as needed.
Surgical masks are designed to prevent the respiratory
secretions
of the person wearing the mask from entering the air.
To reduce
the expulsion of droplet nuclei into the air, patients
suspected
of having TB should wear surgical masks when not in TB
isolation
rooms. These patients do not need to wear particulate
respir-
ators, which are designed to filter the air before it
is inhaled
by the person wearing the respirator. Patients
suspected of
having or known to have TB should never wear a
respirator that
has an exhalation valve, because this type of
respirator does not
prevent expulsion of droplet nuclei into the air.
Cough-Inducing and Aerosol-Generating Procedures
General guidelines
Procedures that involve instrumentation of the lower
respiratory
tract or induce coughing can increase the likelihood of
droplet
nuclei being expelled into the air. These
cough-inducing
procedures include endotracheal intubation and
suctioning,
diagnostic sputum induction, aerosol treatments (e.g.,
penta-
midine therapy), and bronchoscopy. Other procedures
that can
generate aerosols (e.g., irrigation of tuberculous
abscesses,
homogenizing or lyophilizing tissue, or other
processing of
tissue that may contain tubercle bacilli) are also
covered by
these recommendations.
Cough-inducing procedures should not be performed
on patients
who may have infectious TB unless the procedures
are
absolutely necessary and can be performed with
appropriate
precautions.
All cough-inducing procedures performed on patients
who may
have infectious TB should be performed using local
exhaust
ventilation devices (e.g., booths or special
enclosures) or,
if this is not feasible, in a room that meets the
ventilation
requirements for TB isolation.
HCWs should wear respiratory protection when
present in rooms
or enclosures in which cough-inducing procedures
are being
performed on patients who may have infectious TB.
After completion of cough-inducing procedures,
patients who
may have infectious TB should remain in their
isolation rooms
or enclosures and not return to common waiting
areas until
coughing subsides. They should be given tissues and
instructed to cover their mouths and noses with the
tissues
when coughing. If TB patients must recover from
sedatives or
anesthesia after a procedure (e.g, after a
bronchoscopy),
they should be placed in separate isolation rooms
(and not in
recovery rooms with other patients) while they are
being
monitored.
Before the booth, enclosure, or room is used for
another
patient, enough time should be allowed to pass for
at least
99% of airborne contaminants to be removed. This
time will
vary according to the efficiency of the ventilation
or
filtration used (Suppl. 3, Table_S31).
Special considerations for bronchoscopy
If performing bronchoscopy in positive-pressure
rooms (e.g.,
operating rooms) is unavoidable, TB should be ruled
out as a
diagnosis before the procedure is performed. If the
broncho-
scopy is being performed for the purpose of
diagnosing
pulmonary disease and that diagnosis could include
TB, the
procedure should be performed in a room that meets
TB
isolation ventilation requirements.
Special considerations for the administration of
aerosolized
pentamidine
Patients should be screened for active TB before
prophylactic
therapy with aerosolized pentamidine is initiated.
Screening
should include obtaining a medical history and
performing
skin testing and chest radiography.
Before each subsequent treatment with aerosolized
penta-
midine, patients should be screened for symptoms
suggestive
of TB (e.g., development of a productive cough). If
such
symptoms are elicited, a diagnostic evaluation for
TB should
be initiated.
Patients who have suspected or confirmed active TB
should
take, if clinically practical, oral prophylaxis for
P.
carinii pneumonia.
Education and Training of HCWs
All HCWs, including physicians, should receive education
regarding TB
that is relevant to persons in their particular
occupational group.
Ideally, training should be conducted before initial
assignment, and
the need for additional training should be reevaluated
periodically
(e.g., once a year). The level and detail of this education
will vary
according to the HCW's work responsibilities and the level
of risk in
the facility (or area of the facility) in which the HCW
works.
However, the program may include the following elements:
The basic concepts of M. tuberculosis transmission,
pathogenesis,
and diagnosis, including information concerning the
difference
between latent TB infection and active TB disease, the
signs and
symptoms of TB, and the possibility of reinfection.
The potential for occupational exposure to persons who
have
infectious TB in the health-care facility, including
information
concerning the prevalence of TB in the community and
facility,
the ability of the facility to properly isolate
patients who have
active TB, and situations with increased risk for
exposure to M.
tuberculosis.
The principles and practices of infection control that
reduce the
risk for transmission of M. tuberculosis, including
information
concerning the hierarchy of TB infection-control
measures and the
written policies and procedures of the facility.
Site-specific
control measures should be provided to HCWs working in
areas that
require control measures in addition to those of the
basic TB
infection-control program.
The purpose of PPD skin testing, the significance of a
positive
PPD test result, and the importance of participating in
the skin-
test program.
The principles of preventive therapy for latent TB
infection.
These principles include the indications, use,
effectiveness, and
the potential adverse effects of the drugs (Suppl. 2).
The HCW's responsibility to seek prompt medical
evaluation if a
PPD test conversion occurs or if symptoms develop that
could be
caused by TB. Medical evaluation will enable HCWs who
have TB to
receive appropriate therapy and will help to prevent
transmission
of M. tuberculosis to patients and other HCWs.
The principles of drug therapy for active TB.
The importance of notifying the facility if the HCW is
diagnosed
with active TB so that contact investigation procedures
can be
initiated.
The responsibilities of the facility to maintain the
confiden-
tiality of the HCW while ensuring that the HCW who has
TB
receives appropriate therapy and is noninfectious
before
returning to duty.
The higher risks associated with TB infection in
persons who have
HIV infection or other causes of severely impaired
cell-mediated
immunity, including a) the more frequent and rapid
development of
clinical TB after infection with M. tuberculosis, b)
the
differences in the clinical presentation of disease,
and c) the
high mortality rate associated with MDR-TB in such
persons.
The potential development of cutaneous anergy as immune
function
(as measured by CD4+ T-lymphocyte counts) declines.
Information regarding the efficacy and safety of BCG
vaccination
and the principles of PPD screening among BCG
recipients.
The facility's policy on voluntary work reassignment
options for
immunocompromised HCWs.
HCW Counseling, Screening, and Evaluation
A TB counseling, screening, and prevention program for HCWs
should be
established to protect both HCWs and patients. HCWs who
have positive
PPD test results, PPD test conversions, or symptoms
suggestive of TB
should be identified, evaluated to rule out a diagnosis of
active TB,
and started on therapy or preventive therapy if indicated
(5). In
addition, the results of the HCW PPD screening program will
contribute to evaluation of the effectiveness of current
infection-
control practices.
Counseling HCWs regarding TB
Because of the increased risk for rapid progression
from
latent TB infection to active TB in HIV-infected or
otherwise
severely immunocompromised persons, all HCWs should
know if
they have a medical condition or are receiving a
medical
treatment that may lead to severely impaired
cell-mediated
immunity. HCWs who may be at risk for HIV infection
should
know their HIV status (i.e., they should be
encouraged to
voluntarily seek counseling and testing for HIV
antibody
status). Existing guidelines for counseling and
testing
should be followed routinely (56). Knowledge of
these
conditions allows the HCW to seek the appropriate
preventive
measures outlined in this document and to consider
voluntary
work reassignments. Of particular importance is
that HCWs
need to know their HIV status if they are at risk
for HIV
infection and they work in settings where patients
who have
drug-resistant TB may be encountered.
All HCWs should be informed about the need to
follow existing
recommendations for infection control to minimize
the risk
for exposure to infectious agents; implementation
of these
recommendations will greatly reduce the risk for
occupational
infections among HCWs (57). All HCWs should also be
informed
about the potential risks to severely
immunocompromised
persons associated with caring for patients who
have some
infectious diseases, including TB. It should be
emphasized
that limiting exposure to TB patients is the most
protective
measure that severely immunosuppressed HCWs can
take to avoid
becoming infected with M. tuberculosis. HCWs who
have
severely impaired cell-mediated immunity and who
may be
exposed to M. tuberculosis may consider a change in
job
setting to avoid such exposure. HCWs should be
advised of the
option that severely immunocompromised HCWs can
choose to
transfer voluntarily to areas and work activities
in which
there is the lowest possible risk for exposure to
M. tuber-
culosis. This choice should be a personal decision
for HCWs
after they have been informed of the risks to their
health.
Employers should make reasonable accommodations
(e.g.,
alternative job assignments) for employees who have
a health
condition that compromises cell-mediated immunity
and who
work in settings where they may be exposed to M.
tuber-
culosis. HCWs who are known to be immunocompromised
should be
referred to employee health professionals who can
indivi-
dually counsel the employees regarding their risk
for TB.
Upon the request of the immunocompromised HCW,
employers
should offer, but not compel, a work setting in
which the HCW
would have the lowest possible risk for
occupational exposure
to M. tuberculosis. Evaluation of these situations
should
also include consideration of the provisions of the
Americans
With Disabilities Act of 1990 ****** and other
applicable
federal, state, and local laws.
All HCWs should be informed that immunosuppressed
HCWs should
have appropriate follow-up and screening for
infectious
diseases, including TB, provided by their medical
practi-
tioner. HCWs who are known to be HIV-infected or
otherwise
severely immunosuppressed should be tested for
cutaneous
anergy at the time of PPD testing (Suppl. 2).
Consideration
should be given to retesting, at least every 6
months, those
immunocompromised HCWs who are potentially exposed
to M.
tuberculosis because of the high risk for rapid
progression
to active TB if they become infected.
Information provided by HCWs regarding their immune
status
should be treated confidentially. If the HCW
requests
voluntary job reassignment, the confidentiality of
the HCW
should be maintained. Facilities should have
written
procedures on confidential handling of such
information.
Screening HCWs for active TB
Any HCW who has a persistent cough (i.e., a cough
lasting
greater than or equal to 3 weeks), especially in
the presence
of other signs or symptoms compatible with active
TB (e.g.,
weight loss, night sweats, bloody sputum, anorexia,
or
fever), should be evaluated promptly for TB. The
HCW should
not return to the workplace until a diagnosis of TB
has been
excluded or until the HCW is on therapy and a
determination
has been made that the HCW is noninfectious.
Screening HCWs for latent TB infection
The risk assessment should identify which HCWs have
potential
for exposure to M. tuberculosis and the frequency
with which
the exposure may occur. This information is used to
determine
which HCWs to include in the skin-testing program
and the
frequency with which they should be tested
(Table_2).
If HCWs are from risks groups with increased
prevalence of
TB, consideration may be given to including them in
the skin-
testing program, even if they do not have potential
occupa-
tional exposure to M. tuberculosis, so that
converters can be
identified and preventive therapy offered.
Administrators of health-care facilities should
ensure that
physicians and other personnel not paid by, but
working in,
the facility receive skin testing at appropriate
intervals
for their occupational group and work location.
During the pre-employment physical or when applying
for
hospital privileges, HCWs who have potential for
exposure to
M. tuberculosis (Table_2), including those with
a history
of BCG vaccination, should have baseline PPD skin
testing
performed (Suppl. 2). For HCWs who have not had a
documented
negative PPD test result during the preceding 12
months, the
baseline PPD testing should employ the two-step
method; this
will detect boosting phenomena that might be
misinterpreted
as a skin-test conversion. Decisions concerning the
use of
the two-step procedure for baseline testing in a
particular
facility should be based on the frequency of
boosting in that
facility.
HCWs who have a documented history of a positive
PPD test,
adequate treatment for disease, or adequate
preventive
therapy for infection, should be exempt from
further PPD
screening unless they develop signs or symptoms
suggestive of
TB.
PPD-negative HCWs should undergo repeat PPD testing
at
regular intervals as determined by the risk
assessment
(Section II.B). In addition, these HCWs should be
tested
whenever they have been exposed to a TB patient and
appro-
priate precautions were not observed at the time of
exposure
(Section II.K.3). Performing PPD testing of HCWs
who work in
the same area or occupational group on different
scheduled
dates (e.g., test them on their birthdays or on
their
employment anniversary dates), rather than testing
all HCWs
in the area or group on the same day, may lead to
earlier
detection of M. tuberculosis transmission.
All PPD tests should be administered, read, and
interpreted
in accordance with current guidelines by specified
trained
personnel (Suppl. 2). At the time their test
results are
read, HCWs should be informed about the
interpretation of
both positive and negative PPD test results. This
information
should indicate that the interpretation of an
induration that
is 5-9 mm in diameter depends on the HCW's immune
status and
history of exposure to persons who have infectious
TB. Speci-
fically, HCWs who have indurations of 5-9 mm in
diameter
should be advised that such results may be
considered
positive for HCWs who are contacts of persons with
infectious
TB or who have HIV infection or other causes of
severe
immunosuppression (e.g., immunosuppressive therapy
for organ
transplantation).
When an HCW who is not assigned regularly to a
single work
area has a PPD test conversion, appropriate
personnel should
identify the areas where the HCW worked during the
time when
infection was likely to have occurred. This
information can
then be considered in analyzing the risk for
transmission in
those areas.
In any area of the facility where transmission of
M. tuber-
culosis is known to have occurred, a problem
evaluation
should be conducted (Section II.K), and the
frequency of skin
testing should be determined according to the
applicable risk
category (Section II.B).
PPD test results should be recorded confidentially
in the
individual HCW's employee health record and in an
aggregate
database of all HCW PPD test results. The database
can be
analyzed periodically to estimate the risk for
acquiring new
infection in specific areas or occupational groups
in the
facility.
Evaluation and management of HCWs who have positive PPD
test
results or active TB
Evaluation
All HCWs with newly recognized positive PPD
test results
or PPD test conversions should be evaluated
promptly for
active TB. This evaluation should include a
clinical
examination and a chest radiograph. If the
history,
clinical examination, or chest radiograph is
compatible
with active TB, additional tests should be
performed
(Section II.C.2). If symptoms compatible with
TB are
present, the HCW should be excluded from the
workplace
until either a) a diagnosis of active TB is
ruled out or
b) a diagnosis of active TB was established,
the HCW is
being treated, and a determination has been
made that the
HCW is noninfectious (Suppl. 2). HCWs who do
not have
active TB should be evaluated for preventive
therapy
according to published guidelines (Suppl. 2).
If an HCW's PPD test result converts to
positive, a
history of confirmed or suspected TB exposure
should be
obtained in an attempt to determine the
potential source.
When the source of exposure is known, the
drug-suscepti-
bility pattern of the M. tuberculosis isolated
from the
source should be identified so that the correct
curative
or preventive therapy can be initiated for the
HCW with
the PPD test conversion. The
drug-susceptibility pattern
should be recorded in the HCW's medical record,
where it
will be available if the HCW subsequently
develops active
TB and needs therapy specific for the
drug-susceptibility
pattern.
All HCWs, including those with histories of
positive PPD
test results, should be reminded periodically
about the
symptoms of TB and the need for prompt
evaluation of any
pulmonary symptoms suggestive of TB.
Routine and follow-up chest radiographs
Routine chest radiographs are not required for
asympto-
matic, PPD-negative HCWs. HCWs with positive
PPD test
results should have a chest radiograph as part
of the
initial evaluation of their PPD test; if
negative, repeat
chest radiographs are not needed unless
symptoms develop
that could be attributed to TB (58). However,
more
frequent monitoring for symptoms of TB may be
considered
for recent converters and other PPD-positive
HCWs who are
at increased risk for developing active TB
(e.g., HIV-
infected or otherwise severely
immunocompromised HCWs).
Workplace restrictions
Active TB
HCWs with pulmonary or laryngeal TB pose a
risk to
patients and other HCWs while they are
infectious,
and they should be excluded from the
workplace until
they are noninfectious. The same work
restrictions
apply to all HCWs regardless of their
immune status.
Before the HCW who has TB can return to the
work-
place, the health-care facility should have
docu-
mentation from the HCW's health-care
provider that
the HCW is receiving adequate therapy, the
cough has
resolved, and the HCW has had three
consecutive
negative sputum smears collected on
different days.
After work duties are resumed and while the
HCW
remains on anti-TB therapy, facility staff
should
receive periodic documentation from the
HCW's
health-care provider that the HCW is being
maintained on effective drug therapy for
the
recommended time period and that the sputum
AFB
smears continue to be negative.
HCWs with active laryngeal or pulmonary TB
who
discontinue treatment before they are cured
should
be evaluated promptly for infectiousness.
If the
evaluation determines that they are still
infec-
tious, they should be excluded from the
workplace
until treatment has been resumed, an
adequate
response to therapy has been documented,
and three
more consecutive sputum AFB smears
collected on
different days have been negative.
HCWs who have TB at sites other than the
lung or
larynx usually do not need to be excluded
from the
workplace if a diagnosis of concurrent
pulmonary TB
has been ruled out.
Latent TB infection
HCWs receiving preventive treatment for
latent TB
infection should not be restricted from
their usual
work activities.
HCWs with latent TB infection who cannot
take or who
do not accept or complete a full course of
preven-
tive therapy should not be excluded from
the work-
place. These HCWs should be counseled about
the risk
for developing active TB and instructed
regularly to
seek prompt evaluation if signs or symptoms
develop
that could be caused by TB.
Problem Evaluation
Epidemiologic investigations may be indicated for several
situations.
These include, but are not limited to, a) the occurrence of
PPD test
conversions or active TB in HCWs; b) the occurrence of
possible
person-to-person transmission of M. tuberculosis; and c)
situations
in which patients or HCWs with active TB are not promptly
identified
and isolated, thus exposing other persons in the facility
to M.
tuberculosis. The general objectives of the epidemiologic
investi-
gations in these situations are as follows:
to determine the likelihood that transmission of and
infection
with M. tuberculosis has occurred in the facility;
to determine the extent to which M. tuberculosis has
been
transmitted;
to identify those persons who have been exposed and
infected,
enabling them to receive appropriate clinical
management;
to identify factors that could have contributed to
trans-
mission and infection and to implement appropriate
interventions;
and
to evaluate the effectiveness of any interventions
that are
implemented and to ensure that exposure to and
transmission of M.
tuberculosis have been terminated.
The exact circumstances of these situations are likely to
vary
considerably, and the associated epidemiologic
investigations should
be tailored to the individual circumstances. The following
sections
provide general guidance for conducting these
investigations.
Investigating PPD test conversions and active TB in
HCWs
Investigating PPD test conversions in HCWs
PPD test conversions may be detected in HCWs as a
result of
a contact investigation, in which case the probable
source of
exposure and transmission is already known (Section
II.K.3.),
or as a result of routine screening, in which case
the
probable source of exposure and infection is not
already
known and may not be immediately apparent.
If a skin-test conversion in an HCW is identified
as part of
routine screening, the following steps should be
considered
(Figure_2Figure_2c):
The HCW should be evaluated promptly for active
TB. The
initial evaluation should include a thorough
history,
physical examination, and chest radiograph. On
the basis
of the initial evaluation, other diagnostic
procedures
(e.g., sputum examination) may be indicated.
If appropriate, the HCW should be placed on
preventive or
curative therapy in accordance with current
guidelines
(Suppl. 2) (5).
A history of possible exposure to M.
tuberculosis should
be obtained from the HCW to determine the most
likely
source of infection. When the source of
infection is
known, the drug-susceptibility pattern of the
M. tuber-
culosis isolate from the source patient should
be
identified to determine appropriate preventive
or
curative therapy regimens.
If the history suggests that the HCW was
exposed to and
infected with M. tuberculosis outside the
facility, no
further epidemiologic investigation to identify
a source
in the facility is necessary.
If the history does not suggest that the HCW
was exposed
and infected outside the facility but does
identify a
probable source of exposure in the facility,
contacts of
the suspected source patient should be
identified and
evaluated. Possible reasons for the exposure
and trans-
mission should be evaluated (Table_4),
interventions
should be implemented to correct these causes,
and PPD
testing of PPD-negative HCWs should be
performed
immediately and repeated after 3 months.
If no additional PPD test conversions are
detected on
follow-up testing, the investigation can be
terminated.
If additional PPD test conversions are detected
on
follow-up testing, the possible reasons for
exposure and
transmission should be reassessed, the
appropriateness of
and degree of adherence to the interventions
implemented
should be evaluated, and PPD testing of
PPD-negative HCWs
should be repeated after another 3 months.
If no additional PPD test conversions are
detected on the
second round of follow-up testing, the
investigation can
be terminated. However, if additional PPD
conversions are
detected on the second round of follow-up
testing, a
high-risk protocol should be implemented in the
affected
area or occupational group, and the public
health
department or other persons with expertise in
TB
infection control should be consulted.
If the history does not suggest that the HCW
was exposed
to and infected with M. tuberculosis outside
the facility
and does not identify a probable source of
exposure in
the facility, further investigation to identify
the
probable source patient in the facility is
warranted.
The interval during which the HCW could have
been
infected should be estimated. Generally, this
would be
the interval from 10 weeks before the most
recent
negative PPD test through 2 weeks before the
first
positive PPD test (i.e., the conversion).
Laboratory and infection-control records should
be
reviewed to identify all patients or HCWs who
have
suspected or confirmed infectious TB and who
could have
transmitted M. tuberculosis to the HCW.
If this process does identify a likely source
patient,
contacts of the suspected source patient should
be
identified and evaluated, and possible reasons
for the
exposure and transmission should be evaluated
(Table_4). Interventions should be
implemented to
correct these causes, and PPD testing of
PPD-negative
HCWs should be repeated after 3 months.
However, if this
process does not identify a probable source
case, PPD
screening results of other HCWs in the same
area or
occupational group should be reviewed for
additional
evidence of M. tuberculosis transmission. If
sufficient
additional PPD screening results are not
available,
appropriate personnel should consider
conducting
additional PPD screening of other HCWs in the
same area
or occupational group.
If this review and/or screening does not
identify
additional PPD conversions, nosocomial
transmission is
less likely, and the contact investigation can
probably
be terminated. Whether the HCW's PPD test
conversion
resulted from occupational exposure and
infection is
uncertain; however, the absence of other data
implicating
nosocomial transmission suggests that the
conversion
could have resulted from a) unrecognized
exposure to M.
tuberculosis outside the facility; b)
cross-reactivity
with another antigen (e.g., nontuberculous
mycobacteria);
c) errors in applying, reading, or interpreting
the test;
d) false positivity caused by the normal
variability of
the test; or e) false positivity caused by a
defective
PPD preparation.
If this review and/or screening does identify
additional
PPD test conversions, nosocomial transmission
is more
likely. In this situation, the patient
identification
(i.e., triage) process, TB infection-control
policies and
practices, and engineering controls should be
evaluated
to identify problems that could have led to
exposure and
transmission (Table_4).
If no such problems are identified, a high-risk
protocol
should be implemented in the affected area or
occupa-
tional group, and the public health department
or other
persons with expertise in TB infection control
should be
consulted.
If such problems are identified, appropriate
interven-
tions should be implemented to correct the
problem(s),
and PPD skin testing of PPD-negative HCWs
should be
repeated after 3 months.
If no additional PPD conversions are detected
on follow-
up testing, the investigation can be
terminated.
If additional PPD conversions are detected on
follow-up
testing, the possible reasons for exposure and
trans-
mission should be reassessed, the
appropriateness of and
adherence to the interventions implemented
should be
evaluated, and PPD skin testing of PPD-negative
HCWs
should be repeated after another 3 months.
If no additional PPD test conversions are
detected on
this second round of follow-up testing, the
investigation
can be terminated. However, if additional PPD
test
conversions are detected on the second round of
follow-up
testing, a high-risk protocol should be
implemented in
the affected area or occupational group, and
the public
health department or other persons with
expertise in TB
infection control should be consulted.
Investigating cases of active TB in HCWs
If an HCW develops active TB, the following steps
should be
taken:
The case should be evaluated epidemiologically,
in a
manner similar to PPD test conversions in HCWs,
to
determine the likelihood that it resulted from
occupational transmission and to identify
possible causes
and implement appropriate interventions if the
evaluation
suggests such transmission.
Contacts of the HCW (e.g., other HCWs,
patients,
visitors, and others who have had intense
exposure to the
HCW) should be identified and evaluated for TB
infection
and disease (Section II.K.3; Suppl. 2). The
public health
department should be notified immediately for
consul-
tation and to allow for investigation of
community
contacts who were not exposed in the
health-care
facility.
The public health department should notify
facilities
when HCWs with TB are reported by physicians so
that an
investigation of contacts can be conducted in
the
facility. The information provided by the
health depart-
ment to facilities should be in accordance with
state or
local laws to protect the confidentiality of
the HCW.
Investigating possible patient-to-patient transmission
of M.
tuberculosis
Surveillance of active TB cases in patients should be
conducted.
If this surveillance suggests the possibility of
patient-to-
patient transmission of M. tuberculosis (e.g., a high
proportion
of TB patients had prior admissions during the year
preceding
onset of their TB, the number of patients with
drug-resistant TB
increased suddenly, or isolates obtained from multiple
patients
had identical and characteristic drug-susceptibility or
DNA
fingerprint patterns), the following steps should be
taken:
Review the HCW PPD test results and patient
surveillance data
for the suspected areas to detect additional
patients or HCWs
with PPD test conversions or active disease.
Look for possible exposures that patients with
newly
diagnosed TB could have had to other TB patients
during
previous admissions. For example, were the patients
admitted
to the same room or area, or did they receive the
same
procedure or go to the same treatment area on the
same day?
If the evaluation thus far suggests transmission has
occurred,
the following steps should be taken:
Evaluate possible causes of the transmission (e.g.,
problem
with patient detection, institutional barriers to
imple-
menting appropriate isolation practices, or
inadequate
engineering controls) (Table_4).
Ascertain whether other patients or HCWs could have
been
exposed; if so, evaluate these persons for TB
infection and
disease (Section II.K.3; Suppl. 2).
Notify the public health department so they can
begin a
community contact investigation if necessary.
Investigating contacts of patients and HCWs who have
infectious
TB
If a patient who has active TB is examined in a
health-care
facility and the illness is not diagnosed correctly,
resulting in
failure to apply appropriate precautions, or if an HCW
develops
active TB and exposes other persons in the facility,
the
following steps should be taken when the illness is
later
diagnosed correctly:
To identify other patients and HCWs who were
exposed to the
source patient before isolation procedures were
begun,
interview the source patient and all applicable
personnel and
review that patient's medical record. Determine the
areas of
the facility in which the source patient was
hospitalized,
visited, or worked before being placed in isolation
(e.g.,
outpatient clinics, hospital rooms, treatment
rooms,
radiology and procedure areas, and patient lounges)
and the
HCWs who may have been exposed during that time
(e.g.,
persons providing direct care, therapists, clerks,
transpor-
tation personnel, housekeepers, and social
workers).
The contact investigation should first determine if
M.
tuberculosis transmission has occurred from the
source
patient to those persons with whom the source
patient had the
most intense contact.
Administer PPD tests to the most intensely exposed
HCWs and
patients as soon as possible after the exposure has
occurred.
If transmission did occur to the most intensely
exposed
persons, then those persons with whom the patient
had less
contact should be evaluated. If the initial PPD
test result
is negative, a second test should be administered
12 weeks
after the exposure was terminated.
Those persons who were exposed to M. tuberculosis
and who
have either a PPD test conversion or symptoms
suggestive of
TB should receive prompt clinical evaluation and,
if
indicated, chest radiographs and bacteriologic
studies should
be performed (Suppl. 2). Those persons who have
evidence of
newly acquired infection or active disease should
be evalu-
ated for preventive or curative therapy (Suppl. 2).
Persons
who have previously had positive PPD test results
and who
have been exposed to an infectious TB patient do
not require
a repeat PPD test or a chest radiograph unless they
have
symptoms suggestive of TB.
In addition to PPD testing those HCWs and patients
who have
been exposed to M. tuberculosis because a patient
was not
isolated promptly or an HCW with active TB was not
identified
promptly, the investigation should determine why
the diag-
nosis of TB was delayed. If the correct diagnosis
was made
but the patient was not isolated promptly, the
reasons for
the delay need to be defined so that corrective
actions can
be taken.
Coordination with the Public Health Department
As soon as a patient or HCW is known or suspected to
have active
TB, the patient or HCW should be reported to the public
health
department so that appropriate follow-up can be
arranged and a
community contact investigation can be performed. The
health
department should be notified well before patient
discharge to
facilitate follow-up and continuation of therapy. A
discharge
plan coordinated with the patient or HCW, the health
department,
and the inpatient facility should be implemented.
The public health department should protect the
confidentiality
of the patient or HCW in accordance with state and
local laws.
Health-care facilities and health departments should
coordinate
their efforts to perform appropriate contact
investigations on
patients and HCWs who have active TB.
In accordance with state and local laws and
regulations, results
of all AFB-positive sputum smears, cultures positive
for M.
tuberculosis, and drug-susceptibility results on M.
tuberculosis
isolates should be reported to the public health
department as
soon as these results are available.
The public health department may be able to assist
facilities
with planning and implementing various aspects of a TB
infection-
control program (e.g., surveillance, screening
activities, and
outbreak investigations). In addition, the state health
depart-
ment may be able to provide names of experts to assist
with the
engineering aspects of TB infection control.
Additional Considerations for Selected Areas in Health-Care
Facilities and Other Health-Care Settings
This section contains additional information for selected
areas in
health-care facilities and for other health-care settings.
Selected areas in health-care facilities
Operating rooms
Elective operative procedures on patients who
have TB
should be delayed until the patient is no
longer
infectious.
If operative procedures must be performed, they
should be
done, if possible, in operating rooms that have
anterooms. For operating rooms without
anterooms, the
doors to the operating room should be closed,
and traffic
into and out of the room should be minimal to
reduce the
frequency of opening and closing the door.
Attempts
should be made to perform the procedure at a
time when
other patients are not present in the operative
suite and
when a minimum number of personnel are present
(e.g., at
the end of day).
Placing a bacterial filter on the patient
endotracheal
tube (or at the expiratory side of the
breathing circuit
of a ventilator or anesthesia machine if these
are used)
when operating on a patient who has confirmed
or
suspected TB may help reduce the risk for
contaminating
anesthesia equipment or discharging tubercle
bacilli into
the ambient air.
During postoperative recovery, the patient
should be
monitored and should be placed in a private
room that
meets recommended standards for ventilating TB
isolation
rooms.
When operative procedures (or other procedures
requiring
a sterile field) are performed on patients who
may have
infectious TB, respiratory protection worn by
the HCW
must protect the field from the respiratory
secretions of
the HCW and protect the HCW from the infectious
droplet
nuclei generated by the patient. Valved or
positive-
pressure respirators do not protect the sterile
field;
therefore, a respirator that does not have a
valve and
that meets the criteria in Section II.G should
be used.
Autopsy rooms
Because infectious aerosols are likely to be
present in
autopsy rooms, such areas should be at negative
pressure
with respect to adjacent areas (Suppl. 3), and
the room
air should be exhausted directly to the outside
of the
building. ASHRAE recommends that autopsy rooms
have
ventilation that provides an airflow of 12 ACH
(47),
although the effectiveness of this ventilation
level in
reducing the risk for M. tuberculosis
transmission has
not been evaluated. Where possible, this level
should be
increased by means of ventilation system design
or by
auxiliary methods (e.g., recirculation of air
within the
room through HEPA filters) (Suppl. 3).
Respiratory protection should be worn by
personnel while
performing autopsies on deceased persons who
may have had
TB at the time of death (Section II.G; Suppl.
4).
Recirculation of HEPA-filtered air within the
room or
UVGI may be used as a supplement to the
recommended
ventilation (Suppl. 3).
Laboratories
Laboratories in which specimens for
mycobacteriologic
studies (e.g., AFB smears and cultures) are
processed
should be designed to conform with criteria
specified by
CDC and the National Institutes of Health (59).
Other health-care settings
TB precautions may be appropriate in a number of other
types of
health-care settings. The specific precautions that are
applied
will vary depending on the setting. At a minimum, a
risk
assessment should be performed yearly for these
settings; a
written TB infection-control plan should be developed,
evaluated,
and revised on a regular basis; protocols should be in
place for
identifying and managing patients who may have active
TB; HCWs
should receive appropriate training, education, and
screening;
protocols for problem evaluation should be in place;
and coordin-
ation with the public health department should be
arranged when
necessary. Other recommendations specific to certain of
these
settings follow.
Emergency medical services
When EMS personnel or others must transport
patients who
have confirmed or suspected active TB, a
surgical mask
should be placed, if possible, over the
patient's mouth
and nose. Because administrative and
engineering controls
during emergency transport situations cannot be
ensured,
EMS personnel should wear respiratory
protection when
transporting such patients. If feasible, the
windows of
the vehicle should be kept open. The heating
and air-
conditioning system should be set on a
nonrecirculating
cycle.
EMS personnel should be included in a
comprehensive PPD
screening program and should receive a baseline
PPD test
and follow-up testing as indicated by the risk
assess-
ment. They should also be included in the
follow-up of
contacts of a patient with infectious TB.
*******
Hospices
Hospice patients who have confirmed or
suspected TB
should be managed in the manner described in
this
document for management of TB patients in
hospitals.
General-use and specialized areas (e.g.,
treatment or TB
isolation rooms) should be ventilated in the
same manner
as described for similar hospital areas.
Long-term care facilities
Recommendations published previously for
preventing and
controlling TB in long-term care facilities
should be
followed (60).
Long-term care facilities should also follow
the recom-
mendations outlined in this document.
Correctional facilities
Recommendations published previously for
preventing and
controlling TB in correctional facilities
should be
followed (61).
Prison medical facilities should also follow
the recom-
mendations outlined in this document.
Dental settings
In general, the symptoms for which patients seek
treatment in
a dental-care setting are not likely to be caused
by
infectious TB. Unless a patient requiring dental
care
coincidentally has TB, it is unlikely that
infectious TB will
be encountered in the dental setting. Furthermore,
generation
of droplet nuclei containing M. tuberculosis during
dental
procedures has not been demonstrated (62).
Therefore, the
risk for transmission of M. tuberculosis in most
dental
settings is probably quite low. Nevertheless,
during dental
procedures, patients and dental workers share the
same air
for varying periods of time. Coughing may be
stimulated
occasionally by oral manipulations, although no
specific
dental procedures have been classified as
"cough-inducing."
In some instances, the population served by a
dental-care
facility, or the HCWs in the facility, may be at
relatively
high risk for TB. Because the potential exists for
trans-
mission of M. tuberculosis in dental settings, the
following
recommendations should be followed:
A risk assessment (Section II.B) should be done
period-
ically, and TB infection-control policies for
each dental
setting should be based on the risk assessment.
The
policies should include provisions for
detection and
referral of patients who may have undiagnosed
active TB;
management of patients with active TB, relative
to
provision of urgent dental care; and
employer-sponsored
HCW education, counseling, and screening.
While taking patients' initial medical
histories and at
periodic updates, dental HCWs should routinely
ask all
patients whether they have a history of TB
disease and
symptoms suggestive of TB.
Patients with a medical history or symptoms
suggestive of
undiagnosed active TB should be referred
promptly for
medical evaluation of possible infectiousness.
Such
patients should not remain in the dental-care
facility
any longer than required to arrange a referral.
While in
the dental-care facility, they should wear
surgical masks
and should be instructed to cover their mouths
and noses
when coughing or sneezing.
Elective dental treatment should be deferred
until a
physician confirms that the patient does not
have
infectious TB. If the patient is diagnosed as
having
active TB, elective dental treatment should be
deferred
until the patient is no longer infectious.
If urgent dental care must be provided for a
patient who
has, or is strongly suspected of having,
infectious TB,
such care should be provided in facilities that
can
provide TB isolation (Sections II.E and G).
Dental HCWs
should use respiratory protection while
performing
procedures on such patients.
Any dental HCW who has a persistent cough
(i.e., a cough
lasting greater than or equal to 3 weeks),
especially in
the presence of other signs or symptoms
compatible with
active TB (e.g., weight loss, night sweats,
bloody
sputum, anorexia, and fever), should be
evaluated
promptly for TB. The HCW should not return to
the work-
place until a diagnosis of TB has been excluded
or until
the HCW is on therapy and a determination has
been made
that the HCW is noninfectious.
In dental-care facilities that provide care to
popula-
tions at high risk for active TB, it may be
appropriate
to use engineering controls similar to those
used in
general-use areas (e.g., waiting rooms) of
medical
facilities that have a similar risk profile.
Home-health-care settings
HCWs who provide medical services in the homes
of
patients who have suspected or confirmed
infectious TB
should instruct such patients to cover their
mouths and
noses with a tissue when coughing or sneezing.
Until such
patients are no longer infectious, HCWs should
wear
respiratory protection when entering these
patients'
homes (Suppl. 4).
Precautions in the home may be discontinued
when the
patient is no longer infectious (Suppl. 1).
HCWs who provide health-care services in their
patients'
homes can assist in preventing transmission of
M. tuber-
culosis by educating their patients regarding
the impor-
tance of taking medications as prescribed and
by admin-
istering DOT.
Cough-inducing procedures performed on patients
who have
infectious TB should not be done in the
patients' homes
unless absolutely necessary. When medically
necessary
cough-inducing procedures (e.g., AFB sputum
collection
for evaluation of therapy) must be performed on
patients
who may have infectious TB, the procedures
should be
performed in a health-care facility in a room
or booth
that has the recommended ventilation for such
procedures.
If these procedures must be performed in a
patient's
home, they should be performed in a
well-ventilated area
away from other household members. If feasible,
the HCW
should consider opening a window to improve
ventilation
or collecting the specimen while outside the
dwelling.
The HCW collecting these specimens should wear
respir-
atory protection during the procedure (Section
II.G).
HCWs who provide medical services in their
patients'
homes should be included in comprehensive
employer-
sponsored TB training, education, counseling,
and
screening programs. These programs should
include
provisions for identifying HCWs who have active
TB,
baseline PPD skin testing, and follow-up PPD
testing at
intervals appropriate to the degree of risk.
Patients who are at risk for developing active
TB and the
HCWs who provide medical services in the homes
of such
patients should be reminded periodically of the
impor-
tance of having pulmonary symptoms evaluated
promptly to
permit early detection of and treatment for TB.
Medical offices
In general, the symptoms of active TB are symptoms
for which
patients are likely to seek treatment in a medical
office.
Furthermore, the populations served by some medical
offices,
or the HCWs in the office, may be at relatively
high risk for
TB. Thus, it is likely that infectious TB will be
encountered
in a medical office. Because of the potential for
M. tuber-
culosis transmission, the following recommendations
should be
observed:
A risk assessment should be conducted
periodically, and
TB infection-control policies based on results
of the
risk assessment should be developed for the
medical
office. The policies should include provisions
for
identifying and managing patients who may have
undiag-
nosed active TB; managing patients who have
active TB;
and educating, training, counseling, and
screening HCWs.
While taking patients' initial medical
histories and at
periodic updates, HCWs who work in medical
offices should
routinely ask all patients whether they have a
history of
TB disease or have had symptoms suggestive of
TB.
Patients with a medical history and symptoms
suggestive
of active TB should receive an appropriate
diagnostic
evaluation for TB and be evaluated promptly for
possible
infectiousness. Ideally, this evaluation should
be done
in a facility that has TB isolation capability.
At a
minimum, the patient should be provided with
and asked to
wear a surgical mask, instructed to cover the
mouth and
nose with a tissue when coughing or sneezing,
and
separated as much as possible from other
patients.
Medical offices that provide evaluation or
treatment
services for TB patients should follow the
recommen-
dations for managing patients in
ambulatory-care settings
(Section II.D).
If cough-inducing procedures are to be
administered in a
medical office to patients who may have active
TB,
appropriate precautions should be followed
(Section
II.H).
Any HCW who has a persistent cough (i.e., a
cough lasting
greater than or equal to 3 weeks), especially
in the
presence of other signs or symptoms compatible
with
active TB (e.g., weight loss, night sweats,
bloody
sputum, anorexia, or fever) should be evaluated
promptly
for TB. HCWs with such signs or symptoms should
not
return to the workplace until a diagnosis of TB
has been
excluded or until they are on therapy and a
determination
has been made that they are noninfectious.
HCWs who work in medical offices in which there
is a
likelihood of exposure to patients who have
infectious TB
should be included in employer-sponsored
education,
training, counseling, and PPD testing programs
appro-
priate to the level of risk in the office.
In medical offices that provide care to
populations at
relatively high risk for active TB, use of
engineering
controls as described in this document for
general-use
areas (e.g., waiting rooms) may be appropriate
(Section
II.F; Suppl. 3).
Supplement 1: Determining the Infectiousness of a TB Patient
The infectiousness of patients with TB correlates with the number
of
organisms expelled into the air, which, in turn, correlates with
the
following factors: a) disease in the lungs, airways, or larynx; b)
presence
of cough or other forceful expiratory measures; c) presence of
acid-fast
bacilli (AFB) in the sputum; d) failure of the patient to cover the
mouth and
nose when coughing; e) presence of cavitation on chest radiograph;
f)
inappropriate or short duration of chemotherapy; and g)
administration of
procedures that can induce coughing or cause aerosolization of M.
tuberculosis (e.g., sputum induction).
The most infectious persons are most likely those who have not been
treated
for TB and who have either a) pulmonary or laryngeal TB and a cough
or are
undergoing cough-inducing procedures, b) a positive AFB sputum
smear, or c)
cavitation on chest radiograph. Persons with extrapulmonary TB
usually are
not infectious unless they have a) concomitant pulmonary disease;
b)
nonpulmonary disease located in the respiratory tract or oral
cavity; or c)
extrapulmonary disease that includes an open abscess or lesion in
which the
concentration of organisms is high, especially if drainage from the
abscess
or lesion is extensive (20,22). Coinfection with HIV does not
appear to
affect the infectiousness of TB patients (63-65).
In general, children who have TB may be less likely than adults to
be
infectious; however, transmission from children can occur.
Therefore,
children with TB should be evaluated for infectiousness using the
same
parameters as for adults (i.e., pulmonary or laryngeal TB, presence
of cough
or cough-inducing procedures, positive sputum AFB smear, cavitation
on chest
radiograph, and adequacy and duration of therapy). Pediatric
patients who may
be infectious include those who a) are not on therapy, b) have just
been
started on therapy, or c) are on inadequate therapy, and who a)
have
laryngeal or extensive pulmonary involvement, b) have pronounced
cough or are
undergoing cough-inducing procedures, c) have positive sputum AFB
smears, or
d) have cavitary TB. Children who have typical primary tuberculous
lesions
and do not have any of the indicators of infectiousness listed
previously
usually do not need to be placed in isolation. Because the source
case for
pediatric TB patients often occurs in a member of the infected
child's family
(45), parents and other visitors of all pediatric TB patients
should be
evaluated for TB as soon as possible.
Infection is most likely to result from exposure to persons who
have
unsuspected pulmonary TB and are not receiving anti-TB therapy or
from
persons who have diagnosed TB and are not receiving adequate
therapy.
Administration of effective anti-TB therapy has been associated
with
decreased infectiousness among persons who have active TB (66).
Effective
therapy reduces coughing, the amount of sputum produced, and the
number of
organisms in the sputum. However, the period of time a patient must
take
effective therapy before becoming noninfectious varies between
patients (67).
For example, some TB patients are never infectious, whereas those
with
unrecognized or inadequately treated drug-resistant TB may remain
infectious
for weeks or months (24). Thus, decisions about infectiousness
should be made
on an individual basis.
In general, patients who have suspected or confirmed active TB
should be
considered infectious if they a) are coughing, b) are undergoing
cough-
inducing procedures, or c) have positive AFB sputum smears, and if
they a)
are not on chemotherapy, b) have just started chemotherapy, or c)
have a poor
clinical or bacteriologic response to chemotherapy. A patient who
has drug-
susceptible TB and who is on adequate chemotherapy and has had a
significant
clinical and bacteriologic response to therapy (i.e., reduction in
cough,
resolution of fever, and progressively decreasing quantity of
bacilli on
smear) is probably no longer infectious. However, because
drug-susceptibility
results are not usually known when the decision to discontinue
isolation is
made, all TB patients should remain in isolation while hospitalized
until
they have had three consecutive negative sputum smears collected on
different
days and they demonstrate clinical improvement.
Supplement 2: Diagnosis and Treatment of Latent TB Infection and
Active TB
Diagnostic Procedures for TB Infection and Disease
A diagnosis of TB may be considered for any patient who has a
persistent
cough (i.e., a cough lasting greater than or equal to 3 weeks)
or other
signs or symptoms compatible with TB (e.g., bloody sputum,
night sweats,
weight loss, anorexia, or fever). However, the index of
suspicion for TB
will vary in different geographic areas and will depend on the
prevalence
of TB and other characteristics of the population served by the
facility.
The index of suspicion for TB should be very high in areas or
among
groups of patients in which the prevalence of TB is high
(Section I.B).
Persons for whom a diagnosis of TB is being considered should
receive
appropriate diagnostic tests, which may include PPD skin
testing, chest
radiography, and bacteriologic studies (e.g., sputum microscopy
and
culture).
PPD Skin Testing and Anergy Testing
Application and reading of PPD skin tests
The PPD skin test is the only method available for
demonstrating
infection with M. tuberculosis. Although currently
available PPD
tests are less than 100% sensitive and specific for
detection of
infection with M. tuberculosis, no better diagnostic
methods have
yet been devised. Interpretation of PPD test results
requires
knowledge of the antigen used, the immunologic basis
for the
reaction to this antigen, the technique used to
administer and
read the test, and the results of epidemiologic and
clinical
experience with the test (2,5,6). The PPD test, like
all medical
tests, is subject to variability, but many of the
variations in
administering and reading PPD tests can be avoided by
proper
training and careful attention to details.
The intracutaneous (Mantoux) administration of a
measured amount
of PPD-tuberculin is currently the preferred method for
doing the
test. One-tenth milliliter of PPD (5 TU) is injected
just beneath
the surface of the skin on either the volar or dorsal
surface of
the forearm. A discrete, pale elevation of the skin
(i.e., a
wheal) that is 6-10 mm in diameter should be produced.
PPD test results should be read by designated, trained
personnel
between 48 and 72 hours after injection. Patient or HCW
self-
reading of PPD test results should not be accepted
(68). The
result of the test is based on the presence or absence
of an
induration at the injection site. Redness or erythema
should not
be measured. The transverse diameter of induration
should be
recorded in millimeters.
Interpretation of PPD skin tests
General
The interpretation of a PPD reaction should be
influenced by
the purpose for which the test was given (e.g.,
epidemiologic
versus diagnostic purposes), by the prevalence of
TB
infection in the population being tested, and by
the
consequences of false classification. Errors in
classifi-
cation can be minimized by establishing an
appropriate
definition of a positive reaction (Table_S21).
The positive-predictive value of PPD tests (i.e,
the
probability that a person with a positive PPD test
is
actually infected with M. tuberculosis) is
dependent on the
prevalence of TB infection in the population being
tested and
the specificity of the test (69,70). In populations
with a
low prevalence of TB infection, the probability
that a
positive PPD test represents true infection with M.
tuber-
culosis is very low if the cut-point is set too low
(i.e.,
the test is not adequately specific). In
populations with a
high prevalence of TB infection, the probability
that a
positive PPD test using the same cut-point
represents true
infection with M. tuberculosis is much higher. To
ensure that
few persons infected with tubercle bacilli will be
misclas-
sified as having negative reactions and few persons
not
infected with tubercle bacilli will be
misclassified as
having positive reactions, different cut-points are
used to
separate positive reactions from negative reactions
for
different populations, depending on the risk for TB
infection
in that population.
A lower cut-point (i.e., 5 mm) is used for persons
in the
highest risk groups, which include HIV-infected
persons,
recent close contacts of persons with TB (e.g., in
the
household or in an unprotected occupational
exposure similar
in intensity and duration to household contact),
and persons
who have abnormal chest radiographs with fibrotic
changes
consistent with inactive TB. A higher cut-point
(i.e., 10 mm)
is used for persons who are not in the highest risk
group but
who have other risk factors (e.g., injecting-drug
users known
to be HIV seronegative; persons with certain
medical condi-
tions that increase the risk for progression from
latent TB
infection to active TB {Table_S21}); medically
under-
served, low-income populations; persons born in
foreign
countries that have a high prevalence of TB; and
residents of
correc-tional institutions and nursing homes). An
even higher
cut-point (i.e., 15 mm) is used for all other
persons who
have none of the above risk factors.
Recent PPD converters are considered members of a
high-risk
group. A greater than or equal to 10 mm increase in
the size
of the induration within a 2-year period is
classified as a
conversion from a negative to a positive test
result for
persons less than 35 years of age. An increase of
induration
of greater than or equal to 15 mm within a 2-year
period is
classified as a conversion for persons greater than
or equal
to 35 years of age (5).
HCWs
In general, HCWs should have their skin-test
results inter-
preted according to the recommendations in this
supplement
and in sections 1, 2, 3, and 5 of Table_S21.
However, the
prevalence of TB in the facility should be
considered when
choosing the appropriate cut-point for defining a
positive
PPD reaction. In facilities where there is
essen-tially no
risk for exposure to TB patients (i.e., minimal- or
very low-
risk facilities {Section II.B}), an induration
greater than
or equal to 15 mm may be an appropriate cut-point
for HCWs
who have no other risk factors. In other facilities
where TB
patients receive care, the appropriate cut-point
for HCWs who
have no other risk factors may be greater than or
equal to 10
mm.
A recent PPD test conversion in an HCW should be
defined
generally as an increase of greater than or equal
to 10 mm in
the size of induration within a 2-year period. For
HCWs in
facilities where exposure to TB is very unlikely
(e.g.,
minimal-risk facilities), an increase of greater
than or
equal to 15 mm within a 2-year period may be more
appropriate
for defining a recent conversion because of the
lower
positive-predictive value of the test in such
groups.
Anergy testing
HIV-infected persons may have suppressed reactions to
PPD skin
tests because of anergy, particularly if their CD4+
T-lymphocyte
counts decline (71). Persons with anergy will have a
negative PPD
test regardless of infection with M. tuberculosis.
HIV-infected
persons should be evaluated for anergy in conjunction
with PPD
testing (72). Two companion antigens (e.g., Candida
antigen and
tetanus toxoid) should be administered in addition to
PPD.
Persons with greater than or equal to 3 mm of
induration to any
of the skin tests (including tuberculin) are considered
not
anergic. Reactions of greater than or equal to 5 mm to
PPD are
considered to be evidence of TB infection in
HIV-infected persons
regardless of the reactions to the companion antigens.
If there
is no reaction (i.e., less than 3 mm induration) to any
of the
antigens, the person being tested is considered
anergic. Deter-
mination of whether such persons are likely to be
infected with
M. tuberculosis must be based on other epidemiologic
factors
(e.g., the proportion of other persons with the same
level of
exposure who have positive PPD test results and the
intensity or
duration of exposure to infectious TB patients that the
anergic
person experienced).
Pregnancy and PPD skin testing
Although thousands (perhaps millions) of pregnant women
have been
PPD skin tested since the test was devised, thus far no
docu-
mented episodes of fetal harm have resulted from use of
the
tuberculin test (73). Pregnancy should not exclude a
female HCW
from being skin tested as part of a contact
investigation or as
part of a regular skin-testing program.
BCG vaccination and PPD skin testing
BCG vaccination may produce a PPD reaction that cannot
be
distinguished reliably from a reaction caused by
infection with
M. tuberculosis. For a person who was vaccinated with
BCG, the
probability that a PPD test reaction results from
infection with
M. tuberculosis increases a) as the size of the
reaction
increases, b) when the person is a contact of a person
with TB,
c) when the person's country of origin has a high
prevalence of
TB, and d) as the length of time between vaccination
and PPD
testing increases. For example, a PPD test reaction of
greater
than or equal to 10 mm probably can be attributed to M.
tuber-
culosis infection in an adult who was vaccinated with
BCG as a
child and who is from a country with a high prevalence
of TB
(74,75).
The booster phenomenon
The ability of persons who have TB infection to react
to PPD may
gradually wane. For example, if tested with PPD, adults
who were
infected during their childhood may have a negative
reaction.
However, the PPD could boost the hypersensitivity, and
the size
of the reaction could be larger on a subsequent test.
This
boosted reaction may be misinterpreted as a PPD test
conversion
from a newly acquired infection. Misinterpretation of a
boosted
reaction as a new infection could result in unnecessary
investi-
gations of laboratory and patient records in an attempt
to
identify the source case and in unnecessary
prescription of
preventive therapy for HCWs. Although boosting can
occur among
persons in any age group, the likelihood of the
reaction
increases with the age of the person being tested
(6,76).
When PPD testing of adults is to be repeated
periodically (as in
HCW skin-testing programs), two-step testing can be
used to
reduce the likelihood that a boosted reaction is
misinterpreted
as a new infection. Two-step testing should be
performed on all
newly employed HCWs who have an initial negative PPD
test result
at the time of employment and have not had a documented
negative
PPD test result during the 12 months preceding the
initial test.
A second test should be performed 1-3 weeks after the
first test.
If the second test result is positive, this is most
likely a
boosted reaction, and the HCW should be classified as
previously
infected. If the second test result remains negative,
the HCW is
classified as uninfected, and a positive reaction to a
subsequent
test is likely to represent a new infection with M.
tuberculosis.
Chest Radiography
Patients who have positive skin-test results or symptoms
suggestive
of TB should be evaluated with a chest radiograph
regardless of PPD
test results. Radiographic abnormalities that strongly
suggest active
TB include upper-lobe infiltration, particularly if
cavitation is
seen (77), and patchy or nodular infiltrates in the apical
or
subapical posterior upper lobes or the superior segment of
the lower
lobe. If abnormalities are noted, or if the patient has
symptoms
suggestive of extrapulmonary TB, additional diagnostic
tests should
be conducted.
The radiographic presentation of pulmonary TB in
HIV-infected
patients may be unusual (78). Typical apical cavitary
disease is less
common among such patients. They may have infiltrates in
any lung
zone, a finding that is often associated with mediastinal
and/or
hilar adenopathy, or they may have a normal chest
radiograph,
although this latter finding occurs rarely.
Bacteriology
Smear and culture examination of at least three sputum
specimens
collected on different days is the main diagnostic
procedure for
pulmonary TB (6). Sputum smears that fail to demonstrate
AFB do not
exclude the diagnosis of TB. In the United States,
approximately 60%
of patients with positive sputum cultures have positive AFB
sputum
smears. HIV-infected patients who have pulmonary TB may be
less
likely than immunocompetent patients to have AFB present on
sputum
smears, which is consistent with the lower frequency of
cavitary
pulmonary disease observed among HIV-infected persons
(39,41).
Specimens for smear and culture should contain an adequate
amount of
expectorated sputum but not much saliva. If a diagnosis of
TB cannot
be established from sputum, a bronchoscopy may be necessary
(36,37).
In young children who cannot produce an adequate amount of
sputum,
gastric aspirates may provide an adequate specimen for
diagnosis.
A culture of sputum or other clinical specimen that
contains M.
tuberculosis provides a definitive diagnosis of TB.
Conventional
laboratory methods may require 4-8 weeks for species
identification;
however, the use of radiometric culture techniques and
nucleic acid
probes facilitates more rapid detection and identification
of
mycobacteria (79,80). Mixed mycobacterial infection, either
simultaneous or sequential, can obscure the identification
of M.
tuberculosis during the clinical evaluation and the
laboratory
analysis (42). The use of nucleic acid probes for both M.
avium
complex and M. tuberculosis may be useful for identifying
mixed
mycobacterial infections in clinical specimens.
Preventive Therapy for Latent TB Infection and Treatment of
Active TB
Preventive Therapy for Latent TB Infection
Determining whether a person with a positive PPD test
reaction or
conversion is a candidate for preventive therapy must be
based on a)
the likelihood that the reaction represents true infection
with M.
tuberculosis (as determined by the cut-points), b) the
estimated risk
for progression from latent infection to active TB, and c)
the risk
for hepatitis associated with taking isoniazid (INH)
preventive
therapy (as determined by age and other factors).
HCWs with positive PPD test results should be evaluated for
preven-
tive therapy regardless of their ages if they a) are recent
converters, b) are close contacts of persons who have
active TB, c)
have a medical condition that increases the risk for TB, d)
have HIV
infection, or e) use injecting drugs (5). HCWs with
positive PPD test
results who do not have these risk factors should be
evaluated for
preventive therapy if they are less than 35 years of age.
Preventive therapy should be considered for anergic persons
who are
known contacts of infectious TB patients and for persons
from
populations in which the prevalence of TB infection is very
high
(e.g., a prevalence of greater than 10%).
Because the risk for INH-associated hepatitis may be
increased during
the peripartum period, the decision to use preventive
therapy during
pregnancy should be made on an individual basis and should
depend on
the patient's estimated risk for progression to active
disease. In
general, preventive therapy can be delayed until after
delivery.
However, for pregnant women who were probably infected
recently or
who have high-risk medical conditions, especially HIV
infection, INH
preventive therapy should begin when the infection is
documented
(81-84). No evidence suggests that INH poses a carcinogenic
risk to
humans (85-87).
The usual preventive therapy regimen is oral INH 300 mg
daily for
adults and 10 mg/kg/day for children (88). The recommended
duration
of therapy is 12 months for persons with HIV infection and
9 months
for children. Other persons should receive INH therapy for
6-12
months. For persons who have silicosis or a chest
radiograph
demonstrating inactive fibrotic lesions and who have no
evidence of
active TB, acceptable regimens include a) 4 months of INH
plus
rifampin or b) 12 months of INH, providing that infection
with INH-
resistant organisms is unlikely (33). For persons likely to
be
infected with MDR-TB, alternative multidrug preventive
therapy
regimens should be considered (89).
All persons placed on preventive therapy should be educated
regarding
the possible adverse reactions associated with INH use, and
they
should be questioned carefully at monthly intervals by
qualified
personnel for signs or symptoms consistent with liver
damage or other
adverse effects (81-84,88,90,91). Because INH-associated
hepatitis
occurs more frequently among persons greater than 35 years
of age, a
transaminase measurement should be obtained from persons in
this age
group before initiation of INH therapy and then obtained
monthly
until treatment has been completed. Other factors
associated with an
increased risk for hepatitis include daily alcohol use,
chronic liver
disease, and injecting-drug use. In addition, postpubertal
black and
Hispanic women may be at greater risk for hepatitis or drug
interactions (92). More careful clinical monitoring of
persons with
these risk factors and possibly more frequent laboratory
monitoring
should be considered. If any of these tests exceeds three
to five
times the upper limit of normal, discontinuation of INH
should be
strongly considered. Liver function tests are not a
substitute for
monthly clinical evaluations or for the prompt assessment
of signs or
symptoms of adverse reactions that could occur between the
regularly
scheduled evaluations (33).
Persons who have latent TB infection should be advised that
they can
be reinfected with another strain of M. tuberculosis (93).
Treatment of Patients Who Have Active TB
Drug-susceptibility testing should be performed on all
initial
isolates from patients with TB. However, test results may
not be
available for several weeks, making selection of an initial
regimen
difficult, especially in areas where drug-resistant TB has
been
documented. Current recommendations for therapy and dosage
schedules
for the treatment of drug-susceptible TB should be followed
(Table_S22; Table_S23) (43). Streptomycin is
contraindicated
in the treatment of pregnant women because of the risk for
ototoxi-
city to the fetus. In geographic areas or facilities in
which drug-
resistant TB is highly prevalent, the initial treatment
regimen used
while results of drug-susceptibility tests are pending may
need to be
expanded. This decision should be based on analysis of
surveil-lance
data.
When results from drug-susceptibility tests become
available, the
regimen should be adjusted appropriately (94-97). If drug
resistance
is present, clinicians unfamiliar with the management of
patients
with drug-resistant TB should seek expert consultation.
For any regimen to be effective, adherence to the regimen
must be
ensured. The most effective method of ensuring adherence is
the use
of DOT after the patient has been discharged from the
hospital
(43,91). This practice should be coordinated with the
public health
department.
Supplement 3: Engineering Controls
Introduction
This supplement provides information regarding the use of
ventilation
(Section II) and UVGI (Section III) for preventing the
transmission of M.
tuberculosis in health-care facilities. The information
provided is
primarily conceptual and is intended to educate staff in the
health-care
facility concerning engineering controls and how these controls
can be
used as part of the TB infection-control program. This
supplement should
not be used in place of consultation with experts, who can
assume respon-
sibility for advising on ventilation system design and
selection, instal-
lation, and maintenance of equipment.
The recommendations for engineering controls include a) local
exhaust
ventilation (i.e., source control), b) general ventilation, and
c) air
cleaning. General ventilation considerations include a)
dilution and
removal of contaminants, b) airflow patterns within rooms, c)
airflow
direction in facilities, d) negative pressure in rooms, and e)
TB
isolation rooms. Air cleaning or disinfection can be
accomplished by
filtration of air (e.g., through HEPA filters) or by UVGI.
II. Ventilation
Ventilation systems for health-care facilities should be
designed, and
modified when necessary, by ventilation engineers in
collaboration with
infection-control and occupational health staff.
Recommendations for
designing and operating ventilation systems have been published
by ASHRAE
(47), AIA (48), and the American Conference of Governmental
Industrial
Hygienists, Inc. (98).
As part of the TB infection-control plan, health-care facility
personnel
should determine the number of TB isolation rooms, treatment
rooms, and
local exhaust devices (i.e., for cough-inducing or
aerosol-generating
procedures) that the facility needs. The locations of these
rooms and
devices will depend on where in the facility the ventilation
conditions
recommended in this document can be achieved. Grouping
isolation rooms
together in one area of the facility may facilitate the care of
TB
patients and the installation and maintenance of optimal
engineering
controls (particularly ventilation).
Periodic evaluations of the ventilation system should review
the number
of TB isolation rooms, treatment rooms, and local exhaust
devices needed
and the regular maintenance and monitoring of the local and
general
exhaust systems (including HEPA filtration systems if they are
used).
The various types and conditions of ventilation systems in
health-care
facilities and the individual needs of these facilities
preclude the
ability to provide specific instructions regarding the
implementation of
these recommendations. Engineering control methods must be
tailored to
each facility on the basis of need and the feasibility of using
the
ventilation and air-cleaning concepts discussed in this
supplement.
Local Exhaust Ventilation
Purpose: To capture airborne contaminants at or near their
source
(i.e., the source control method) and remove these
contaminants
without exposing persons in the area to infectious agents
(98).
Source control techniques can prevent or reduce the spread
of
infectious droplet nuclei into the general air circulation
by
entrapping infectious droplet nuclei as they are being
emitted by the
patient (i.e., the source). These techniques are especially
important
when performing procedures likely to generate aerosols
containing
infectious particles and when infectious TB patients are
coughing or
sneezing.
Local exhaust ventilation is a preferred source control
technique,
and it is often the most efficient way to contain airborne
contam-
inants because it captures these contaminants near their
source
before they can disperse. Therefore, the technique should
be used, if
feasible, wherever aerosol-generating procedures are
performed. Two
basic types of local exhaust devices use hoods: a) the
enclosing
type, in which the hood either partially or fully encloses
the
infectious source; and b) the exterior type, in which the
infectious
source is near but outside the hood. Fully enclosed hoods,
booths, or
tents are always preferable to exterior types because of
their
superior ability to prevent contaminants from escaping into
the HCW's
breathing zone. Descriptions of both enclosing and exterior
devices
have been published previously (98).
Enclosing devices
The enclosing type of local exhaust ventilation device
includes
laboratory hoods used for processing specimens that
could contain
viable infectious organisms, booths used for sputum
induction or
administration of aerosolized medications (e.g.,
aerosolized
pentamidine) (Figure_S31), and tents or hoods made
of vinyl
or other materials used to enclose and isolate a
patient. These
devices are available in various configurations. The
most simple
of these latter devices is a tent that is placed over
the
patient; the tent has an exhaust connection to the room
discharge
exhaust system. The most complex device is an enclosure
that has
a sophisticated self-contained airflow and
recirculation system.
Both tents and booths should have sufficient airflow to
remove at
least 99% of airborne particles during the interval
between the
departure of one patient and the arrival of the next
(99). The
time required for removing a given percentage of
airborne
particles from an enclosed space depends on several
factors.
These factors include the number of ACH, which is
determined by
the number of cubic feet of air in the room or booth
and the rate
at which air is entering the room or booth at the
intake source;
the location of the ventilation inlet and outlet; and
the
physical configuration of the room or booth
(Table_S31).
Exterior devices
The exterior type of local exhaust ventilation device
is usually
a hood very near, but not enclosing, the infectious
patient. The
airflow produced by these devices should be sufficient
to prevent
cross-currents of air near the patient's face from
causing escape
of droplet nuclei. Whenever possible, the patient
should face
directly into the hood opening so that any coughing or
sneezing
is directed into the hood, where the droplet nuclei are
captured.
The device should maintain an air velocity of greater
than or
equal to 200 feet per minute at the patient's breathing
zone to
ensure capture of droplet nuclei.
Discharge exhaust from booths, tents, and hoods
Air from booths, tents, and hoods may be discharged
into the room
in which the device is located or it may be exhausted
to the
outside. If the air is discharged into the room, a HEPA
filter
should be incorporated at the discharge duct or vent of
the
device. The exhaust fan should be located on the
discharge side
of the HEPA filter to ensure that the air pressure in
the filter
housing and booth is negative with respect to adjacent
areas.
Uncontaminated air from the room will flow into the
booth through
all openings, thus preventing infectious droplet nuclei
in the
booth from escaping into the room. Most commercially
available
booths, tents, and hoods are fitted with HEPA filters,
in which
case additional HEPA filtration is not needed.
If the device does not incorporate a HEPA filter, the
air from
the device should be exhausted to the outside in
accordance with
recommendations for isolation room exhaust (Suppl. 3,
Section
II.B.5). (See Supplement 3, Section II.C, for
information
regarding recirculation of exhaust air.)
General Ventilation
General ventilation can be used for several purposes,
including
diluting and removing contaminated air, controlling airflow
patterns
within rooms, and controlling the direction of airflow
throughout a
facility. Information on these topics is contained in the
following
sections.
Dilution and removal
Purpose: To reduce the concentration of contaminants in
the air.
General ventilation maintains air quality by two
processes:
dilution and removal of airborne contaminants.
Uncontaminated
supply (i.e., incoming) air mixes with the contaminated
room air
(i.e., dilution), which is subsequently removed from
the room by
the exhaust system (i.e., removal). These processes
reduce the
concentration of droplet nuclei in the room air.
Types of general ventilation systems
Two types of general ventilation systems can be
used for
dilution and removal of contaminated air: the
single-pass
system and the recirculating system. In a
single-pass system,
the supply air is either outside air that has been
appro-
priately heated and cooled or air from a central
system that
supplies a number of areas. After air passes
through the room
(or area), 100% of that air is exhausted to the
outside. The
single-pass system is the preferred choice in areas
where
infectious airborne droplet nuclei are known to be
present
(e.g., TB isolation rooms or treatment rooms)
because it
prevents contaminated air from being recirculated
to other
areas of the facility.
In a recirculating system, a small portion of the
exhaust air
is discharged to the outside and is replaced with
fresh
outside air, which mixes with the portion of
exhaust air that
was not discharged to the outside. The resulting
mixture,
which can contain a large proportion of
contaminated air, is
then recirculated to the areas serviced by the
system. This
air mixture could be recirculated into the general
ventila-
tion, in which case contaminants may be carried
from contam-
inated areas to uncontaminated areas.
Alternatively, the air
mixture could also be recirculated within a
specific room or
area, in which case other areas of the facility
will not be
affected (Suppl. 3, Section II.C.3).
Ventilation rates
Recommended general ventilation rates for
health-care
facilities are usually expressed in number of ACH.
This
number is the ratio of the volume of air entering
the room
per hour to the room volume and is equal to the
exhaust
airflow (Q {cubic feet per minute}) divided by the
room
volume (V {cubic feet}) multiplied by 60 (i.e., ACH
= Q / V
x 60).
The feasibility of achieving specific ventilation
rates
depends on the construction and operational
requirements of
the ventilation system (e.g., the energy
requirements to move
and to heat or cool the air). The feasibility of
achieving
specific ventilation rates may also be different
for retro-
fitted facilities and newly constructed facilities.
The
expense and effort of achieving specific higher
ventilation
rates for new construction may be reasonable,
whereas retro-
fitting an existing facility to achieve similar
ventilation
rates may be more difficult. However, achieving
higher
ventilation rates by using auxiliary methods (e.g.,
room-air
recirculation) in addition to exhaust ventilation
may be
feasible in existing facilities (Suppl. 3, Section
II.C).
Airflow patterns within rooms (air mixing)
Purpose: To provide optimum airflow patterns and
prevent both
stagnation and short-circuiting of air.
General ventilation systems should be designed to
provide optimal
patterns of airflow within rooms and prevent air
stagnation or
short-circuiting of air from the supply to the exhaust
(i.e.,
passage of air directly from the air supply to the air
exhaust).
To provide optimal airflow patterns, the air supply and
exhaust
should be located such that clean air first flows to
parts of the
room where HCWs are likely to work, and then flows
across the
infectious source and into the exhaust. In this way,
the HCW is
not positioned between the infectious source and the
exhaust
location. Although this configuration may not always be
possible,
it should be used whenever feasible. One way to achieve
this
airflow pattern is to supply air at the side of the
room opposite
the patient and exhaust it from the side where the
patient is
located. Another method, which is most effective when
the supply
air is cooler than the room air, is to supply air near
the
ceiling and exhaust it near the floor (Figure_S32).
Airflow
patterns are affected by large air temperature
differentials, the
precise location of the supply and exhausts, the
location of
furniture, the movement of HCWs and patients, and the
physical
configuration of the space. Smoke tubes can be used to
visualize
airflow patterns in a manner similar to that described
for
estimating room air mixing.
Adequate air mixing, which requires that an adequate
number of
ACH be provided to a room (Suppl. 3, Section II.B.1),
must be
ensured to prevent air stagnation within the room.
However, the
air will not usually be changed the calculated number
of times
per hour because the airflow patterns in the room may
not permit
complete mixing of the supply and room air in all parts
of the
room. This results in an "effective" airflow rate in
which the
supplied airflow may be less than required for proper
ventila-
tion. To account for this variation, a mixing factor
(which
ranges from 1 for perfect mixing to 10 for poor mixing)
is
applied as a multiplier to determine the actual supply
airflow
(i.e., the recommended ACH multiplied by the mixing
factor equals
the actual required ACH) (51,98). The room air supply
and exhaust
system should be designed to achieve the lowest mixing
factor
possible. The mixing factor is determined most
accurately by
experimentally testing each space configuration, but
this
procedure is complex and time-consuming. A reasonably
good
qualitative measure of mixing can be estimated by an
experienced
ventilation engineer who releases smoke from smoke
tubes at a
number of locations in the room and observes the
movement of the
smoke. Smoke movement in all areas of the room
indicates good
mixing. Stagnation of air in some areas of the room
indicates
poor mixing, and movement of the supply and exhaust
openings or
redirection of the supply air is necessary.
Airflow direction in the facility
Purpose: To contain contaminated air in localized areas
in a
facility and prevent its spread to uncontaminated
areas.
Directional airflow
The general ventilation system should be designed
and
balanced so that air flows from less contaminated
(i.e., more
clean) to more contaminated (less clean) areas
(47,48). For
example, air should flow from corridors (cleaner
areas) into
TB isolation rooms (less clean areas) to prevent
spread of
contaminants to other areas. In some special
treatment rooms
in which operative and invasive procedures are
performed, the
direction of airflow is from the room to the
hallway to
provide cleaner air during these procedures.
Cough-inducing
or aerosol-generating procedures (e.g.,
bronchoscopy and
irrigation of tuberculous abscesses) should not be
performed
in rooms with this type of airflow on patients who
may have
infectious TB.
Negative pressure for achieving directional airflow
The direction of airflow is controlled by creating
a lower
(negative) pressure in the area into which the flow
of air is
desired. For air to flow from one area to another,
the air
pressure in the two areas must be different. Air
will flow
from a higher pressure area to a lower pressure
area. The
lower pressure area is described as being at
negative
******** pressure relative to the higher pressure
area.
Negative pressure is attained by exhausting air
from an area
at a higher rate than air is being supplied. The
level of
negative pressure necessary to achieve the desired
airflow
will depend on the physical configuration of the
ventilation
system and area, including the airflow path and
flow
openings, and should be determined on an individual
basis by
an experienced ventilation engineer.
Achieving negative pressure in a room
Purpose: To control the direction of airflow between
the room and
adjacent areas, thereby preventing contaminated air
from escaping
from the room into other areas of the facility.
Pressure differential
The minimum pressure difference necessary to
achieve and
maintain negative pressure that will result in
airflow into
the room is very small (0.001 inch of water).
Higher
pressures ( greater than or equal to 0.001 inch of
water) are
satisfactory; however, these higher pressures may
be
difficult to achieve. The actual level of negative
pressure
achieved will depend on the difference in the
ventilation
exhaust and supply flows and the physical
configuration of
the room, including the airflow path and flow
openings. If
the room is well sealed, negative pressures greater
than the
minimum of 0.001 inch of water may be readily
achieved.
However, if rooms are not well sealed, as may be
the case in
many facilities (especially older facilities),
achieving
higher negative pressures may require
exhaust/supply flow
differentials beyond the capability of the
ventilation
system.
To establish negative pressure in a room that has a
normally
functioning ventilation system, the room supply and
exhaust
airflows are first balanced to achieve an exhaust
flow of
either 10% or 50 cubic feet per minute (cfm)
greater than the
supply (whichever is the greater). In most
situations, this
specification should achieve a negative pressure of
at least
0.001 inch of water. If the minimum 0.001 inch of
water is
not achieved and cannot be achieved by increasing
the flow
differential (within the limits of the ventilation
system),
the room should be inspected for leakage (e.g.,
through
doors, windows, plumbing, and equipment wall
penetrations),
and corrective action should be taken to seal the
leaks.
Negative pressure in a room can be altered by
changing the
ventilation system operation or by the opening and
closing of
the room's doors, corridor doors, or windows. When
an
operating configuration has been established, it is
essential
that all doors and windows remain properly closed
in the
isolation room and other areas (e.g., doors in
corridors that
affect air pressure) except when persons need to
enter or
leave the room or area.
Alternate methods for achieving negative pressure
Although an anteroom is not a substitute for
negative
pressure in a room, it may be used to reduce escape
of
droplet nuclei during opening and closing of the
isolation
room door. Some anterooms have their own air supply
duct, but
others do not. The TB isolation room should have
negative
pressure relative to the anteroom, but the air
pressure in
the anteroom relative to the corridor may vary
depending on
the building design. This should be determined, in
accordance
with applicable regulations, by a qualified
ventilation
engineer.
If the existing ventilation system is incapable of
achieving
the desired negative pressure because the room
lacks a
separate ventilation system or the room's system
cannot
provide the proper airflow, steps should be taken
to provide
a means to discharge air from the room. The amount
of air to
be exhausted will be the same as discussed
previously (Suppl.
3, Section II.B.4.a).
Fixed room-air recirculation systems (i.e., systems
that
recirculate the air in an entire room) may be
designed to
achieve negative pressure by discharging air
outside the room
(Suppl. 3, Section II.C.3).
Some portable room-air recirculation units (Suppl.
3, Section
II.C.3.b.) are designed to discharge air to the
outside to
achieve negative pressure. Air cleaners that can
accomplish
this must be designed specifically for this
purpose.
A small centrifugal blower (i.e., exhaust fan) can
be used to
exhaust air to the outside through a window or
outside wall.
This approach may be used as an interim measure to
achieve
negative pressure, but it provides no fresh air and
suboptimal dilution.
Another approach to achieving the required pressure
difference is to pressurize the corridor. Using
this method,
the corridor's general ventilation system is
balanced to
create a higher air pressure in the corridor than
in the
isolation room; the type of balancing necessary
depends on
the configuration of the ventilation system.
Ideally, the
corridor air supply rate should be increased while
the
corridor exhaust rate is not increased. If this is
not
possible, the exhaust rate should be decreased by
resetting
appropriate exhaust dampers. Caution should be
exercised,
however, to ensure that the exhaust rate is not
reduced below
acceptable levels. This approach requires that all
settings
used to achieve the pressure balance, including
doors, be
maintained. This method may not be desirable if the
corridor
being pressurized has rooms in which negative
pressure is not
desired. In many situations, this system is
difficult to
achieve, and it should be considered only after
careful
review by ventilation personnel.
Monitoring negative pressure
The negative pressure in a room can be monitored by
visually
observing the direction of airflow (e.g., using
smoke tubes)
or by measuring the differential pressure between
the room
and its surrounding area.
Smoke from a smoke tube can be used to observe
airflow
between areas or airflow patterns within an area.
To check
the negative pressure in a room by using a smoke
tube, hold
the smoke tube near the bottom of the door and
approximately
2 inches in front of the door, or at the face of a
grille or
other opening if the door has such a feature, and
generate a
small amount of smoke by gently squeezing the bulb
(Figure_S33). The smoke tube should be held
parallel to
the door, and the smoke should be issued from the
tube slowly
to ensure the velocity of the smoke from the tube
does not
overpower the air velocity. The smoke will travel
in the
direction of airflow. If the room is at negative
pressure,
the smoke will travel under the door and into the
room (e.g.,
from higher to lower pressure). If the room is not
at
negative pressure, the smoke will be blown outward
or will
stay stationary. This test must be performed while
the door
is closed. If room air cleaners are being used in
the room,
they should be running. The smoke is irritating if
inhaled,
and care should be taken not to inhale it directly
from the
smoke tube. However, the quantity of smoke issued
from the
tube is minimal and is not detectable at short
distances from
the tube.
Differential pressure-sensing devices also can be
used to
monitor negative pressure; they can provide either
periodic
(noncontinuous) pressure measurements or continuous
pressure
monitoring. The continuous monitoring component may
simply be
a visible and/or audible warning signal that air
pressure is
low. In addition, it may also provide a pressure
readout
signal, which can be recorded for later
verification or used
to automatically adjust the facility's ventilation
control
system.
Pressure-measuring devices should sense the room
pressure
just inside the airflow path into the room (e.g.,
at the
bottom of the door). Unusual airflow patterns
within the room
can cause pressure variations; for example, the air
can be at
negative pressure at the middle of a door and at
positive
pressure at the bottom of the same door
(Figure_S34). If
the pressure-sensing ports of the device cannot be
located
directly across the airflow path, it will be
necessary to
validate that the negative pressure at the sensing
point is
and remains the same as the negative pressure
across the flow
path.
Pressure-sensing devices should incorporate an
audible
warning with a time delay to indicate that a door
is open.
When the door to the room is opened, the negative
pressure
will decrease. The time-delayed signal should allow
sufficient time for persons to enter or leave the
room
without activating the audible warning.
A potential problem with using pressure-sensing
devices is
that the pressure differentials used to achieve the
low
negative pressure necessitate the use of very
sensitive
mechanical devices, electronic devices, or pressure
gauges to
ensure accurate measurements. Use of devices that
cannot
measure these low pressures (i.e., pressures as low
as 0.001
inch of water) will require setting higher negative
pressures
that may be difficult and, in some instances,
impractical to
achieve (Suppl. 3, Section II.B.4).
Periodic checks are required to ensure that the
desired
negative pressure is present and that the
continuous
monitoring devices, if used, are operating
properly. If smoke
tubes or other visual checks are used, TB isolation
rooms and
treatment rooms should be checked frequently for
negative
pressure. Rooms undergoing changes to the
ventilation system
should be checked daily. TB isolation rooms should
be checked
daily for negative pressure while being used for TB
isolation. If these rooms are not being used for
patients who
have suspected or confirmed TB but potentially
could be used
for such patients, the negative pressure in the
rooms should
be checked monthly. If pressure-sensing devices are
used,
negative pressure should be verified at least once
a month by
using smoke tubes or taking pressure measurements.
HEPA filtration
Purpose: To remove contaminants from the air.
HEPA filtration can be used as a method of air cleaning
that supple-
ments other recommended ventilation measures. For the
purposes of
these guidelines, HEPA filters are defined as air-cleaning
devices
that have a demonstrated and documented minimum removal
efficiency of
99.97% of particles greater than or equal to 0.3 um in
diameter. HEPA
filters have been shown to be effective in reducing the
concentration
of Aspergillus spores (which range in size from 1.5 um to 6
um) to
below measurable levels (100-102). The ability of HEPA
filters to
remove tubercle bacilli from the air has not been studied,
but M.
tuberculosis droplet nuclei probably range from 1 um to 5
um in
diameter (i.e., approximately the same size as Aspergillus
spores).
Therefore, HEPA filters can be expected to remove
infectious droplet
nuclei from contaminated air. HEPA filters can be used to
clean air
before it is exhausted to the outside, recirculated to
other areas of
a facility, or recirculated within a room. If the device is
not
completely passive (e.g., it utilizes techniques such as
electro-
statics) and the failure of the electrostatic components
permits loss
of filtration efficiency to less than 99.97%, the device
should not
be used in systems that recirculate air back into the
general
facility ventilation system from TB isolation rooms and
treatment
rooms in which procedures are performed on patients who may
have
infectious TB (Suppl. 3, Section II.C.2).
HEPA filters can be used in a number of ways to reduce or
eliminate
infectious droplet nuclei from room air or exhaust. These
methods
include placement of HEPA filters a) in exhaust ducts to
remove
droplet nuclei from air being discharged to the outside,
either
directly or through ventilation equipment; b) in ducts
discharging
room air into the general ventilation system; and c) in
fixed or
portable room-air cleaners. The effectiveness of portable
HEPA room-
air cleaning units has not been evaluated adequately, and
there is
probably considerable variation in their effectiveness.
HEPA filters
can also be used in exhaust ducts or vents that discharge
air from
booths or enclosures into the surrounding room (Suppl. 3,
Section
II.A.3). In any application, HEPA filters should be
installed
carefully and maintained meticulously to ensure adequate
function.
Manufacturers of room-air cleaning equipment should provide
documen-
tation of the HEPA filter efficiency and the efficiency of
the
installed device in lowering room-air contaminant levels.
Use of HEPA filtration when exhausting air to the
outside
HEPA filters can be used as an added safety measure to
clean air
from isolation rooms and local exhaust devices (i.e.,
booths,
tents, or hoods used for cough-inducing procedures)
before
exhausting it directly to the outside, but such use is
unneces-
sary if the exhaust air cannot re-enter the ventilation
system
supply. The use of HEPA filters should be considered
wherever
exhaust air could possibly reenter the system.
In many instances, exhaust air is not discharged
directly to the
outside; rather, the air is directed through
heat-recovery
devices (e.g., heat wheels). Heat wheels are often used
to reduce
the costs of operating ventilation systems (103). If
such units
are used with the system, a HEPA filter should also be
used. As
the wheel rotates, energy is transferred into or
removed from the
supply inlet air stream. The HEPA filter should be
placed
upstream from the heat wheel because of the potential
for leakage
across the seals separating the inlet and exhaust
chambers and
the theoretical possibility that droplet nuclei could
be impacted
on the wheel by the exhaust air and subsequently
stripped off
into the supply air.
Recirculation of HEPA-filtered air to other areas of a
facility
Air from TB isolation rooms and treatment rooms used to
treat
patients who have confirmed or suspected infectious TB
should be
exhausted to the outside in accordance with applicable
federal,
state, and local regulations. The air should not be
recirculated
into the general ventilation. In some instances,
recirculation of
air into the general ventilation system from such rooms
is
unavoidable (i.e., in existing facilities in which the
ventila-
tion system or facility configuration makes venting the
exhaust
to the outside impossible). In such cases, HEPA filters
should be
installed in the exhaust duct leading from the room to
the
general ventilation system to remove infectious
organisms and
particulates the size of droplet nuclei from the air
before it is
returned to the general ventilation system (Section
II.F; Suppl.
3). Air from TB isolation rooms and treatment rooms in
new or
renovated facilities should not be recirculated into
the general
ventilation system.
Recirculation of HEPA-filtered air within a room
Individual room-air recirculation can be used in areas
where
there is no general ventilation system, where an
existing system
is incapable of providing adequate airflow, or where an
increase
in ventilation is desired without affecting the fresh
air supply
or negative pressure system already in place.
Recirculation of
HEPA-filtered air within a room can be achieved in
several ways:
by exhausting air from the room into a duct,
filtering it
through a HEPA filter installed in the duct, and
returning it to
the room (Figure_S35); b) by filtering air through
HEPA
recirculation systems mounted on the wall or ceiling of
the room
(Figure_S36); or c) by filtering air through
portable HEPA
recirculation systems. In this document, the first two
of these
approaches are referred to as fixed room-air
recirculation
systems, because the HEPA filter devices are fixed in
place and
are not easily movable.
Fixed room-air recirculation systems
The preferred method of recirculating HEPA-filtered
air
within a room is a built-in system, in which air is
exhausted
from the room into a duct, filtered through a HEPA
filter,
and returned to the room (Figure_S35). This
technique may
be used to add air changes in areas where there is
a
recommended minimum ACH that is difficult to meet
with
general ventilation alone. The air does not have to
be
conditioned, other than by the filtration, and this
permits
higher airflow rates than the general ventilation
system can
usually achieve. An alternative is the use of HEPA
filtration
units that are mounted on the wall or ceiling of
the room
(Figure_S37). Fixed recirculation systems are
preferred
over portable (free-standing) units because they
can be
installed and maintained with a greater degree of
reliability.
Portable room-air recirculation units
Portable HEPA filtration units may be considered
for recir-
culating air within rooms in which there is no
general
ventilation system, where the system is incapable
of
providing adequate airflow, or where increased
effectiveness
in room airflow is desired. Effectiveness depends
on circu-
lating as much of the air in the room as possible
through the
HEPA filter, which may be difficult to achieve and
evaluate.
The effectiveness of a particular unit can vary
depending on
the room's configuration, the furniture and persons
in the
room, and placement of the HEPA filtration unit and
the
supply and exhaust grilles. Therefore, the
effectiveness of
the portable unit may vary considerably in rooms
with
different configurations or in the same room if
moved from
one location to another in the room. If portable
units are
used, caution should be exercised to ensure they
can recir-
culate all or nearly all of the room air through
the HEPA
filter. Some commercially available units may not
be able to
meet this requirement because of design limitations
or insuf-
ficient airflow capacity. In addition, units should
be
designed and operated to ensure that persons in the
room
cannot interfere with or otherwise compromise the
functioning
of the unit. Portable HEPA filtration units have
not been
evaluated adequately to determine their role in TB
infection-
control programs.
Portable HEPA filtration units should be designed
to achieve
the equivalent of greater than or equal to 12 ACH.
They
should also be designed to ensure adequate air
mixing in all
areas of the hospital rooms in which they are used,
and they
should not interfere with the current ventilation
system.
Some HEPA filtration units employ UVGI for
disinfecting air
after HEPA filtration. However, whether exposing
the HEPA-
filtered air to UV irradiation further decreases
the concen-
tration of contaminants is not known.
Evaluation of room-air recirculation systems and
units
Detailed and accurate evaluations of room-air
recirculation
systems and units require the use of sophisticated
test
equipment and lengthy test procedures that are not
practical.
However, an estimate of the unit's ability to
circulate the
air in the room can be made by visualizing airflow
patterns
as was described previously for estimating room air
mixing
(Suppl. 3, Section II.B.1). If the air movement is
good in
all areas of the room, the unit should be
effective.
Installing, maintaining, and monitoring HEPA filters
Proper installation and testing and meticulous
maintenance are
critical if a HEPA filtration system is used (104),
especially if
the system used recirculates air to other parts of the
facility.
Improper design, installation, or maintenance could
allow infec-
tious particles to circumvent filtration and escape
into the
general ventilation system (47). HEPA filters should be
installed
to prevent leakage between filter segments and between
the filter
bed and its frame. A regularly scheduled maintenance
program is
required to monitor the HEPA filter for possible
leakage and for
filter loading. A quantitative leakage and filter
performance
test (e.g., the dioctal phthalate {DOP} penetration
test {105})
should be performed at the initial installation and
every time
the filter is changed or moved. The test should be
repeated every
6 months for filters in general-use areas and in areas
with
systems that exhaust air that is likely to be
contaminated with
M. tuberculosis (e.g, TB isolation rooms).
A manometer or other pressure-sensing device should be
installed
in the filter system to provide an accurate and
objective means
of determining the need for filter replacement.
Pressure drop
characteristics of the filter are supplied by the
manufacturer of
the filter. Installation of the filter should allow for
mainten-
ance that will not contaminate the delivery system or
the area
served. For general infection-control purposes, special
care
should be taken to not jar or drop the filter element
during or
after removal.
The scheduled maintenance program should include
procedures for
installation, removal, and disposal of filter elements.
HEPA
filter maintenance should be performed only by
adequately trained
personnel. Appropriate respiratory protection should be
worn
while performing maintenance and testing procedures. In
addition,
filter housing and ducts leading to the housing should
be
labelled clearly with the words "Contaminated Air" (or
a similar
warning).
When a HEPA filter is used, one or more lower
efficiency dispos-
able prefilters installed upstream will extend the
useful life of
the HEPA filter. A disposable filter can increase the
life of a
HEPA filter by 25%. If the disposable filter is
followed by a 90%
extended surface filter, the life of the HEPA filter
can be
extended almost 900% (98). These prefilters should be
handled and
disposed of in the same manner as the HEPA filter.
TB Isolation Rooms and Treatment Rooms
Purpose: To separate patients who are likely to have
infectious TB
from other persons, to provide an environment that will
allow
reduction of the concentration of droplet nuclei through
various
engineering methods, and to prevent the escape of droplet
nuclei from
such rooms into the corridor and other areas of the
facility using
directional airflow.
A hierarchy of ventilation methods used to achieve a
reduction in the
concentration of droplet nuclei and to achieve directional
airflow
using negative pressure has been developed (Table_S32).
The
methods are listed in order from the most desirable to the
least
desirable. The method selected will depend on the
configuration of
the isolation room and the ventilation system in the
facility; the
determination should be made in consultation with a
ventilation
engineer.
Preventing the escape of droplet nuclei from the room
Rooms used for TB isolation should be single-patient
rooms with
negative pressure relative to the corridor or other
areas
connected to the room. Doors between the isolation room
and other
areas should remain closed except for entry into or
exit from the
room. The room's openings (e.g., windows and electrical
and
plumbing entries) should be sealed as much as possible.
However,
a small gap of 1/8 to 1/2 inch should be at the bottom
of the
door to provide a controlled airflow path. Proper use
of negative
pressure will prevent contaminated air from escaping
the room.
Reducing the concentration of droplet nuclei in the
room
ASHRAE (47), AIA (48), and the Health Resources and
Services
Administration (49) recommend a minimum of 6 ACH for TB
isolation
rooms and treatment rooms. This ventilation rate is
based on
comfort- and odor-control considerations. The
effectiveness of
this level of airflow in reducing the concentration of
droplet
nuclei in the room, thus reducing the transmission of
airborne
pathogens, has not been evaluated directly or
adequately.
Ventilation rates greater than 6 ACH are likely to
produce an
incrementally greater reduction in the concentration of
bacteria
in a room than are lower rates (50-52). However,
accurate quanti-
tation of decreases in risk that would result from
specific
increases in general ventilation levels has not been
performed
and may not be possible.
To reduce the concentration of droplet nuclei, TB
isolation rooms
and treatment rooms in existing health-care facilities
should
have an airflow of greater than or equal to 6 ACH.
Where
feasible, this airflow rate should be increased to
greater than
or equal to 12 ACH by adjusting or modifying the
ventilation
system or by using auxiliary means (e.g., recirculation
of air
through fixed HEPA filtration units or portable air
cleaners)
(Suppl. 3, Section II.C) (53). New construction or
renovation of
existing health-care facilities should be designed so
that TB
isolation rooms achieve an airflow of greater than or
equal to 12
ACH.
Exhaust from TB isolation rooms and treatment rooms
Air from TB isolation rooms and treatment rooms in
which patients
with infectious TB may be examined should be exhausted
directly
to the outside of the building and away from air-intake
vents,
persons, and animals in accordance with federal, state,
and local
regulations concerning environmental discharges. (See
Suppl. 3,
Section II.C, for information regarding recirculation
of exhaust
air.) Exhaust ducts should not be located near areas
that may be
populated (e.g., near sidewalks or windows that could
be opened).
Ventilation system exhaust discharges and inlets should
be
designed to prevent reentry of exhausted air. Wind
blowing over
a building creates a highly turbulent recirculation
zone, which
can cause exhausted air to reenter the building
(Figure_S37).
Exhaust flow should be discharged above this zone
(Suppl. 3,
Section II.C.1). Design guidelines for proper placement
of
exhaust ducts can be found in the 1989 ASHRAE
Fundamentals
Handbook (106). If recirculation of air from such rooms
into the
general ventilation system is unavoidable, the air
should be
passed through a HEPA filter before recirculation
(Suppl. 3,
Section II.C.2).
Alternatives to TB isolation rooms
Isolation can also be achieved by use of
negative-pressure
enclosures (e.g, tents or booths) (Suppl. 3, Section
II.A.1).
These can be used to provide patient isolation in areas
such as
emergency rooms and medical testing and treatment areas
and to
supplement isolation in designated isolation rooms.
UVGI
Purpose: To kill or inactivate airborne tubercle bacilli.
Research has demonstrated that UVGI is effective in killing or
inacti-
vating tubercle bacilli under experimental conditions
(66,107-110) and in
reducing transmission of other infections in hospitals (111),
military
housing (112), and classrooms (113-115). Because of the results
of
numerous studies (116-120) and the experiences of TB clinicians
and
mycobacteriologists during the past several decades, the use of
UVGI has
been recommended as a supplement to other TB infection-control
measures
in settings where the need for killing or inactivating tubercle
bacilli
is important (2,4,121-125).
UV radiation is defined as that portion of the electromagnetic
spectrum
described by wavelengths from 100 to 400 nm. For convenience of
classi-
fication, the UV spectrum has been separated into three
different wave-
length bands: UV-A (long wavelengths, range: 320-400 nm), UV-B
(midrange
wavelengths, range: 290-320 nm), and UV-C (short wavelengths,
range:
100-290 nm) (126). Commercially available UV lamps used for
germicidal
purposes are low-pressure mercury vapor lamps (127) that emit
radiant
energy in the UV-C range, predominantly at a wavelength of
253.7 nm
(128).
Applications
UVGI can be used as a method of air disinfection to
supplement other
engineering controls. Two systems of UVGI can be used for
this
purpose: duct irradiation and upper-room air irradiation.
Duct irradiation
Purpose: To inactivate tubercle bacilli without
exposing persons
to UVGI.
In duct irradiation systems, UV lamps are placed inside
ducts
that remove air from rooms to disinfect the air before
it is
recirculated. When UVGI duct systems are properly
designed,
installed, and maintained, high levels of UV radiation
may be
produced in the duct work. The only potential for human
exposure
to this radiation occurs during maintenance operations.
Duct irradiation may be used:
In a TB isolation room or treatment room to
recirculate air
from the room, through a duct containing UV lamps,
and back
into the room. This recirculation method can
increase the
overall room airflow but does not increase the
supply of
fresh outside air to the room.
In other patients' rooms and in waiting rooms,
emergency
rooms, and other general-use areas of a facility
where
patients with undiagnosed TB could potentially
contaminate
the air, to recirculate air back into the general
ventila-
tion.
Duct-irradiation systems are dependent on airflow
patterns
within a room that ensure that all or nearly all of
the room
air circulates through the duct.
Upper-room air irradiation
Purpose: To inactivate tubercle bacilli in the upper
part of the
room, while minimizing radiation exposure to persons in
the lower
part of the room.
In upper-room air irradiation, UVGI lamps are suspended
from the
ceiling or mounted on the wall. The bottom of the lamp
is
shielded to direct the radiation upward but not
downward. The
system depends on air mixing to take irradiated air
from the
upper to the lower part of the room, and nonirradiated
air from
the lower to the upper part. The irradiated air space
is much
larger than that in a duct system.
UVGI has been effective in killing bacteria under
conditions
where air mixing was accomplished mainly by convection.
For
example, BCG was atomized in a room that did not have
supple-
mental ventilation (120), and in another study a
surrogate
bacteria, Serratia marcesens, was aerosolized in a room
with a
ventilation rate of 6 ACH (129). These reports
estimated the
effect of UVGI to be equivalent to 10 and 39 ACH,
respectively,
for the organisms tested, which are less resistant to
UVGI than
M. tuberculosis (120). The addition of fans or some
heating/air
conditioning arrangements may double the effectiveness
of UVGI
lamps (130-132). Greater rates of ventilation, however,
may
decrease the length of time the air is irradiated, thus
decreasing the killing of bacteria (117,129). The
optimal rela-
tionship between ventilation and UVGI is not known. Air
irradi-
ation lamps used in corridors have been effective in
killing
atomized S. marcesens (133). Use of UVGI lamps in an
outpatient
room has reduced culturable airborne bacteria by
14%-19%.
However, the irradiation did not reduce the
concentration of
gram-positive, rod-shaped bacteria; although
fast-growing
mycobacteria were cultured, M. tuberculosis could not
be
recovered from the room's air samples because of fungal
over-
growth of media plates (134).
Upper-room air UVGI irradiation may be used:
In isolation or treatment rooms as a supplemental
method of
air cleaning.
In other patients' rooms and in waiting rooms,
emergency
rooms, corridors, and other central areas of a
facility where
patients with undiagnosed TB could potentially
contaminate
the air.
Determinants of UVGI effectiveness include room
configura-
tion, UV lamp placement, and the adequacy of
airflow patterns
in bringing contaminated air into contact with the
irradiated
upper-room space. Air mixing may be facilitated by
supplying
cool air near the ceiling in rooms where warmer air
(or a
heating device) is present below. The ceiling
should be high
enough for a large volume of upper-room air to be
irradiated
without HCWs and patients being overexposed to UV
radiation.
Limitations
Because the clinical effectiveness of UV systems varies,
and because
of the risk for transmission of M. tuberculosis if a system
malfunc-
tions or is maintained improperly, UVGI is not recommended
for the
following specific applications:
Duct systems using UVGI are not recommended as a
substitute
for HEPA filters if air from isolation rooms must be
recirculated
to other areas of a facility.
UVGI alone is not recommended as a substitute for
HEPA
filtration or local exhaust of air to the outside from
booths,
tents, or hoods used for cough-inducing procedures.
UVGI is not a substitute for negative pressure.
The use of UV lamps and HEPA filtration in a single unit
would not be
expected to have any infection-control benefits not
provided by use
of the HEPA filter alone.
The effectiveness of UVGI in killing airborne tubercle
bacilli
depends on the intensity of UVGI, the duration of contact
the
organism has with the irradiation, and the relative
humidity
(66,108,111). Humidity can have an adverse effect on UVGI
effective-
ness at levels greater than 70% relative humidity for S.
marcescens
(135). The interaction of these factors has not been fully
defined,
however, making precise recommendations for individual UVGI
instal-
lations difficult to develop.
Old lamps or dust-covered UV lamps are less effective;
therefore,
regular maintenance of UVGI systems is crucial.
Safety Issues
Short-term overexposure to UV radiation can cause erythema
and kera-
toconjunctivitis (136,137). Broad-spectrum UV radiation has
been
associated with increased risk for squamous and basal cell
carcinomas
of the skin (138). UV-C was recently classified by the
International
Agency for Research on Cancer as "probably carcinogenic to
humans
(Group 2A)" (138). This classification is based on studies
suggesting
that UV-C radiation can induce skin cancers in animals; DNA
damage,
chromosomal aberrations and sister chromatid exchange and
transfor-
mation in human cells in vitro; and DNA damage in mammalian
skin
cells in vivo. In the animal studies, a contribution of
UV-B to the
tumor effects could not be excluded, but the effects were
greater
than expected for UV-B alone (138). Although some recent
studies have
demonstrated that UV radiation can activate HIV gene
promoters (i.e.,
the genes in HIV that prompt replication of the virus) in
laboratory
samples of human cells (139-144), the implications of these
in vitro
findings for humans are unknown.
In 1972, the National Institute for Occupational Safety and
Health
(NIOSH) published a recommended exposure limit (REL) for
occupational
exposure to UV radiation (136). The REL is intended to
protect
workers from the acute effects of UV exposure (e.g.,
erythema and
photokeratoconjunctivitis). However, photosensitive persons
and those
exposed concomitantly to photoactive chemicals may not be
protected
by the recommended standard.
If proper procedures are not followed, HCWs performing
maintenance on
such fixtures are at risk for exposure to UV radiation.
Because UV
fixtures used for upper-room air irradiation are present in
rooms,
rather than hidden in ducts, safety may be much more
difficult to
achieve and maintain. Fixtures must be designed and
installed to
ensure that UV exposure to persons in the room (including
HCWs and
inpatients) are below current safe exposure levels. Recent
health
hazard evaluations conducted by CDC have noted problems
with over-
exposure of HCWs to UVGI and with inadequate maintenance,
training,
labelling, and use of personal protective equipment
(145-147).
The current number of persons who are properly trained in
UVGI system
design and installation is limited. CDC strongly recommends
that a
competent UVGI system designer be consulted to address
safety consid-
erations before such a system is procured and installed.
Experts who
might be consulted include industrial hygienists,
engineers, and
health physicists. Principles for the safe installation of
UV lamp
fixtures have been developed and can be used as guidelines
(148,149).
If UV lamps are being used in a facility, the general TB
education of
HCWs should include:
The basic principles of UVGI systems (i.e., how they
work and
what their limitations are).
The potential hazardous effects of UVGI if
overexposure
occurs.
The potential for photosensitivity associated with
certain
medical conditions or use of some medications.
The importance of general maintenance procedures for
UVGI
fixtures.
Exposure to UV intensities above the REL should be avoided.
Light-
weight clothing made of tightly woven fabric and
UV-absorbing
sunscreens with solar-protection factors (SPFs) greater
than or equal
to 15 may help protect photosensitive persons. HCWs should
be advised
that any eye or skin irritation that develops after UV
exposure
should be examined by occupational health staff.
Exposure Criteria for UV Radiation
The NIOSH REL for UV radiation is wavelength dependent
because
different wavelengths of UV radiation have different
adverse effects
on the skin and eyes (136). Relative spectral effectiveness
(S sub l)
is used to compare various UV sources with a source
producing UV
radiation at 270 nm, the wavelength of maximum ocular
sensitivity.
For example, the S sub l at 254 nm is 0.5; therefore, twice
as much
energy is required at 254 nm to produce an identical
biologic effect
at 270 nm (136). Thus, at 254 nm, the NIOSH REL is 0.006
joules per
square centimeter (J/cm2); and at 270 nm, it is 0.003
J/cm2.
For germicidal lamps that emit radiant energy predominantly
at a
wavelength of 254 nm, proper use of the REL requires that
the
measured irradiance level (E) in microwatts per square
centimeter
(uW/cm2) be multiplied by the relative spectral
effectiveness at 254
nm (0.5) to obtain the effective irradiance (Eeff). The
maximum
permissible exposure time can then be determined for
selected values
of Eeff (Table_S33), or it can be calculated (in
seconds) by
dividing 0.003 J/cm2 (the NIOSH REL at 270 nm) by Eeff in
uW/cm2
(136,150).
To protect HCWs who are exposed to germicidal UV radiation
for 8
hours per workday, the measured irradiance (E) should be
less than or
equal to 0.2 uW/cm2. This is calculated by obtaining Eeff
(0.1
YuW/cm2) (Table_S33) and then dividing this value by S
sub l
(0.5).
Maintenance and Monitoring
Labelling and posting
Warning signs should be posted on UV lamps and wherever
high-
intensity (i.e., UV exposure greater than the REL)
germicidal UV
irradiation is present (e.g., upper-room air space and
accesses
to ducts {if duct irradiation is used}) to alert
maintenance
staff or other HCWs of the hazard. Some examples are
shown below:
CAUTION CAUTION
ULTRAVIOLET ENERGY: ULTRAVIOLET
ENERGY:
TURN OFF LAMPS BEFORE PROTECT EYES &
SKIN
ENTERING UPPER ROOM
Maintenance
Because the intensity of UV lamps fluctuates as they
age, a
schedule for replacing the lamps should be developed.
The
schedule can be determined from either a time/use log
or a system
based on cumulative time. The tube should be checked
periodically
for dust build-up, which lessens the output of UVGI. If
the tube
is dirty, it should be allowed to cool, then cleaned
with a damp
cloth. Tubes should be replaced if they stop glowing or
if they
flicker to an objectionable extent. Maintenance
personnel must
turn off all UV tubes before entering the upper part of
the room
or before accessing ducts for any purpose. Only a few
seconds of
direct exposure to the intense UV radiation in the
upper-room air
space or in ducts can cause burns. Protective equipment
(e.g.,
gloves and goggles {and/or face shields}) should be
worn if
exposure greater than the recommended standard is
anticipated.
Banks of UVGI tubes can be installed in ventilating
ducts. Safety
devices should be used on access doors to eliminate
hazard to
maintenance personnel. For duct irradiation systems,
the access
door for servicing the lamps should have an inspection
window
********* through which the lamps are checked
periodically for
dust build-up and malfunctioning. The access door
should have a
warning sign written in languages appropriate for
maintenance
personnel to alert them to the health hazard of looking
directly
at bare tubes. The lock for this door should have an
automatic
electric switch or other device that turns off the
lamps when the
door is opened.
Two types of fixtures are used in upper-room air
irradiation:
wall-mounted fixtures that have louvers to block
downward
radiation and ceiling-mounted fixtures that have
baffles to block
radiation below the horizontal plane of the UV tube.
The actual
UV tube in either type of fixture must not be visible
from any
normal position in the room. Light switches that can be
locked
should be used, if possible, to prevent injury to
personnel who
might unintentionally turn the lamps on during
maintenance
procedures.
In most applications, properly shielding the UV lamps
to provide
protection from most, if not all, of the direct UV
radiation is
not difficult. However, radiation reflected from glass,
polished
metal, and high-gloss ceramic paints can be harmful to
persons in
the room, particularly if more than one UV lamp is in
use.
Surfaces in irradiated rooms that can reflect UVGI into
occupied
areas of the room should be covered with non-UV
reflecting
material.
Monitoring
A regularly scheduled evaluation of the UV intensity to
which
HCWs, patients, and others are exposed should be
conducted.
UV measurements should be made in various locations
within a room
using a detector designed to be most sensitive at 254
nm.
Equipment used to measure germicidal UV radiation
should be
maintained and calibrated on a regular schedule.
A new UV installation must be carefully checked for hot
spots
(i.e., areas of the room where the REL is exceeded) by
an indus-
trial hygienist or other person knowledgeable in making
UV
measurements. UV radiation levels should not exceed
those in the
recommended guidelines.
Supplement 4: Respiratory Protection
Considerations for Selection of Respirators
Personal respiratory protection should be used by a) persons
entering
rooms where patients with known or suspected infectious TB are
being
isolated, b) persons present during cough-inducing or
aerosol-generating
procedures performed on such patients, and c) persons in other
settings
where administrative and engineering controls are not likely to
protect
them from inhaling infectious airborne droplet nuclei. These
other
settings should be identified on the basis of the facility's
risk
assessment.
Although data regarding the effectiveness of respiratory
protection from
many hazardous airborne materials have been collected, the
precise level
of effectiveness in protecting HCWs from M. tuberculosis
transmission in
health-care settings has not been determined. Information
concerning the
transmission of M. tuberculosis is incomplete. Neither the
smallest
infectious dose of M. tuberculosis nor the highest level of
exposure to
M. tuberculosis at which transmission will not occur has been
defined
conclusively (59,151,152). Furthermore, the size distribution
of droplet
nuclei and the number of particles containing viable M.
tuberculosis that
are expelled by infectious TB patients have not been defined
adequately,
and accurate methods of measuring the concentration of
infectious droplet
nuclei in a room have not been developed.
Nevertheless, in certain settings the administrative and
engineering
controls may not adequately protect HCWs from airborne droplet
nuclei
(e.g., in TB isolation rooms, treatment rooms in which
cough-inducing or
aerosol-generating procedures are performed, and ambulances
during the
transport of infectious TB patients). Respiratory protective
devices used
in these settings should have characteristics that are suitable
for the
organism they are protecting against and the settings in which
they are
used.
Performance Criteria for Personal Respirators for
Protection Against
Transmission of M. tuberculosis
Respiratory protective devices used in health-care settings
for
protection against M. tuberculosis should meet the
following standard
criteria. These criteria are based on currently available
informa-
tion, including a) data on the effectiveness of respiratory
protec-
tion against noninfectious hazardous materials in
workplaces other
than health-care settings and on an interpretation of how
these data
can be applied to respiratory protection against M.
tuberculosis; b)
data on the efficiency of respirator filters in filtering
biological
aerosols; c) data on face-seal leakage; and d) data on the
character-
istics of respirators that were used in conjunction with
adminis-
trative and engineering controls in outbreak settings where
trans-
mission to HCWs and patients was terminated.
The ability to filter particles 1 um in size in the
unloaded
state with a filter efficiency of greater than or equal
to 95%
(i.e., filter leakage of less than or equal to 5%),
given flow
rates of up to 50 L per minute.
Available data suggest that infectious droplet nuclei
range in
size from 1 um to 5 um; therefore, respirators used in
health-
care settings should be able to efficiently filter the
smallest
particles in this range. Fifty liters per minute is a
reasonable
estimate of the highest airflow rate an HCW is likely
to achieve
during breathing, even while performing strenuous work
activi-
ties.
The ability to be qualitatively or quantitatively fit
tested in
a reliable way to obtain a face-seal leakage of less
than or
equal to 10% (54,55).
The ability to fit the different facial sizes and
characteristics
of HCWs, which can usually be met by making the
respirators
available in at least three sizes.
The ability to be checked for facepiece fit, in
accordance with
OSHA standards and good industrial hygiene practice, by
HCWs each
time they put on their respirators (54,55).
In some settings, HCWs may be at risk for two types of
exposure: a)
inhalation of M. tuberculosis and b) mucous membrane
exposure to
fluids that may contain bloodborne pathogens. In these
settings,
protection against both types of exposure should be used.
When operative procedures (or other procedures requiring a
sterile
field) are performed on patients who may have infectious
TB, respira-
tory protection worn by the HCW should serve two functions:
a) it
should protect the surgical field from the respiratory
secretions of
the HCW and b) it should protect the HCW from infectious
droplet
nuclei that may be expelled by the patient or generated by
the
procedure. Respirators with expiration valves and
positive-pressure
respirators do not protect the sterile field; therefore, a
respirator
that does not have a valve and that meets the criteria in
Supplement
4, Section I.A, should be used.
Specific Respirators
The OSHA respiratory protection standard requires that all
respira-
tory protective devices used in the workplace be certified
by NIOSH.
********** NIOSH-approved HEPA respirators are the only
currently
available air-purifying respirators that meet or exceed the
standard
performance criteria stated above. However, the NIOSH
certification
procedures are currently being revised (153). Under the
proposed
revision, filter materials would be tested at a flow rate
of 85 L/min
for penetration by particles with a median aerodynamic
diameter of
0.3 um and, if certified, would be placed in one of the
following
categories: type A, which has greater than or equal to
99.97%
efficiency (similar to current HEPA filter media); type B,
greater
than or equal to 99% efficiency; or type C, greater than or
equal to
95% efficiency. According to this proposed scheme, type C
filter
material would meet or exceed the standard performance
criteria
specified in this document.
The facility's risk assessment may identify a limited
number of
selected settings (e.g., bronchoscopy performed on patients
suspected
of having TB or autopsy performed on deceased persons
suspected of
having had active TB at the time of death) where the
estimated risk
for transmission of M. tuberculosis may be such that a
level of
respiratory protection exceeding the standard criteria is
appro-
priate. In such circumstances, a level of respiratory
protection
exceeding the standard criteria and compatible with
patient-care
delivery (e.g., negative-pressure respirators that are more
protec-
tive; powered air-purifying particulate respirators
{PAPRs}; or
positive-pressure airline, half-mask respirators) should be
provided
by employers to HCWs who are exposed to M. tuberculosis.
Information
on these and other respirators may be found in the NIOSH
Guide to
Industrial Respiratory Protection (55).
The Effectiveness of Respiratory Protective Devices
The following information, which is based on experience
with respira-
tory protection in the industrial setting, summarizes the
available
data about the effectiveness of respiratory protection
against
hazardous airborne materials. Data regarding protection
against
transmission of M. tuberculosis are not available.
The parameters used to determine the effectiveness of a
respiratory
protective device are face-seal efficacy and filter
efficacy.
Face-seal leakage
Face-seal leakage compromises the ability of
particulate respira-
tors to protect HCWs from airborne materials (154-156).
A proper
seal between the respirator's sealing surface and the
face of the
person wearing the respirator is essential for
effective and
reliable performance of any negative-pressure
respirator. This
seal is less critical, but still important, for
positive-pressure
respirators. Face-seal leakage can result from various
factors,
including incorrect facepiece size or shape, incorrect
or
defective facepiece sealing-lip, beard growth,
perspiration or
facial oils that can cause facepiece slippage, failure
to use all
the head straps, incorrect positioning of the facepiece
on the
face, incorrect head strap tension or position,
improper respir-
ator maintenance, and respirator damage.
Every time a person wearing a negative-pressure
particulate
respirator inhales, a negative pressure (relative to
the
workplace air) is created inside the facepiece. Because
of this
negative pressure, air containing contaminants can take
a path of
least resistance into the respirator -- through leaks
at the
face-seal interface -- thus avoiding the
higher-resistance filter
material. Currently available, cup-shaped, disposable
particulate
respirators have from 0 to 20% face-seal leakage
(55,154). This
face-seal leakage results from the variability of the
human face
and from limitations in the respirator's design,
construction,
and number of sizes available. The face-seal leakage is
probably
higher if the respirator is not fitted properly to the
HCW's
face, tested for an adequate fit by a qualified person,
and then
checked for fit by the HCW every time the respirator is
put on.
Face-seal leakage may be reduced to less than 10% with
improve-
ments in design, a greater variety in available sizes,
and appro-
priate fit testing and fit checking.
In comparison with negative-pressure respirators,
positive-
pressure respirators produce a positive pressure inside
the
facepiece under most conditions of use. For example, in
a PAPR,
a blower forcibly draws ambient air through HEPA
filters, then
delivers the filtered air to the facepiece. This air is
blown
into the facepiece at flow rates that generally exceed
the
expected inhalation flow rates. The positive pressure
inside the
facepiece reduces face-seal leakage to low levels,
particularly
during the relatively low inhalation rates expected in
health-
care settings. PAPRs with a tight-fitting facepiece
have less
than 2% face-seal leakage under routine conditions
(55). Powered-
air respirators with loose-fitting facepieces, hoods,
or helmets
have less than 4% face-seal leakage under routine
conditions
(55). Thus, a PAPR may offer lower levels of face-seal
leakage
than nonpowered, half-mask respirators. Full facepiece,
non-
powered respirators have the same leakage (i.e., less
than 2%) as
PAPRs.
Another factor contributing to face-seal leakage of
cup-shaped,
disposable respirators is that some of these
respirators are
available in only one size. A single size may produce
higher
leakage for persons who have smaller or
difficult-to-fit faces
(157). The facepieces used for some reusable (including
HEPA and
replaceable filter, negative-pressure) and all
positive-pressure
particulate air-purifying respirators are available in
as many as
three different sizes.
Filter leakage
Aerosol leakage through respirator filters depends on
at least
five independent variables: a) the filtration
characteristics for
each type of filter, b) the size distribution of the
droplets in
the aerosol, c) the linear velocity through the
filtering
material, d) the filter loading (i.e., the amount of
contaminant
deposited on the filter), and e) any electrostatic
charges on the
filter and on the droplets in the aerosol (158).
When HEPA filters are used in particulate air-purifying
respirators, filter efficiency is so high (i.e.,
effectively
100%) that filter leakage is not a consideration.
Therefore, for
all HEPA-filter respirators, virtually all inward
leakage of
droplet nuclei occurs at the respirator's face seal.
Fit testing
Fit testing is part of the respiratory protection
program
required by OSHA for all respiratory protective devices
used in
the workplace. A fit test determines whether a
respiratory
protective device adequately fits a particular HCW. The
HCW may
need to be fit tested with several devices to determine
which
device offers the best fit. However, fit tests can
detect only
the leakage that occurs at the time of the fit testing,
and the
tests cannot distinguish face-seal leakage from filter
leakage.
Determination of facepiece fit can involve qualitative
or quanti-
tative tests (55). A qualitative test relies on the
subjective
response of the HCW being fit tested. A quantitative
test uses
detectors to measure inward leakage.
Disposable, negative-pressure particulate respirators
can be
qualitatively fit tested with aerosolized substances
that can be
tasted, although the results of this testing are
limited because
the tests depend on the subjective response of the HCW
being
tested. Quantitative fit testing of disposable
negative-pressure
particulate respirators can best be performed if the
manufacturer
provides a test respirator with a probe for this
purpose.
Replaceable filter, negative-pressure particulate
respirators and
all positive-pressure particulate respirators can be
fit tested
reliably, both qualitatively and quantitatively, when
fitted with
HEPA filters.
Fit checking
A fit check is a maneuver that an HCW performs before
each use of
the respiratory protective device to check the fit. The
fit check
can be performed according to the manufacturer's
facepiece
fitting instructions by using the applicable
negative-pressure or
positive-pressure test.
Some currently available cup-shaped, disposable
negative-pressure
particulate respirators cannot be fit checked reliably
by persons
wearing the devices because occluding the entire
surface of the
filter is difficult. Strategies for overcoming these
limitations
are being developed by respirator manufacturers.
Reuse of respirators
Conscientious respirator maintenance should be an
integral part
of an overall respirator program. This maintenance
applies both
to respirators with replaceable filters and respirators
that are
classified as disposable but that are reused.
Manufacturers'
instructions for inspecting, cleaning, and maintaining
respira-
tors should be followed to ensure that the respirator
continues
to function properly (55).
When respirators are used for protection against
noninfectious
aerosols (e.g., wood dust), which may be present in the
air in
heavy concentrations, the filter material may become
occluded
with airborne material. This occlusion may result in an
uncom-
fortable breathing resistance. In health-care settings
where
respirators are used for protection against biological
aerosols,
the concentration of infectious particles in the air is
probably
low; thus, the filter material in a respirator is very
unlikely
to become occluded with airborne material. In addition,
there is
no evidence that particles impacting on the filter
material in a
respirator are re-aerosolized easily. For these
reasons, the
filter material used in respirators in the health-care
setting
should remain functional for weeks to months.
Respirators with
replaceable filters are reusable, and a respirator
classified as
disposable may be reused by the same HCW as long as it
remains
functional.
Before each use, the outside of the filter material
should be
inspected. If the filter material is physically damaged
or
soiled, the filter should be changed (in the case of
respirators
with replaceable filters) or the respirator discarded
(in the
case of disposable respirators). Infection-control
personnel
should develop standard operating procedures for
storing,
reusing, and disposing of respirators that have been
designated
as disposable and for disposing of replaceable filter
elements.
Implementing a Personal Respiratory Protection Program
If personal respiratory protection is used in a health-care
setting, OSHA
requires that an effective personal respiratory protection
program be
developed, implemented, administered, and periodically
reevaluated
(54,55).
All HCWs who need to use respirators for protection against
infection
with M. tuberculosis should be included in the respiratory
protection
program. Visitors to TB patients should be given respirators to
wear
while in isolation rooms, and they should be given general
instructions
on how to use their respirators.
The number of HCWs included in the respiratory protection
program in each
facility will vary depending on a) the number of potentially
infectious
TB patients, b) the number of rooms or areas to which patients
with
suspected or confirmed infectious TB are admitted, and c) the
number of
HCWs needed in these rooms or areas. Where respiratory
protection
programs are required, they should include enough HCWs to
provide
adequate care for a patient with known or suspected TB should
such a
patient be admitted to the facility. However, administrative
measures
should be used to limit the number of HCWs who need to enter
these rooms
or areas, thus limiting the number of HCWs who need to be
included in the
respiratory protection program.
Information regarding the development and management of a
respiratory
protection program is available in technical training courses
that cover
the basics of personal respiratory protection. Such courses are
offered
by various organizations, such as NIOSH, OSHA, and the American
Indus-
trial Hygiene Association. Similar courses are available from
private
contractors and universities.
To be effective and reliable, respiratory protection programs
must
contain at least the following elements (55,154):
Assignment of responsibility. Supervisory responsibility
for the
respiratory protection program should be assigned to
designated
persons who have expertise in issues relevant to the
program,
including infectious diseases and occupational health.
Standard operating procedures. Written standard
operating
procedures should contain information concerning all
aspects of the
respiratory protection program.
Medical screening. HCWs should not be assigned a task
requiring
use of respirators unless they are physically able to
perform the
task while wearing the respirator. HCWs should be screened
for
pertinent medical conditions at the time they are hired,
then
rescreened periodically (55). The screening could occur as
infre-
quently as every 5 years. The screening process should
begin with a
general screening (e.g., a questionnaire) for pertinent
medical
conditions, and the results of the screening should then be
used to
identify HCWs who need further evaluation. Routine physical
examin-
ation or testing with chest radiographs or spirometry is
not
necessary or required.
Few medical conditions preclude the use of most
negative-pressure
particulate respirators. HCWs who have mild pulmonary or
cardiac
conditions may report discomfort with breathing when
wearing
negative-pressure particulate respirators, but these
respirators are
unlikely to have adverse health effects on the HCWs. Those
HCWs who
have more severe cardiac or pulmonary conditions may have
more diffi-
culty than HCWs with similar but milder conditions if
performing
duties while wearing negative-pressure respirators.
Furthermore,
these HCWs may be unable to use some PAPRs because of the
added
weight of these respirators.
Training. HCWs who wear respirators and the persons who
supervise
them should be informed about the necessity for wearing
respirators
and the potential risks associated with not doing so. This
training
should also include at a minimum:
The nature, extent, and specific hazards of M.
tuberculosis
transmission in their respective health-care facility.
A description of specific risks for TB infection among
persons
exposed to M. tuberculosis, of any subsequent treatment
with INH
or other chemoprophylactic agents, and of the
possibility of
active TB disease.
A description of engineering controls and work
practices and the
reasons why they do not eliminate the need for personal
respira-
tory protection.
An explanation for selecting a particular type of
respirator, how
the respirator is properly maintained and stored, and
the opera-
tion, capabilities, and limitations of the respirator
provided.
Instruction in how the HCW wearing the respirator
should inspect,
put on, fit check, and correctly wear the provided
respirator
(i.e., achieve and maintain proper face-seal fit on the
HCW's
face).
An opportunity to handle the provided respirator and
learn how to
put it on, wear it properly, and check the important
parts.
Instruction in how to recognize an inadequately
functioning
respirator.
5. Face-seal fit testing and fit checking. HCWs should
undergo fit
testing to identify a respirator that adequately fits each
individual
HCW. The HCW should receive fitting instructions that
include demon-
strations and practice in how the respirator should be
worn, how it
should be adjusted, and how to determine if it fits
properly. The HCW
should be taught to check the facepiece fit before each
use.
6. Respirator inspection, cleaning, maintenance, and
storage. Consci-
entious respirator maintenance should be an integral part
of an
overall respirator program. This maintenance applies both
to respir-
ators with replaceable filters and respirators that are
classified as
disposable but that are reused. Manufacturers' instructions
for
inspecting, cleaning, and maintaining respirators should be
followed
to ensure that the respirator continues to function
properly (55).
7. Periodic evaluation of the personal respiratory
protection
program. The program should be evaluated completely at
least once a
year, and both the written operating procedures and program
adminis-
tration should be revised as necessary based on the results
of the
evaluation. Elements of the program that should be
evaluated include
work practices and employee acceptance of respirator use
(i.e.,
subjective comments made by employees concerning comfort
during use
and interference with duties).
Supplement 5: Decontamination -- Cleaning, Disinfecting, and
Sterilizing of
Patient-Care Equipment
Equipment used on patients who have TB is usually not involved in
the trans-
mission of M. tuberculosis, although transmission by contaminated
broncho-
scopes has been demonstrated (159,160). Guidelines for cleaning,
disin-
fecting, and sterilizing equipment have been published (161,162).
The
rationale for cleaning, disinfecting, or sterilizing patient-care
equipment
can be understood more readily if medical devices, equipment, and
surgical
materials are divided into three general categories. These
categories --
critical, semicritical, and noncritical items -- are defined by the
potential
risk for infection associated with their use (163,164).
Critical items are instruments that are introduced directly into
the blood-
stream or into other normally sterile areas of the body (e.g.,
needles,
surgical instruments, cardiac catheters, and implants). These items
should be
sterile at the time of use.
Semicritical items are those that may come in contact with mucous
membranes
but do not ordinarily penetrate body surfaces (e.g., noninvasive
flexible and
rigid fiberoptic endoscopes or bronchoscopes, endotracheal tubes,
and anes-
thesia breathing circuits). Although sterilization is preferred for
these
instruments, high-level disinfection that destroys vegetative
microorganisms,
most fungal spores, tubercle bacilli, and small nonlipid viruses
may be used.
Meticulous physical cleaning of such items before sterilization or
high-level
disinfection is essential.
Noncritical items are those that either do not ordinarily touch the
patient
or touch only the patient's intact skin (e.g., crutches, bedboards,
blood
pressure cuffs, and various other medical accessories). These items
are not
associated with direct transmission of M. tuberculosis, and washing
them with
detergent is usually sufficient.
Health-care facility policies should specify whether cleaning,
disinfecting,
or sterilizing an item is necessary to decrease the risk for
infection.
Decisions about decontamination processes should be based on the
intended use
of the item, not on the diagnosis of the patient for whom the item
was used.
Selection of chemical disinfectants depends on the intended use,
the level of
disinfection required, and the structure and material of the item
to be
disinfected.
Although microorganisms are ordinarily found on walls, floors, and
other
environmental surfaces, these surfaces are rarely associated with
trans-
mission of infections to patients or HCWs. This is particularly
true with
organisms such as M. tuberculosis, which generally require
inhalation by the
host for infection to occur. Therefore, extraordinary attempts to
disinfect
or sterilize environmental surfaces are not indicated. If a
detergent
germicide is used for routine cleaning, a hospital-grade,
EPA-approved
germicide/disinfectant that is not tuberculocidal can be used. The
same
routine daily cleaning procedures used in other rooms in the
facility should
be used to clean TB isolation rooms, and personnel should follow
isolation
practices while cleaning these rooms. For final cleaning of the
isolation
room after a patient has been discharged, personal protective
equipment is
not necessary if the room has been ventilated for the appropriate
amount of
time (Table_S31).
References
CDC. National action plan to combat multidrug-resistant
tuberculosis.
Atlanta: US Department of Health and Human Services, Public
Health
Service, CDC, 1992.
CDC. Guidelines for preventing the transmission of
tuberculosis in
health-care settings, with special focus on HIV-related
issues. MMWR
1990;39(No. RR-17).
CDC. Draft guidelines for preventing the transmission of
tuberculosis in
health-care facilities, second edition; notice of comment
period.
Federal Register 1993;58:52810-54.
CDC. Guidelines for prevention of TB transmission in
hospitals. Atlanta:
US Department of Health and Human Services, Public Health
Service, CDC,
1982; DHHS publication no. (CDC)82-8371.
CDC. Screening for tuberculosis and tuberculous infection in
high-risk
populations, and the use of preventive therapy for tuberculous
infection
in the United States: recommendations of the Advisory
Committee for
Elimination of Tuberculosis. MMWR 1990;39(No. RR-8).
American Thoracic Society/CDC. Diagnostic standards and
classification
of tuberculosis. Am Rev Respir Dis 1990;142:725-35.
Wells WF. Aerodynamics of droplet nuclei. In: Airborne
contagion and air
hygiene. Cambridge: Harvard University Press, 1955:13-9.
Selwyn PA, Hartel D, Lewis VA, et al. A prospective study of
the risk of
tuberculosis among intravenous drug users with human
immunodeficiency
virus infection. N Engl J Med 1989;320:545-50.
Di Perri G, Cruciani M, Danzi MC, et al. Nosocomial epidemic
of active
tuberculosis among HIV-infected patients. Lancet
1989;2:1502-4.
Daley CL, Small PM, Schecter GF, et al. An outbreak of
tuberculosis with
accelerated progression among persons infected with the human
immuno-
deficiency virus: an analysis using
restriction-fragment-length poly-
morphisms. N Engl J Med 1992;326:231-5.
Edlin BR, Tokars JI, Grieco MH, et al. An outbreak of
multidrug-
resistant tuberculosis among hospitalized patients with the
acquired
immunodeficiency syndrome. N Engl J Med 1992;326:1514-21.
Dooley SW, Villarino E, Lawrence M, et al. Nosocomial
transmission of
tuberculosis in a hospital unit for HIV-infected patients.
JAMA 1992;
267:2632-4.
ten Dam HG. Research on BCG vaccination. Adv Tuberc Res
1984;21:79-106.
Barrett-Connor E. The epidemiology of tuberculosis in
physicians. JAMA
1979;241:33-8.
Brennen C, Muder RR, Muraca PW. Occult endemic tuberculosis in
a chronic
care facility. Infect Control Hosp Epidemiol 1988;9:548-52.
Goldman KP. Tuberculosis in hospital doctors. Tubercle
1988;69:237-40.
Catanzaro A. Nosocomial tuberculosis. Am Rev Respir Dis
1982;125:559-62.
Ehrenkranz NJ, Kicklighter JL. Tuberculosis outbreak in a
general
hospital: evidence of airborne spread of infection. Ann Intern
Med 1972;
77:377-82.
Haley CE, McDonald RC, Rossi L, et al. Tuberculosis epidemic
among
hospital personnel. Infect Control Hosp Epidemiol
1989;10:204-10.
Hutton MD, Stead WW, Cauthen GM, et al. Nosocomial
transmission of
tuberculosis associated with a draining tuberculous abscess. J
Infect
Dis 1990;161:286-95.
Kantor HS, Poblete R, Pusateri SL. Nosocomial transmission of
tuber-
culosis from unsuspected disease. Am J Med 1988;84:833-8.
Lundgren R, Norrman E, Asberg I. Tuberculous infection
transmitted at
autopsy. Tubercle 1987;68:147-50.
CDC. Mycobacterium tuberculosis transmission in a health
clinic --
Florida, 1988. MMWR 1989;38:256-8,263-4.
Beck-Sague C, Dooley SW, Hutton MD, et al. Outbreak of
multidrug-
resistant Mycobacterium tuberculosis infections in a hospital:
trans-
mission to patients with HIV infection and staff. JAMA
1992;268:1280-6.
CDC. Nosocomial transmission of multidrug-resistant
tuberculosis to
health-care workers and HIV-infected patients in an urban
hospital --
Florida. MMWR 1990;39:718-22.
CDC. Nosocomial transmission of multidrug-resistant
tuberculosis among
HIV-infected persons -- Florida and New York, 1988-1991. MMWR
1991;
40:585-91.
Pearson ML, Jereb JA, Frieden TR, et al. Nosocomial
transmission of
multidrug-resistant Mycobacterium tuberculosis: a risk to
patients and
health care workers. Ann Intern Med 1992;117:191-6.
Dooley SW, Jarvis WR, Martone WJ, Snider DE Jr.
Multidrug-resistant
tuberculosis {Editorial}. Ann Intern Med 1992;117:257-8.
Wenger P, Beck-Sague C, Otten J, et al. Efficacy of control
measures in
preventing nosocomial transmission of multidrug-resistant
tuberculosis
among patient and health-care workers {Abstract 53A}. In:
Program and
abstracts of the World Congress on Tuberculosis. Bethesda, MD:
National
Institutes of Health, Fogarty International Center, 1992.
Otten J, Chen J, Cleary T. Successful control of an outbreak
of multi-
drug-resistant tuberculosis in an urban teaching hospital
{Abstract
51D}. In: Program and abstracts of the World Congress on
Tuberculosis.
Bethesda, MD: National Institutes of Health, Fogarty
International
Center, 1992.
Maloney S, Pearson M, Gordon M, et al. The efficacy of
recommended
infection control measures in preventing nosocomial
transmission of
multidrug-resistant TB {Abstract 51C}. In: Program and
abstracts of the
World Congress on Tuberculosis. Bethesda, MD: National
Institutes of
Health, Fogarty International Center, 1992.
Stroud L, Tokars J, Grieco M, Gilligan M, Jarvis W.
Interruption of
nosocomial transmission of multidrug-resistant Mycobacterium
tuber-
culosis (MDR-TB) among AIDS patients in a New York City
Hospital
{Abstract A1-3}. In: Third Annual Meeting of the Society for
Hospital
Epidemiologists of America. Chicago: Society for Hospital
Epidemi-
ologists of America, 1993.
American Thoracic Society. Treatment of tuberculosis and
tuberculosis
infection in adults and children. Am J Respir Crit Care Med
1994;149:
1359-74.
Strong BE, Kubica GP. Isolation and identification of
Mycobacterium
tuberculosis. Atlanta: US Department of Health and Human
Services,
Public Health Service, CDC, 1981; DHHS publication no.
(CDC)81-8390.
CDC. Tuberculosis and human immunodeficiency virus infection:
recommen-
dations of the Advisory Committee for the Elimination of
Tuberculosis
(ACET). MMWR 1989;38:236-8,243-50.
Willcox PA, Benator SR, Potgieter PD. Use of flexible
fiberoptic
bronchoscope in diagnosis of sputum-negative pulmonary
tuberculosis.
Thorax 1982;37:598-601.
Willcox PA, Potgieter PD, Bateman ED, Benator SR. Rapid
diagnosis of
sputum-negative miliary tuberculosis using the flexible
fiberoptic
bronchoscope. Thorax 1986;41:681-4.
Tenover FC, Crawford JT, Huebner RE, Geiter LJ, Horsburgh CR
Jr, Good
RC. The resurgence of tuberculosis: is your laboratory ready?
J Clin
Microbiol 1993;31:767-70.
Pitchenik AE, Cole C, Russell BW, et al. Tuberculosis,
atypical mycobac-
teriosis, and the acquired immunodeficiency syndrome among
Haitian and
non-Haitian patients in South Florida. Ann Intern Med
1984;101:641-5.
Maayan S, Wormser GP, Hewlett D, et al. Acquired
immunodeficiency
syndrome (AIDS) in an economically disadvantaged population.
Arch Intern
Med 1985;145:1607-12.
Klein NC, Duncanson FP, Lenox TH III, et al. Use of
mycobacterial smears
in the diagnosis of pulmonary tuberculosis in AIDS/ARC
patients. Chest
1989;95:1190-2.
Burnens AP, Vurma-Rapp U. Mixed mycobacterial cultures --
occurrence in
the clinical laboratory. Int J Med Microbiol 1989;27:85-90.
CDC. Initial therapy for tuberculosis in the era of multidrug
resistance: recommendations of the Advisory Council for the
Elimination
of Tuberculosis. MMWR 1993;42(No. RR-7).
Rabalais G, Adams G, Stover B. PPD skin test conversion in
health-care
workers after exposure to Mycobacterium tuberculosis infection
in
infants {Letter}. Lancet 1991;338:826.
Wallgren A. On contagiousness of childhood tuberculosis. Acta
Pediatr
Scand 1937;22:229-34.
Riley RL. Airborne infection. Am J Med 1974;57:466-75.
American Society of Heating, Refrigerating and
Air-Conditioning
Engineers. Chapter 7: Health facilities. In: 1991 Application
handbook.
Atlanta: American Society of Heating, Refrigerating and
Air-Conditioning
Engineers, Inc., 1991.
American Institute of Architects, Committee on Architecture
for Health.
Chapter 7: General hospital. In: Guidelines for construction
and equip-
ment of hospital and medical facilities. Washington, DC: The
American
Institute of Architects Press, 1987.
Health Resources and Services Administration. Guidelines for
construc-
tion and equipment of hospital and medical facilities.
Rockville, MD: US
Department of Health and Human Services, Public Health
Service, 1984;
PHS publication no. (HRSA)84-14500.
Riley RL, O'Grady F. Airborne infection: transmission and
control. New
York: McMillan, 1961.
Galson E, Goddard KR. Hospital air conditioning and sepsis
control.
ASHRAE Journal, 1968;(Jul):33-41.
Kethley TW. Air: its importance and control. In: Proceedings
of the
National Conference on Institutionally Acquired Infections.
Washington,
DC: US Department of Health, Education, and Welfare, Public
Health
Service, Communicable Disease Center, Division of Hospital and
Medical
Facilities, 1963:35-46; PHS publication no. 1188.
Hermans RD, Streifel AJ. Ventilation design. In: Bierbaum PJ,
Lippmann
M, eds. Proceedings of the Workshop on Engineering Controls
for
Preventing Airborne Infections in Workers in Health Care and
Related
Facilities. Cincinnati: US Department of Health and Human
Services,
Public Health Service, CDC, 1994; DHHS publication no.
(NIOSH)94-106.
American National Standards Institute. American national
standard
practices for respiratory protection. New York: American
National
Standards Institute, 1992.
NIOSH. Guide to industrial respiratory protection. Morgantown,
WV: US
Department of Health and Human Services, Public Health
Service, CDC,
1987; DHHS publication no. (NIOSH)87-116.
CDC. Recommendations for HIV testing services for inpatients
and
outpatients in acute-care hospital settings; and Technical
guidance on
HIV counseling. MMWR 1993;42(No. RR-2).
Williams WW. Guidelines for infection control in hospital
personnel.
Infect Control 1983;4(suppl):326-49.
Barrett-Connor E. The periodic chest roentgenogram for the
control of
tuberculosis in health care personnel. Am Rev Respir Dis
1980;122:153-5.
CDC/National Institutes of Health. Agent: Mycobacterium
tuberculosis, M.
bovis. In: Biosafety in microbiological and biomedical
laboratories.
Atlanta: US Department of Health and Human Services, Public
Health
Service, 1993:95; DHHS publication no. (CDC)93-8395.
CDC. Prevention and control of tuberculosis in facilities
providing
long-term care to the elderly: recommendations of the Advisory
Committee
for Elimination of Tuberculosis. MMWR 1990;39(No. RR-10).
CDC. Prevention and control of tuberculosis in correctional
institu-
tions: recommendations of the Advisory Committee for the
Elimination of
Tuberculosis. MMWR 1989;38:313-20,325.
Dueli RC, Madden RN. Droplet nuclei produced during dental
treatment of
tubercular patients. Oral Surg 1970;30:711-6.
Manoff SB, Cauthen GM, Stoneburner RL, Bloch AB, Schultz S,
Snider DE
Jr. TB patients with AIDS: are they more likely to spread TB?
{Abstract
no. 4621}. Book 2. IV International Conference on AIDS.
Stockholm,
Sweden, June 12-16, 1988:216.
Cauthen GM, Dooley SW, Bigler W, Burr J, Ihle W. Tuberculosis
(TB)
transmission by HIV-associated TB cases {Abstract no.
M.C.3326}. Vol 1.
VII International Conference on AIDS. Florence, Italy, June
16-21, 1991.
Klausner JD, Ryder RW, Baende E, et al. Mycobacterium
tuberculosis in
household contacts of human immunodeficiency virus type
1-seropositive
patients with active pulmonary tuberculosis in Kinshasa,
Zaire. J Infect
Dis 1993;168:106-11.
Riley RL, Mills CC, O'Grady F, Sultan LU, Wittstadt F,
Shivpuri DN.
Infectiousness of air from a tuberculosis ward. Am Rev Respir
Dis 1962;
85:511-25.
Noble RC. Infectiousness of pulmonary tuberculosis after
starting chemo-
therapy: review of the available data on an unresolved
question. Am J
Infect Control 1981;9:6-10.
Howard TP, Solomon DA. Reading the tuberculin skin test: who,
when, and
how? Arch Intern Med 1988;148:2457-9.
Snider DE Jr. The tuberculin skin test. Am Rev Respir Dis
1982;125:108-
18.
Huebner RE, Schein MF, Bass JB Jr. The tuberculin skin test.
Clin Infect
Dis 1993;17:968-75.
Canessa PA, Fasano L, Lavecchia MA, Torraca A, Schiattone ML.
Tuberculin
skin test in asymptomatic HIV seropositive carriers {Letter}.
Chest
1989;96:1215-6.
CDC. Purified protein derivative (PPD)-tuberculin anergy and
HIV
infection: guidelines for anergy testing and management of
anergic
persons at risk of tuberculosis. MMWR 1991;40(No. RR-5).
Snider DE, Farer LS. Package inserts for antituberculosis
drugs and
tuberculins. Am Rev Respir Dis 1985;131:809-10.
Snider DE Jr. Bacille Calmette-Guerin vaccinations and
tuberculin skin
test. JAMA 1985;253:3438-9.
CDC. Use of BCG vaccines in the control of TB: a joint
statement by the
ACIP and the Advisory Committee for the Elimination of
Tuberculosis.
MMWR 1988;37:663-4,669-75.
Thompson NJ, Glassroth JL, Snider DE Jr, Farer LS. The booster
phenomenon in serial tuberculin testing. Am Rev Respir Dis
1979;119:
587-97.
Des Prez RM, Heim CR. Mycobacterium tuberculosis. In: Mandell
GL,
Douglas RG Jr, Bennett JE, eds. Principles and practice of
infectious
diseases. 3rd ed. New York: ChurchiII Livingstone,
1990:1877-906.
Pitchenik AE, Rubinson HA. The radiographic appearance of
tuberculosis
in patients with the acquired immune deficiency syndrome
(AIDS) and pre-
AIDS. Am Rev Respir Dis 1985;131:393-6.
Kiehn TE, Cammarata R. Laboratory diagnosis of mycobacterial
infection
in patients with acquired immunodeficiency syndrome. J Clin
Microbiol
1986;24:708-11.
Crawford JT, Eisenach KD, Bates JH. Diagnosis of tuberculosis:
present
and future. Semin Respir Infect 1989;4:171-81.
Moulding TS, Redeker AG, Kanel GC. Twenty isoniazid-associated
deaths in
one state. Am Rev Respir Dis 1989;140:700-5.
Snider DE Jr, Layde PM, Johnson MW, Lyle MA. Treatment of
tuberculosis
during pregnancy. Am Rev Respir Dis 1980;122:65-79.
Snider D. Pregnancy and tuberculosis. Chest
1984;86(suppl):10S-13S.
Hamadeh MA, Glassroth J. Tuberculosis and pregnancy. Chest
1992;101:
1114-20.
Glassroth JL, White MC, Snider DE Jr. An assessment of the
possible
association of isoniazid with human cancer deaths. Am Rev
Respir Dis
1977;116:1065-74.
Glassroth JL, Snider DE Jr, Comstock GW. Urinary tract cancer
and
isoniazid. Am Rev Respir Dis 1977;116:331-3.
Costello HD, Snider DE Jr. The incidence of cancer among
participants in
a controlled, randomized isoniazid preventive therapy trial.
Am J
Epidemiol 1980;111:67-74.
CDC. The use of preventive therapy for tuberculous infection
in the
United States: recommendations of the Advisory Committee for
Elimination
of Tuberculosis. MMWR 1990;39 (No. RR-8):9-12.
CDC. Management of persons exposed to multidrug-resistant
tuberculosis.
MMWR 1992;41(No. RR-11):59-71.
American Thoracic Society/CDC. Treatment of tuberculosis and
tuber-
culosis infection in adults and children, 1986. Am Rev Respir
Dis 1986;
134:355-63.
American Thoracic Society/CDC. Control of tuberculosis in the
United
States. Am Rev Respir Dis 1992;146:1624-35.
Snider DE Jr, Caras GJ. Isoniazid-associated hepatitis deaths:
a review
of available information. Am Rev Respir Dis 1992;145:494-7.
Small PM, Shafer RW, Hopewell PC, et al. Exogenous infection
with multi-
drug-resistant Mycobacterium tuberculosis in patients with
advanced HIV
infection. N Engl J Med 1993;328:1137-44.
Goble M. Drug-resistant tuberculosis. Semin Respir Infect
1986;1:220-9.
Goble M, Iseman MD, Madsen LA, Waite D, Ackerson L, Horsburgh
CR Jr.
Treatment of 171 patients with pulmonary tuberculosis
resistant to
isoniazid and rifampin. N Engl J Med 1993;328:527-32.
Simone PM, Iseman MD. Drug-resistant tuberculosis: a deadly --
and
growing -- danger. J Respir Dis 1992;13:960-71.
American Conference of Governmental Industrial Hygienists.
Industrial
ventilation: a manual of recommended practice. Cincinnati:
American
Conference of Governmental Hygienists, Inc., 1992.
Mutchler JE. Principles of ventilation. In: NIOSH. The
industrial
environment -- its evaluation and control. Washington, DC: US
Department
of Health, Education, and Welfare, Public Health Service,
NIOSH, 1973.
Sherertz RJ, Belani A, Kramer BS, et al. Impact of air
filtration on
nosocomial Aspergillus infections. Am J Med 1987;83:709-18.
Rhame FS, Streifel AJ, Kersey JH, McGlave PB. Extrinsic risk
factors for
pneumonia in the patient at high risk of infection. Am J Med
1984;76:
42-52.
Opal SM, Asp AA, Cannady PB, Morse PL, Burton LJ, Hammer PG.
Efficacy of
infection control measures during a nosocomial outbreak of
disseminated
Aspergillus associated with hospital construction. J Infect
Dis 1986;
153:63-7.
Woods JE. Cost avoidance and productivity in owning and
operating
buildings. Occup Med 1989;4:753-70.
Woods JE, Rask DR. Heating, ventilation, air-conditioning
systems: the
engineering approach to methods of control. In: Kundsin RB,
ed. Archi-
tectural design and indoor microbial pollution. New York:
Oxford Univer-
sity Press, 1988:123-53.
American Society of Heating, Refrigerating and
Air-Conditioning
Engineers. Chapter 25: Air cleaners for particulate
contaminants. In:
1992 Systems and equipment fundamentals handbook. Atlanta:
American
Society of Heating, Refrigerating and Air-Conditioning
Engineers, Inc.,
1992:25.3-25.5.
American Society of Heating, Refrigerating and
Air-Conditioning
Engineers. Chapter 14: Air flow around buildings. In: 1989
Fundamentals
handbook. Atlanta: American Society of Heating, Refrigerating
and Air-
Conditioning Engineers, Inc., 1989:14.1-14.13.
Riley RL, Wells WF, Mills CC, Nyka W, McLean RL. Air hygiene
in tuber-
culosis: quantitative studies of infectivity and control in a
pilot
ward. Am Rev Tuberc 1957;75:420-31.
Riley RL, Nardell EA. Clearing the air: the theory and
application of UV
air disinfection. Am Rev Respir Dis 1989;139:1286-94.
Riley RL. Ultraviolet air disinfection for control of
respiratory
contagion. In: Kundsin RB, ed. Architectural design and indoor
microbial
pollution. New York: Oxford University Press, 1988:175-97.
Stead WW. Clearing the air: the theory and application of
ultraviolet
air disinfection {Letter}. Am Rev Respir Dis 1989;140:1832.
McLean RL. General discussion: the mechanism of spread of
Asian
influenza. Am Rev Respir Dis 1961;83:36-8.
Willmon TL, Hollaender A, Langmuir AD. Studies of the control
of acute
respiratory diseases among naval recruits. I. A review of a
four-year
experience with ultraviolet irradiation and dust suppressive
measures,
1943 to 1947. Am J Hyg 1948;48:227-32.
Wells WF, Wells MW, Wilder TS. The environmental control of
epidemic
contagion. I. An epidemiologic study of radiant disinfection
of air in
day schools. Am J Hyg 1942;35:97-121.
Wells WF, Holla WA. Ventilation in the flow of measles and
chickenpox
through a community: progress report, January 1, 1946 to June
15, 1949
Airborne Infection Study, Westchester County Department of
Health.
JAMA 1950;142:1337-44.
Perkins JE, Bahlke AM, Silverman HF. Effect of ultra-violet
irradiation
of classrooms on spread of measles in large rural central
schools. Am J
Public Health Nations Health 1947;37:529-37.
116. Lurie MB. Resistance to tuberculosis: experimental studies in
native and
acquired defensive mechanisms. Cambridge, MA: Harvard
University Press,
1964:160-4.
117. Collins FM. Relative susceptibility of acid-fast and
non-acid-fast
bacteria to ultraviolet light. Appl Microbiol 1971;21:411-3.
118. David HL, Jones WD Jr, Newman CM. Ultraviolet light
inactivation and
photoreactivation in the mycobacteria. Infect Immun
1971;4:318-9.
119. David HL. Response of mycobacteria to ultraviolet light
radiation. Am
Rev Respir Dis 1973;108:1175-85.
120. Riley RL, Knight M, Middlebrook G. Ultraviolet susceptibility
of BCG and
virulent tubercle bacilli. Am Rev Respir Dis 1976;113:413-8.
121. American Thoracic Society/CDC. Control of tuberculosis. Am Rev
Respir
Dis 1983;128:336-42.
122. National Tuberculosis and Respiratory Disease Association.
Guidelines
for the general hospital in the admission and care of
tuberculous
patients. Am Rev Respir Dis 1969;99:631-3.
123. CDC. Notes on air hygiene: summary of Conference on Air
Disinfection.
Arch Environ Health 1971;22:473-4.
124. Schieffelbein CW Jr, Snider DE Jr. Tuberculosis control among
homeless
populations. Arch Intern Med 1988;148:1843-6.
125. CDC. Prevention and control of tuberculosis in correctional
institu-
tions: recommendations of the Advisory Committee for the
Elimination of
Tuberculosis. MMWR 1989;38:313-20,325.
126. International Commission on Illumination. International
lighting
vocabulary {French}. 4th ed. Geneva, Switzerland: Bureau
Central de la
Commission Electrotechnique Internationale, 1987; CIE
publication no.
17.4.
127. Nagy R. Application and measurement of ultraviolet radiation.
Am Ind Hyg
York: Illuminating Engineering Society, 1966:25-7.
129. Kethley TW, Branch K. Ultraviolet lamps for room air
disinfection:
effect of sampling location and particle size of bacterial
aerosol. Arch
Environ Health 1972;25:205-14.
130. Riley RL, Permutt S, Kaufman JE. Convection, air mixing, and
ultraviolet
air disinfection in rooms. Arch Environ Health 1971;22:200-7.
131. Riley RL, Permutt S. Room air disinfection by ultraviolet
irradiation of
upper air. Arch Environ Health 1971;22:208-19.
132. Riley RL, Permutt S, Kaufman JE. Room air disinfection by
ultraviolet
irradiation of upper air: further analysis of convective air
exchange.
Arch Environ Health 1971;23:35-9.
133. Riley RL, Kaufman JE. Air disinfection in corridors by upper
air irradi-
ation with ultraviolet. Arch Environ Health 1971;22:551-3.
134. Macher JM, Alevantis LE, Chang Y-L, Liu K-S. Effect of
ultraviolet
germicidal lamps on airborne microorganisms in an outpatient
waiting
room. Applied Occupational and Environmental Hygiene
1992;7:505-13.
135. Riley RL, Kaufman JE. Effect of relative humidity on the
inactivation of
airborne Serratia marcescens by ultraviolet radiation. Appl
Microbiol
1972;23:1113-20.
136. NIOSH. Criteria for a recommended standard...occupational
exposure to
ultraviolet radiation. Washington, DC: US Department of
Health,
Education, and Welfare, Public Health Service, 1972;
publication no.
(HSM)73-110009.
137. Everett MA, Sayre RM, Olson RL. Physiologic response of human
skin to
ultraviolet light. In: Urbach F, ed. The biologic effects of
ultraviolet
radiation. Oxford, England: Pergamon Press, 1969.
138. International Agency for Research on Cancer. IARC monographs
on the
evaluation of carcinogenic risks to humans: solar and
ultraviolet
radiation. Vol 55. Lyon, France: World Health Organization,
Inter-
national Agency for Research on Cancer, 1992.
139. Valerie K, Delers A, Bruck C, et al. Activation of human
immuno-
deficiency virus type 1 by DNA damage in human cells. Nature
1988;333:
78-81.
140. Zmudzka BZ, Beer JZ. Activation of human immunodeficiency
virus by
ultraviolet radiation (yearly review). Photochem Photobiol
1990;52:
1153-62.
141. Wallace BM, Lasker JS. Awakenings...UV light and HIV gene
activation.
Science 1992;257:1211-2.
142. Valerie K, Rosenberg M. Chromatin structure implicated in
activation of
HIV-1 gene expression by ultraviolet light. New Biol
1990;2:712-8.
143. Stein B, Rahmsdorf HJ, Steffen A, Litfin M, Herrlich P.
UV-induced DNA
damage is an intermediate step in UV-induced expression of
human immuno-
deficiency virus type 1, collagenase, C-Fos, and
metallathionein. Mol
Cell Biol 1989;9:5169-81.
144. Clerici M, Shearer GM. UV light exposure and HIV replication.
Science
1992;258:1070-1.
145. NIOSH. Hazard evaluation and technical assistance report:
Onondaga
County Medical Examiner's Office, Syracuse, New York.
Cincinnati: US
Department of Health and Human Services, Public Health
Service, CDC,
1992; NIOSH report no. HETA 92-171-2255.
146. NIOSH. Hazard evaluation and technical assistance report: John
C. Murphy
Family Health Center, Berkeley, Missouri. Cincinnati: US
Department of
Health and Human Services, Public Health Service, CDC, 1992;
NIOSH
report no. HETA 91-148-2236.
147. NIOSH. Hazard evaluation and technical assistance report: San
Francisco
General Hospital and Medical Center, San Francisco,
California.
Cincinnati: US Department of Health and Human Services, Public
Health
Service, CDC, 1992; NIOSH report no. HETA 90-122-L2073.
148. Macher JM. Ultraviolet radiation and ventilation to help
control tuber-
culosis transmission: guidelines prepared for California
Indoor Air
Quality Program. Berkeley, CA: Air and Industrial Hygiene
Laboratory,
1989.
149. Riley RL. Principles of UV air disinfection. Baltimore, MD:
Johns
Hopkins University, School of Hygiene and Public Health, 1991.
150. American Conference of Governmental Industrial Hygienists.
Threshold
limit values and biological exposure indices for 1991-1992.
Cincinnati:
American Conference of Governmental Industrial Hygienists,
Inc., 1991.
151. Bloom BR, Murray CJL. Tuberculosis: commentary on a reemergent
killer.
Science 1992;257:1055-64.
152. Nardell EA. Dodging droplet nuclei: reducing the probability
of noso-
comial tuberculosis transmission in the AIDS era. Am Rev
Respir Dis
1990;142:501-3.
153. US Department of Health and Human Services. 42 CFR Part 84:
Respiratory
protective devices; proposed rule. Federal Register
1994;59:26849-89.
154. American National Standards Institute. ANSI Z88.2-1980:
American
national standard practices for respiratory protection. New
York:
American National Standards Institute, 1980.
155. Hyatt EC. Current problems and new developments in respiratory
protection. Am Ind Hyg Assoc J 1963;24:295-304.
156. American National Standards Institute. ANSI Z88.2-1969:
American
national standard practices for respiratory protection. New
York:
American National Standards Institute, 1969.
157. Lowry PL, Hesch PR, Revoir WH. Performance of single-use
respirators. Am
Ind Hyg Assoc J 1977;38:462-7.
158. Hyatt EC, et al. Respiratory studies for the National
Institute for
Occupational Safety and Health -- July 1, 1972, through June
3, 1973.
Los Alamos, NM: Los Alamos Scientific Laboratory; progress
report no.
LA-5620-PR.
159. Nelson KE, Larson PA, Schraufnagel DE, Jackson J. Transmission
of tuber-
culosis by fiber bronchoscopes. Am Rev Respir Dis
1983;127:97-100.
160. Leers WD. Disinfecting endoscopes: how not to transmit
Mycobacterium
tuberculosis by bronchoscopy. Can Med Assoc J 1980;123:275-83.
161. Garner JS, Simmons BP. Guideline for isolation precautions in
hospitals.
Infect Control 1983;4(suppl):245-325.
162. Rutala WA. APIC guidelines for selection and use of
disinfectants. Am J
Infect Control 1990;18:99-117.
163. Favero MS, Bond WW. Chemical disinfection of medical and
surgical
materials. In: Block SS, ed. Disinfection, sterilization, and
preser-
vation. 4th ed. Philadelphia: Lea & Fabiger, 1991:617-41.
164. Garner JS, Favero MS. Guideline for handwashing and hospital
environ-
mental control. Atlanta: US Department of Health and Human
Services,
Public Health Service, CDC, 1985.
CDC. Guidelines for Preventing the Transmission of Tuberculosis
in Health-
Care Facilities, with Special Focus on HIV-Related Issues. MMWR
1990;39(No.
RR-17).
** Area: a structural unit (e.g., a hospital ward or laboratory) or
func-
tional unit (e.g., an internal medicine service) in which HCWs
provide
services to and share air with a specific patient population or
work with
clinical specimens that may contain viable M. tuberculosis
organisms. The
risk for exposure to M. tuberculosis in a given area depends on the
preva-
lence of TB in the population served and the characteristics of the
environ-
ment.
*** Cluster: two or more PPD skin-test conversions occurring within
a 3-month
period among HCWs in a specific area or occupational group, and
epidemiologic
evidence suggests occupational (nosocomial) transmission.
**** Surgical masks are designed to prevent the respiratory
secretions of the
person wearing the mask from entering the air. When not in a TB
isolation
room, patients suspected of having TB should wear surgical masks to
reduce
the expulsion of droplet nuclei into the air. These patients do not
need to
wear particulate respirators, which are designed to filter the air
before it
is inhaled by the person wearing the mask. Patients suspected of
having or
known to have TB should never wear a respirator that has an
exhalation valve,
because the device would provide no barrier to the expulsion of
droplet
nuclei into the air.
***** Some filters become more efficient as they become loaded with
dust.
Health-care settings do not have enough dust in the air to load a
filter on
a respirator. Therefore, the filter efficiency for respirators used
in
health-care settings must be determined in the unloaded state.
****** Americans With Disabilities Act of 1990. PL 101-336, 42
U.S.C. 12101
et seq.
******* The Ryan White Comprehensive AIDS Resource Emergency Act of
1990,
P.L. 101-381, mandates notification of EMS personnel after they
have been
exposed to infectious pulmonary TB (42 U.S.C. &00ff-82.54 Fed. Reg.
13417
{March 21, 1994}).
******** Negative is defined relative to the air pressure in the
area from
which air is to flow.
********* Ordinary glass (not quartz) is sufficient to filter out
UV
radiation.
********** 29 CFR Part 1910.134.
Glossary
This glossary contains many of the terms used in the guidelines, as
well as
others that are encountered frequently by persons who implement TB
infection-
control programs. The definitions given are not dictionary
definitions but
are those most applicable to usage relating to TB.
Acid-fast bacilli (AFB): Bacteria that retain certain dyes after
being washed
in an acid solution. Most acid-fast organisms are
mycobacteria. When AFB
are seen on a stained smear of sputum or other clinical
specimen, a
diagnosis of TB should be suspected; however, the diagnosis of
TB is not
confirmed until a culture is grown and identified as M.
tuberculosis.
Adherence: Refers to the behavior of patients when they follow all
aspects of
the treatment regimen as prescribed by the medical provider,
and also
refers to the behavior of HCWs and employers when they follow
all
guidelines pertaining to infection control.
Aerosol: The droplet nuclei that are expelled by an infectious
person (e.g.,
by coughing or sneezing); these droplet nuclei can remain
suspended in
the air and can transmit M. tuberculosis to other persons.
AIA: The American Institute of Architects, a professional body that
develops
standards for building ventilation.
Air changes: The ratio of the volume of air flowing through a space
in a
certain period of time (i.e., the airflow rate) to the volume
of that
space (i.e., the room volume); this ratio is usually expressed
as the
number of air changes per hour (ACH).
Air mixing: The degree to which air supplied to a room mixes with
the air
already in the room, usually expressed as a mixing factor.
This factor
varies from 1 (for perfect mixing) to 10 (for poor mixing),
and it is
used as a multiplier to determine the actual airflow required
(i.e., the
recommended ACH multiplied by the mixing factor equals the
actual ACH
required).
Alveoli: The small air sacs in the lungs that lie at the end of the
bronchial
tree; the site where carbon dioxide in the blood is replaced
by oxygen
from the lungs and where TB infection usually begins.
Anergy: The inability of a person to react to skin-test antigens
(even if the
person is infected with the organisms tested) because of
immunosuppres-
sion.
Anteroom: A small room leading from a corridor into an isolation
room; this
room can act as an airlock, preventing the escape of
contaminants from
the isolation room into the corridor.
Area: A structural unit (e.g., a hospital ward or laboratory) or
functional
unit (e.g., an internal medicine service) in which HCWs
provide services
to and share air with a specific patient population or work
with
clinical specimens that may contain viable M. tuberculosis
organisms.
The risk for exposure to M. tuberculosis in a given area
depends on the
prevalence of TB in the population served and the
characteristics of the
environment.
ASHRAE: The American Society of Heating, Refrigerating and
Air-Conditioning
Engineers, Inc., a professional body that develops standards
for
building ventilation.
Asymptomatic: Without symptoms, or producing no symptoms.
Bacillus of Calmette and Gu,rin (BCG) vaccine: A TB vaccine used in
many
parts of the world.
BACTEC (R): One of the most often used radiometric methods for
detecting
the early growth of mycobacteria in culture. It provides rapid
growth
(in 7-14 days) and rapid drug-susceptibility testing (in 5-6
days). When
BACTEC (R) is used with rapid species identification methods,
M. tuber-
culosis can be identified within 10-14 days of specimen
collection.
Booster phenomenon: A phenomenon in which some persons (especially
older
adults) who are skin tested many years after infection with M.
tuber-
culosis have a negative reaction to an initial skin test,
followed by a
positive reaction to a subsequent skin test. The second (i.e.,
positive)
reaction is caused by a boosted immune response. Two-step
testing is
used to distinguish new infections from boosted reactions (see
Two-step
testing).
Bronchoscopy: A procedure for examining the respiratory tract that
requires
inserting an instrument (a bronchoscope) through the mouth or
nose and
into the trachea. The procedure can be used to obtain
diagnostic
specimens.
Capreomycin: An injectable, second-line anti-TB drug used primarily
for the
treatment of drug-resistant TB.
Cavity: A hole in the lung resulting from the destruction of
pulmonary tissue
by TB or other pulmonary infections or conditions. TB patients
who have
cavities in their lungs are referred to as having cavitary
disease, and
they are often more infectious than TB patients without
cavitary
disease.
Chemotherapy: Treatment of an infection or disease by means of oral
or
injectable drugs.
Cluster: Two or more PPD skin-test conversions occurring within a
3-month
period among HCWs in a specific area or occupational group,
and epidemi-
ologic evidence suggests occupational (nosocomial)
transmission.
Contact: A person who has shared the same air with a person who has
infec-
tious TB for a sufficient amount of time to allow possible
transmission
of M. tuberculosis.
Conversion, PPD: See PPD test conversion.
Culture: The process of growing bacteria in the laboratory so that
organisms
can be identified.
Cycloserine: A second-line, oral anti-TB drug used primarily for
treating
drug-resistant TB.
Directly observed therapy (DOT): An adherence-enhancing strategy in
which an
HCW or other designated person watches the patient swallow
each dose of
medication.
DNA probe: A technique that allows rapid and precise identification
of myco-
bacteria (e.g., M. tuberculosis and M. bovis) that are grown
in culture.
The identification can often be completed in 2 hours.
Droplet nuclei: Microscopic particles (i.e., 1-5 mm in diameter)
produced
when a person coughs, sneezes, shouts, or sings. The droplets
produced
by an infectious TB patient can carry tubercle bacilli and can
remain
suspended in the air for prolonged periods of time and be
carried on
normal air currents in the room.
Drug resistance, acquired: A resistance to one or more anti-TB
drugs that
develops while a patient is receiving therapy and which
usually results
from the patient's nonadherence to therapy or the prescription
of an
inadequate regimen by a health-care provider.
Drug resistance, primary: A resistance to one or more anti-TB drugs
that
exists before a patient is treated with the drug(s). Primary
resistance
occurs in persons exposed to and infected with a
drug-resistant strain
of M. tuberculosis.
Drug-susceptibility pattern: The anti-TB drugs to which the
tubercle bacilli
cultured from a TB patient are susceptible or resistant based
on drug-
susceptibility tests.
Drug-susceptibility tests: Laboratory tests that determine whether
the
tubercle bacilli cultured from a patient are susceptible or
resistant to
various anti-TB drugs.
Ethambutol: A first-line, oral anti-TB drug sometimes used
concomitantly with
INH, rifampin, and pyrazinamide.
Ethionamide: A second-line, oral anti-TB drug used primarily for
treating
drug-resistant TB.
Exposure: The condition of being subjected to something (e.g.,
infectious
agents) that could have a harmful effect. A person exposed to
M. tuber-
culosis does not necessarily become infected (see
Transmission).
First-line drugs: The most often used anti-TB drugs (i.e., INH,
rifampin,
pyrazinamide, ethambutol, and streptomycin).
Fixed room-air HEPA recirculation systems: Nonmobile devices or
systems that
remove airborne contaminants by recirculating air through a
HEPA filter.
These may be built into the room and permanently ducted or may
be
mounted to the wall or ceiling within the room. In either
situation,
they are fixed in place and are not easily movable.
Fluorochrome stain: A technique for staining a clinical specimen
with
fluorescent dyes to perform a microscopic examination (smear)
for myco-
bacteria. This technique is preferable to other staining
techniques
because the mycobacteria can be seen easily and the slides can
be read
quickly.
Fomites: Linens, books, dishes, or other objects used or touched by
a
patient. These objects are not involved in the transmission of
M. tuber-
culosis.
Gastric aspirate: A procedure sometimes used to obtain a specimen
for culture
when a patient cannot cough up adequate sputum. A tube is
inserted
through the mouth or nose and into the stomach to recover
sputum that
was coughed into the throat and then swallowed. This procedure
is
particularly useful for diagnosis in children, who are often
unable to
cough up sputum.
High-efficiency particulate air (HEPA) filter: A specialized filter
that is
capable of removing 99.97% of particles 30.3 mm in diameter
and that may
assist in controlling the transmission of M. tuberculosis.
Filters may
be used in ventilation systems to remove particles from the
air or in
personal respirators to filter air before it is inhaled by the
person
wearing the respirator. The use of HEPA filters in ventilation
systems
requires expertise in installation and maintenance.
Human immunodeficiency virus (HIV) infection: Infection with the
virus that
causes acquired immunodeficiency syndrome (AIDS). HIV
infection is the
most important risk factor for the progression of latent TB
infection to
active TB.
Immunosuppressed: A condition in which the immune system is not
functioning
normally (e.g., severe cellular immunosuppression resulting
from HIV
infection or immunosuppressive therapy). Immunosuppressed
persons are at
greatly increased risk for developing active TB after they
have been
infected with M. tuberculosis. No data are available regarding
whether
these persons are also at increased risk for infection with M.
tuber-
culosis after they have been exposed to the organism.
Induration: An area of swelling produced by an immune response to
an antigen.
In tuberculin skin testing or anergy testing, the diameter of
the
indurated area is measured 48-72 hours after the injection,
and the
result is recorded in millimeters.
Infection: The condition in which organisms capable of causing
disease (e.g.,
M. tuberculosis) enter the body and elicit a response from the
host' s
immune defenses. TB infection may or may not lead to clinical
disease.
Infectious: Capable of transmitting infection. When persons who
have
clinically active pulmonary or laryngeal TB disease cough or
sneeze,
they can expel droplets containing M. tuberculosis into the
air. Persons
whose sputum smears are positive for AFB are probably
infectious.
Injectable: A medication that is usually administered by injection
into the
muscle (intramuscular {IM}) or the bloodstream (intravenous
{IV}).
Intermittent therapy: Therapy administered either two or three
times per
week, rather than daily. Intermittent therapy should be
administered
only under the direct supervision of an HCW or other
designated person
(see Directly observed therapy {DOT}).
Intradermal: Within the layers of the skin.
Isoniazid (INH): A first-line, oral drug used either alone as
preventive
therapy or in combination with several other drugs to treat TB
disease.
Kanamycin: An injectable, second-line anti-TB drug used primarily
for treat-
ment of drug-resistant TB.
Latent TB infection: Infection with M. tuberculosis, usually
detected by a
positive PPD skin-test result, in a person who has no symptoms
of active
TB and who is not infectious.
Mantoux test: A method of skin testing that is performed by
injecting 0.1 mL
of PPD-tuberculin containing 5 tuberculin units into the
dermis (i.e.,
the second layer of skin) of the forearm with a needle and
syringe. This
test is the most reliable and standardized technique for
tuberculin
testing (see Tuberculin skin test and Purified protein
derivative {PPD}-
tuberculin test).
Multidrug-resistant tuberculosis (MDR-TB): Active TB caused by M.
tuber-
culosis organisms that are resistant to more than one anti-TB
drug; in
practice, often refers to organisms that are resistant to both
INH and
rifampin with or without resistance to other drugs (see Drug
resistance,
acquired and Drug resistance, primary).
M. tuberculosis complex: A group of closely related mycobacterial
species
that can cause active TB (e.g., M. tuberculosis, M. bovis, and
M.
africanum); most TB in the United States is caused by M.
tuberculosis.
Negative pressure: The relative air pressure difference between two
areas in
a health-care facility. A room that is at negative pressure
has a lower
pressure than adjacent areas, which keeps air from flowing out
of the
room and into adjacent rooms or areas.
Nosocomial: An occurrence, usually an infection, that is acquired
in a
hospital or as a result of medical care.
Para-aminosalicylic acid: A second-line, oral anti-TB drug used for
treating
drug-resistant TB.
Pathogenesis: The pathologic, physiologic, or biochemical process
by which a
disease develops.
Pathogenicity: The quality of producing or the ability to produce
pathologic
changes or disease. Some nontuberculous mycobacteria are
pathogenic
(e.g., Mycobacterium kansasii), and others are not (e.g.,
Mycobacterium
phlei).
that remove airborne contaminants by recirculating air through
a HEPA
filter.
Positive PPD reaction: A reaction to the purified protein
derivative (PPD)-
tuberculin skin test that suggests the person tested is
infected with M.
tuberculosis. The person interpreting the skin-test reaction
determines
whether it is positive on the basis of the size of the
induration and
the medical history and risk factors of the person being
tested.
Preventive therapy: Treatment of latent TB infection used to
prevent the
progression of latent infection to clinically active disease.
Purified protein derivative (PPD)-tuberculin: A purified tuberculin
prepar-
ation that was developed in the 1930s and that was derived
from old
tuberculin. The standard Mantoux test uses 0.1 mL of PPD
standardized to
5 tuberculin units.
Purified protein derivative (PPD)-tuberculin test: A method used to
evaluate
the likelihood that a person is infected with M. tuberculosis.
A small
dose of tuberculin (PPD) is injected just beneath the surface
of the
skin, and the area is examined 48-72 hours after the
injection. A
reaction is measured according to the size of the induration.
The
classification of a reaction as positive or negative depends
on the
patient's medical history and various risk factors (see
Mantoux test).
Purified protein derivative (PPD)-tuberculin test conversion: A
change in PPD
test results from negative to positive. A conversion within a
2-year
period is usually interpreted as new M. tuberculosis
infection, which
carries an increased risk for progression to active disease. A
booster
reaction may be misinterpreted as a new infection (see Booster
phenomenon and Two-step testing).
Pyrazinamide: A first-line, oral anti-TB drug used in treatment
regimens.
Radiography: A method of viewing the respiratory system by using
radiation to
transmit an image of the respiratory system to film. A chest
radiograph
is taken to view the respiratory system of a person who is
being
evaluated for pulmonary TB. Abnormalities (e.g., lesions or
cavities in
the lungs and enlarged lymph nodes) may indicate the presence
of TB.
Radiometric method: A method for culturing a specimen that allows
for rapid
detection of bacterial growth by measuring production of CO2
by viable
organisms; also a method of rapidly performing susceptibility
testing of
M. tuberculosis.
Recirculation: Ventilation in which all or most of the air that is
exhausted
from an area is returned to the same area or other areas of
the
facility.
Regimen: Any particular TB treatment plan that specifies which
drugs are
used, in what doses, according to what schedule, and for how
long.
Registry: A record-keeping method for collecting clinical,
laboratory, and
radiographic data concerning TB patients so that the data can
be
organized and made available for epidemiologic study.
Resistance: The ability of some strains of bacteria, including M.
tuber-
culosis, to grow and multiply in the presence of certain drugs
that
ordinarily kill them; such strains are referred to as
drug-resistant
strains.
Rifampin: A first-line, oral anti-TB drug that, when used
concomitantly with
INH and pyrazinamide, provides the basis for short-course
therapy.
Room-air HEPA recirculation systems and units: Devices (either
fixed or
portable) that remove airborne contaminants by recirculating
air through
a HEPA filter.
Second-line drugs: Anti-TB drugs used when the first-line drugs
cannot be
used (e.g., for drug-resistant TB or because of adverse
reactions to the
first-line drugs). Examples are cycloserine, ethionamide, and
capreomycin.
Single-pass ventilation: Ventilation in which 100% of the air
supplied to an
area is exhausted to the outside.
Smear (AFB smear): A laboratory technique for visualizing
mycobacteria. The
specimen is smeared onto a slide and stained, then examined
using a
microscope. Smear results should be available within 24 hours.
In TB, a
large number of myco-bacteria seen on an AFB smear usually
indicates
infectiousness. However, a positive result is not diagnostic
of TB
because organisms other than M. tuberculosis may be seen on an
AFB smear
(e.g., nontuberculous mycobacteria).
Source case: A case of TB in an infectious person who has
transmitted M.
tuberculosis to another person or persons.
Source control: Controlling a contaminant at the source of its
generation,
which prevents the spread of the contaminant to the general
work space.
Specimen: Any body fluid, secretion, or tissue sent to a laboratory
where
smears and cultures for M. tuberculosis will be performed
(e.g., sputum,
urine, spinal fluid, and material obtained at biopsy).
Sputum: Phlegm coughed up from deep within the lungs. If a patient
has
pulmonary disease, an examination of the sputum by smear and
culture can
be helpful in evaluating the organism responsible for the
infection.
Sputum should not be confused with saliva or nasal secretions.
Sputum induction: A method used to obtain sputum from a patient who
is unable
to cough up a specimen spontaneously. The patient inhales a
saline mist,
which stimulates a cough from deep within the lungs.
Sputum smear, positive: AFB are visible on the sputum smear when
viewed under
a microscope. Persons with a sputum smear positive for AFB are
considered more infectious than those with smear-negative
sputum.
Streptomycin: A first-line, injectable anti-TB drug.
Symptomatic: Having symptoms that may indicate the presence of TB
or another
disease (see Asymptomatic).
TB case: A particular episode of clinically active TB. This term
should be
used only to refer to the disease itself, not the patient with
the
disease. By law, cases of TB must be reported to the local
health
department.
TB infection: A condition in which living tubercle bacilli are
present in the
body but the disease is not clinically active. Infected
persons usually
have positive tuberculin reactions, but they have no symptoms
related to
the infection and are not infectious. However, infected
persons remain
at lifelong risk for developing disease unless preventive
therapy is
given.
Transmission: The spread of an infectious agent from one person to
another.
The likelihood of transmission is directly related to the
duration and
intensity of exposure to M. tuberculosis (see Exposure).
Treatment failures: TB disease in patients who do not respond to
chemotherapy
and in patients whose disease worsens after having improved
initially.
Tubercle bacilli: M. tuberculosis organisms.
Tuberculin skin test: A method used to evaluate the likelihood that
a person
is infected with M. tuberculosis. A small dose of
PPD-tuberculin is
injected just beneath the surface of the skin, and the area is
examined
48-72 hours after the injection. A reaction is measured
according to the
size of the induration. The classification of a reaction as
positive or
negative depends on the patient's medical history and various
risk
factors (see Mantoux test, PPD test).
Tuberculosis (TB): A clinically active, symptomatic disease caused
by an
organism in the M. tuberculosis complex (usually M.
tuberculosis or,
rarely, M. bovis or M. africanum).
Two-step testing: A procedure used for the baseline testing of
persons who
will periodically receive tuberculin skin tests (e.g., HCWs)
to reduce
the likelihood of mistaking a boosted reaction for a new
infection. If
the initial tuberculin-test result is classified as negative,
a second
test is repeated 1-3 weeks later. If the reaction to the
second test is
positive, it probably represents a boosted reaction. If the
second test
result is also negative, the person is classified as not
infected. A
positive reaction to a subsequent test would indicate new
infection
(i.e., a skin-test conversion) in such a person.
Ultraviolet germicidal irradiation (UVGI): The use of ultraviolet
radiation
to kill or inactivate microorganisms.
Ultraviolet germicidal irradiation (UVGI) lamps: Lamps that kill or
inactivate microorganisms by emitting ultraviolet germicidal
radiation,
predominantly at a wavelength of 254 nm (intermediate light
waves
between visible light and X-rays). UVGI lamps can be used in
ceiling or
wall fixtures or within air ducts of ventilation systems.
Ventilation, dilution: An engineering control technique to dilute
and remove
airborne contaminants by the flow of air into and out of an
area. Air
that contains droplet nuclei is removed and replaced by
contaminant-free
air. If the flow is sufficient, droplet nuclei become
dispersed, and
their concentration in the air is diminished.
Ventilation, local exhaust: Ventilation used to capture and remove
airborne
contaminants by enclosing the contaminant source (i.e., the
patient) or
by placing an exhaust hood close to the contaminant source.
Virulence: The degree of pathogenicity of a microorganism as
indicated by the
severity of the disease produced and its ability to invade the
tissues
of a host. M. tuberculosis is a virulent organism.
Table_1 Note:
To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 1. Elements of a risk assessment for tuberculosis (TB) in health-care facilities
-------------------------------------------------------------------------------------------
1. Review the community TB profile (from public health department data).
2. Review the number of TB patients who were treated in each area of the facility (both
inpatient and outpatient). (This information can be obtained by analyzing laboratory
surveillance data and by reviewing discharge diagnoses or medical and infection-
control records.)
3. Review the drug-susceptibility patterns of TB isolates of patients who were treated at
the facility.
4. Analyze purified protein derivative (PPD)-tuberculin skin-test results of health-care
workers (HCWs), by area or by occupational group for HCWs not assigned to a specific
area (e.g., respiratory therapists).
5. To evaluate infection-control parameters, review medical records of a sample of TB
patients seen at the facility.
Calculate intervals from:
- admission until TB suspected;
- admission until TB evaluation performed;
- admission until acid-fast bacilli (AFB) specimens ordered;
- AFB specimens ordered until AFB specimens collected;
- AFB specimens collected until AFB smears performed and reported;
- AFB specimens collected until cultures performed and reported;
- AFB specimens collected until species identification conducted and reported;
- AFB specimens collected until drug-susceptibility tests performed and reported;
- admission until TB isolation initiated;
- admission until TB treatment initiated; and
- duration of TB isolation.
Obtain the following additional information:
- Were appropriate criteria used for discontinuing isolation?
- Did the patient have a history of prior admission to the facility?
- Was the TB treatment regimen adequate?
- Were follow-up sputum specimens collected properly?
- Was appropriate discharge planning conducted?
6. Perform an observational review of TB infection control practices.
7. Review the most recent environmental evaluation and maintenance procedures.
-------------------------------------------------------------------------------------------
Table_2 Note:
To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 2. Elements of a tuberculosis (TB) infection-control program
=================================================================================================================================================
Risk categories
-----------------------------------------------------------------------------
Element Minimal Very low Low Intermediate High
----------------------------------------------------------------------------------------------------------------------------------
Assigning responsibility (Section II.A)
Designated TB control officer or committee R R R R R
Conducting a risk assessment
(Section II.B.1)
Baseline risk assessment R R R R R
Community TB profile: incidence,
prevalence, and drug-susceptibility
patterns Y Y Y Y Y
Facility case surveillance (laboratory-
and discharge-diagnosis-based) C C C C C
Analysis of purified protein derivative
(PPD) test results among health-care
workers (HCWs) N/A V * Y every 6-12 mos every 3 mos
Review of TB patient medical records N/A O + Y every 6-12 mos every 3 mos
Observation of infection-control practices N/A N/A Y every 6-12 mos every 3 mos
Evaluation of engineering control
maintenance O & O & Y every 6-12 mos every 3 mos
Developing a TB infection control plan
(Section II.B.2)
Written TB infection control plan R R R R R
Periodically reassessing risk
(Section II.B.3)
Reassessment of risk Y Y Y every 6-12 mos every 3 mos
Identifying, evaluating, and initiating
treatment for patients who may have
active TB (Section II.C)
Protocol (clinical prediction rules) @ for
identifying patients who may have
active TB R R R R R
Protocol for diagnostic evaluation of
patients who may have active TB ** N/A R R R R
Protocol for reporting laboratory results
to clinicians, infection-control
practitioners, collaborating referral
facilities, and appropriate health
department(s) N/A R R R R
Protocol for initiating treatment of
patients who may have active TB ** N/A R R R R
Managing patients who may have TB in
ambulatory-care settings and emergency
departments (Section II.D)
Triage system for identifying patients
who have active TB in emergency
departments and ambulatory-care
settings R R R R R
Protocol for managing patients who may
have active TB in emergency
departments and ambulatory-care
settings R R R R R
Protocol for referring patients who may
have active TB to collaborating facility R R N/A ++ N/A ++ N/A ++
Managing hospitalized patients who may
have TB (Section II.E)
Appropriate number of TB isolation
rooms && N/A N/A R R R
Protocol for initiating TB isolation N/A N/A R R R
Protocol for TB isolation practices N/A N/A R R R
Protocol for discontinuing TB isolation N/A N/A R R R
Protocol for discharge planning N/A N/A R R R
Engineering controls (Suppl. 3, Section II.F)
Protocol(s) for maintenance of
engineering controls O & O & R R R
Respiratory protection (Suppl. 4,
Section II.G)
Respiratory protection program N/A V * R R R
Cough-inducing and aerosol-generating
procedures (Section II.H)
Protocol(s) for performing cough-
inducing or aerosol-generating
procedures O O @@ R R R
Engineering controls for performing
cough-inducing or aerosol-generating
procedures O & O @@ R R R
Educating and Training HCWs
(Section II.I)
Educating and training HCWs regarding
TB R R R R R
Counseling and screening HCWs
(Section II.J)
Counseling HCWs regarding TB R R R R R
Protocol for identifying and evaluating
HCWs who have signs or symptoms of
active TB R R R R R
Baseline PPD testing of HCWs O *** R R R R
Routine periodic PPD screening of HCWs
for latent TB infection N/A V * Y every 6-12 mos every 3 mos
Protocol for evaluating and managing
HCWs who have positive PPD tests R R R R R
Protocol for managing HCWs who have
active TB R R R R R
Conducting a problem evaluation
(Section II.K)
Protocol for investigating PPD
conversions and active TB in HCWs R R R R R
Protocol for investigating possible
patient-to-patient transmission of
Mycobacterium tuberculosis R R R R R
Protocol for investigating possible
contacts of TB patients who were not
diagnosed initially as having TB and
were not placed in isolation R R R R R
Coordination with the public health
department (Section II.L)
Effective system for reporting patients
who have suspected or confirmed TB
to appropriate health department(s) R R R R R
R=recommended; Y=yearly; C=continual; N/A=not applicable; O=optional; V=variable.
----------------------------------------------------------------------------------------------------------------------------------
* Because very low-risk facilities do not admit patients who may have active TB to inpatient areas, most HCWs in such facilities do
not need routine follow-up PPD screening after baseline PPD testing is done. However, those who are involved in the initial
assessment and diagnostic evaluation of patients in the ambulatory-care, emergency, and admitting departments of such facilities
or in the outpatient management of patients with active TB could be exposed potentially to a patient who has active TB. These
HCWs may need to receive routine periodic PPD screening. Similarly, these HCWs may need to be included in a respiratory protection
program.
+ Because very low-risk facilities do not admit patients suspected of having active TB, review of TB patient medical records is not
applicable. However, follow-up of patients who were identified during triage as possibly having active TB and referred to another
institution for further evaluation and management may be useful in evaluating the effectiveness of the triage system.
& Some minimal or very low-risk facilities may elect to use engineering controls (e.g., booths for cough-inducing procedures, portable
high-efficiency particulate {HEPA} filtration units, ultraviolet germicidal irradiation units) in triage/waiting areas. In such situations,
appropriate protocols for maintaining this equipment should be in place, and this maintenance should be evaluated periodically.
@ The criteria used in clinical prediction rules will probably vary from facility to facility depending on the prevalence of TB in the
population served by the facility and on the clinical, radiographic, and laboratory characteristics of TB patients examined in the
facility.
** The protocols should be consistent with CDC/American Thoracic Society recommendations (33).
++ Protocols for referring patients who require specialized treatment (e.g., patients with multidrug-resistant TB) may be appropriate.
&& Based on maximum daily number of patients requiring TB isolation for suspected or confirmed active TB. Isolation rooms should
meet the performance criteria specified in these guidelines.
@@ If such procedures are used in the triage protocol(s) for identifying patients who may have active TB.
*** Minimal-risk facilities do not need to maintain an ongoing PPD skin-testing program. However, baseline PPD testing of HCWs may
be advisable so that if an unexpected exposure does occur, conversions can be distinguished from positive PPD test results caused
by previous exposures.
=================================================================================================================================================
Table_3 Note:
To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 3. Characteristics of an effective tuberculosis (TB) infection-control program *
=================================================================================================
-----------------------------------------------------------------------------------------------
I. Assignment of responsibility
A. Assign responsibility for the TB infection-control program to qualified person(s).
B. Ensure that persons with expertise in infection control, occupational health, and
engineering are identified and included.
II. Risk assessment, TB infection-control plan, and periodic reassessment
A. Initial risk assessments
1. Obtain information concerning TB in the community.
2. Evaluate data concerning TB patients in the facility.
3. Evaluate data concerning purified protein derivative (PPD)-tuberculin skin-test
conversions among health-care workers (HCWs) in the facility.
4. Rule out evidence of person-to-person transmission.
B. Written TB infection-control program
1. Select initial risk protocol(s).
2. Develop written TB infection-control protocols.
C. Repeat risk assessment at appropriate intervals.
1. Review current community and facility surveillance data and PPD-tuberculin
skin-test results.
2. Review records of TB patients.
3. Observe HCW infection-control practices.
4. Evaluate maintenance of engineering controls.
III. Identification, evaluation, and treatment of patients who have TB
A. Screen patients for signs and symptoms of active TB:
1. On initial encounter in emergency department or ambulatory-care setting.
2. Before or at the time of admission.
B. Perform radiologic and bacteriologic evaluation of patients who have signs and
symptoms suggestive of TB.
C. Promptly initiate treatment.
IV. Managing outpatients who have possible infectious TB
A. Promptly initiate TB precautions.
B. Place patients in separate waiting areas or TB isolation rooms.
C. Give patients a surgical mask, a box of tissues, and instructions regarding the use
of these items.
V. Managing inpatients who have possible infectious TB
A. Promptly isolate patients who have suspected or known infectious TB.
B. Monitor the response to treatment.
C. Follow appropriate criteria for discontinuing isolation.
VI. Engineering recommendations
A. Design local exhaust and general ventilation in collaboration with persons who
have expertise in ventilation engineering.
B. Use a single-pass air system or air recirculation after high-efficiency particulate air
(HEPA) filtration in areas where infectious TB patients receive care.
C. Use additional measures, if needed, in areas where TB patients may receive care.
D. Design TB isolation rooms in health-care facilities to achieve greater than or
equal to 6 air changes per hour (ACH) for existing facilities and greater than
or equal to 12 ACH for new or renovated facilities.
E. Regularly monitor and maintain engineering controls.
F. TB isolation rooms that are being used should be monitored daily to ensure they
maintain negative pressure relative to the hallway and all surrounding areas.
G. Exhaust TB isolation room air to outside or, if absolutely unavoidable, recirculate
after HEPA filtration.
VII. Respiratory protection
A. Respiratory protective devices should meet recommended performance criteria.
B. Repiratory protection should be used by persons entering rooms in which
patients with known or suspected infectious TB are being isolated, by HCWs when
performing cough-inducing or aerosol-generating procedures on such patients,
and by persons in other settings where administrative and engineering controls
are not likely to protect them from inhaling infectious airborne droplet nuclei.
C. A respiratory protection program is required at all facilities in which respiratory
protection is used.
VIII. Cough-inducing procedures
A. Do not perform such procedures on TB patients unless absolutely necessary.
B. Perform such procedures in areas that have local exhaust ventilation devices
(e.g., booths or special enclosures) or, if this is not feasible, in a room that meets
the ventilation requirements for TB isolation.
C. After completion of procedures, TB patients should remain in the booth or special
enclosure until their coughing subsides.
IX. HCW TB training and education
A. All HCWs should receive periodic TB education appropriate for their work respon-
sibilities and duties.
B. Training should include the epidemiology of TB in the facility.
C. TB education should emphasize concepts of the pathogenesis of and occupational
risk for TB.
D. Training should describe work practices that reduce the likelihood of transmitting
M. tuberculosis.
X. HCW counseling and screening
A. Counsel all HCWs regarding TB and TB infection.
B. Counsel all HCWs about the increased risk to immunocompromised persons for
developing active TB.
C. Perform PPD skin tests on HCWs at the beginning of their employment, and re-
peat PPD tests at periodic intervals.
D. Evaluate symptomatic HCWs for active TB.
XI. Evaluate HCW PPD test conversions and possible nosocomial transmission of
M. tuberculosis.
XII. Coordinate efforts with public health department(s)
-----------------------------------------------------------------------------------------------
* A program such as this is appropriate for health-care facilities in which there is a high risk
for transmission of Mycobacterium tuberculosis.
==================================================================================================
Table_4 Note:
To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 4. Examples of potential problems that can occur when identifying or isolating patients who may have infectious
tuberculosis (TB)
==============================================================================================================================================
Situation � Potential problem � Intervention
----------------+----------------------------------------------------------+----------------------------------------------------------------
Patient � Patient with signs or symptoms not identified. � Review triage procedures, facilities, and practices.
identification � �
during � Patient had no symptoms listed in triage protocol. � Reevaluate triage protocol.
triage � �
----------------+----------------------------------------------------------+----------------------------------------------------------------
During � Positive smear: results available >24 hours * after � Change laboratory practices. Assess potential barriers. Explore
review of � submitted. � alternatives.
laboratory � �
results � Positive smear: results available but action not taken � Educate appropriate personnel. Review protocol for
� promptly. � management of positive smear results.
� �
� Positive culture: results not available for >3 weeks. * � Change laboratory practices. Assess potential barriers. Explore
� � alternatives.
� �
� Positive culture: results available but action not taken � Educate appropriate personnel. Review protocol for
� promptly. � management of positive culture results.
� �
� Positive culture: susceptibility results not available � Change laboratory practices. Assess potential barriers. Explore
� for >6 weeks. * � alternatives.
� �
� Positive culture: susceptibility results available but � Educate appropriate personnel. Review protocol for
� action not taken promptly. � management of positive culture susceptibility results.
----------------+----------------------------------------------------------+----------------------------------------------------------------
At time of � Patient with signs/symptoms of TB: appropriate tests � Educate appropriate personnel. Evaluate protocols for TB
diagnosis � not ordered promptly. � detection.
and during � �
isolation � Isolation room unavailable. � Reassess need for number of isolation rooms.
� �
� Isolation not ordered or discontinued too soon, or � Educate patients and appropriate personnel. Evaluate
� isolation policy not followed properly (e.g., patients � institutional barriers to implementation of isolation policy.
� going outside of room). �
� �
� Personnel not properly using respiratory protection. � Educate appropriate personnel. Evaluate regularly scheduled
� � re-education. Evaluate institutional barriers to use of
� � respiratory protection.
� �
� Isolation room or procedure room not at negative � Make appropriate engineering modifications. Establish
� pressure relative to surrounding areas. � protocols for regularly monitoring and maintaining negative
� � pressure.
� �
� Inadequate air circulation. � Make appropriate engineering modifications.
� �
� Door left open. � Educate appropriate personnel and patients. Evaluate
� � self-closing doors, comfort levels in the room, and other
� � measures to promote door closing.
----------------+----------------------------------------------------------+----------------------------------------------------------------
* These time intervals are used as examples and should not be considered absolute standards.
==============================================================================================================================================
Table_S21 Note:
To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE S2-1. Summary of interpretation of purified protein derivative (PPD)-tuberculin
skin-test results
===============================================================================================
---------------------------------------------------------------------------------------------
1. An induration of >= 5 mm is classified as positive in:
- persons who have human immunodeficiency virus (HIV) infection or risk factors
for HIV infection but unknown HIV status;
- persons who have had recent close contact * with persons who have active tuber-
culosis (TB);
- persons who have fibrotic chest radiographs (consistent with healed TB).
2. An induration of >= 10 mm is classified as positive in all persons who do not meet any of
the criteria above but who have other risk factors for TB, including:
High-risk groups --
- injecting-drug users known to be HIV seronegative;
- persons who have other medical conditions that reportedly increase the risk for
progressing from latent TB infection to active TB (e.g., silicosis; gastrectomy or
jejuno-ileal bypass; being >= 10% below ideal body weight; chronic renal failure
with renal dialysis; diabetes mellitus; high-dose corticosteroid or other immuno-
suppressive therapy; some hematologic disorders, including malignancies such
as leukemias and lymphomas; and other malignancies);
- children <4 years of age.
High-prevalence groups --
- persons born in countries in Asia, Africa, the Caribbean, and Latin America that
have high prevalence of TB;
- persons from medically underserved, low-income populations;
- residents of long-term-care facilities (e.g., correctional institutions and nursing
homes);
- persons from high-risk populations in their communities, as determined by local
public health authorities.
3. An induration of >= 15 mm is classified as positive in persons who do not meet any of the
above criteria.
4. Recent converters are defined on the basis of both size of induration and age of the
person being tested:
- >= 10 mm increase within a 2-year period is classified as a recent conversion for
persons <35 years of age;
- >= 15 mm increase within a 2-year period is classified as a recent conversion for
persons >= 35 years of age.
5. PPD skin-test results in health-care workers (HCWs)
- In general, the recommendations in sections 1, 2, and 3 of this table should be fol-
lowed when interpreting skin-test results in HCWs.
However, the prevalence of TB in the facility should be considered when choosing
the appropriate cut-point for defining a positive PPD reaction. In facilities where
there is essentially no risk for exposure to Mycobacterium tuberculosis (i.e.,
minimal- or very low-risk facilities �Section II.B�), an induration >= 15 mm may be a
suitable cut-point for HCWs who have no other risk factors. In facilities where TB
patients receive care, the cut-point for HCWs with no other risk factors may be
>= 10 mm.
- A recent conversion in an HCW should be defined generally as a >= 10 mm increase
in size of induration within a 2-year period. For HCWs who work in facilities
where exposure to TB is very unlikely (e.g., minimal-risk facilities), an increase of
>= 15 mm within a 2-year period may be more appropriate for defining a recent con-
version because of the lower positive-predictive value of the test in such groups.
---------------------------------------------------------------------------------------------
* Recent close contact implies either household or social contact or unprotected occupational
exposure similar in intensity and duration to household contact.
===============================================================================================
Table_S22 Note:
To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE S2-2. Regimen options for the treatment of tuberculosis (TB) in children and adults
============================================================================================================================================================
-------+-------------------+-------------+-----------------------------+-----------+---------------+----------------------------------------------
� � � Initial treatment phase � Continuation treatment �
� � � � phase �
� � Total +-----------+-----------------+-----------+---------------+
Option � Indication � duration of � � � � Interval � Comments
� � therapy � � Interval and � � and �
� � � Drugs * � duration � Drugs * � duration �
-------+-------------------+-------------+-----------+-----------------+-----------+---------------+----------------------------------------------
1 � Pulmonary and � 6 mos � INH � Daily for 8 wks � INH � Daily or two � - EMB or SM should be continued until
� extrapulmonary � � RIF � � RIF � or three � susceptibility to INH and RIF
� TB in adults and � � PZA � � � times wkly + � is demonstrated.
� children � � EMB or SM � � � for 16 wks � - In areas where primary INH resistance is
� � � � � � � <4%, EMB or SM may not be necessary
� � � � � � � for patients with no individual risk
� � � � � � � factors for drug resistance.
-------+-------------------+-------------+-----------+-------+---------+-----------+---------------+----------------------------------------------
2 � Pulmonary and � 6 mos � INH � Daily � Two � INH � Two times � - Regimen should be directly observed.
� extrapulmonary � � RIF � for 2 times � RIF � wkly + for 16 � - After the initial phase, EMB or SM should
� TB in adults and � � PZA � wks, � wkly + � � wks & � be continued until susceptibility to INH
� children � � EMB or SM � then for 6 � � � and RIF is demonstrated, unless drug
� � � � � wks � � � resistance is unlikely.
-------+-------------------+-------------+-----------+-------+---------+-----------+---------------+----------------------------------------------
3 � Pulmonary and � 6 mos � INH � 3 times wkly + for 6 mos & � - Regimen should be directly observed.
� extrapulmonary � � RIF � � - Continue all four drugs for 6 mos. @
� TB in adults and � � PZA � � - This regimen has been shown to be
� children � � EMB or SM � � effective for INH-resistant TB.
-------+-------------------+-------------+-----------+-----------------+-----------+---------------+----------------------------------------------
4 � Smear- and � 4 mos � INH � Follow option � INH � Daily or two � - Continue all four drugs for 4 mos.
� culture-negative � � RIF � 1, 2, or 3 for � RIF � or three � - If drug resistance is unlikely (primary INH
� pulmonary TB in � � PZA � 8 wks � PZA � times wkly + � resistance <4% and patient has no
� adults � � EMB or SM � � EMB or SM � for 8 wks � individual risk factors for drug
� � � � � � � resistance), EMB or SM may not be
� � � � � � � necessary and PZA may be discontinued
� � � � � � � after 2 mos.
-------+-------------------+-------------+-----------+-----------------+-----------+---------------+----------------------------------------------
5 � Pulmonary and � 9 mos � INH � Daily for 8 wks � INH � Daily or two � - EMB or SM should be continued until
� extrapulmonary � � RIF � � RIF � times wkly + � susceptibility to INH and RIF is
� TB in adults and � � EMB or � � � for 24 wks & � demonstrated.
� children when � � SM ** � � � � - In areas where primary INH resistance is
� PZA is � � � � � � <4%, EMB or SM may not be necessary
� contraindicated � � � � � � for patients with no individual risk
� � � � � � � factors for drug resistance.
-------+-------------------+-------------+-----------+-----------------+-----------+---------------+----------------------------------------------
* EMB=ethambutol; INH=isoniazid; PZA=pyrazinamide; RIF=rifampin; SM=streptomycin.
+ All regimens administered intermittently should be directly observed.
& For infants and children with miliary TB, bone and joint TB, or TB meningitis, treatment should last at least 12 months. For adults with these forms of
extrapulmonary TB, response to therapy should be monitored closely. If response is slow or suboptimal, treatment may be prolonged on a case-by-case
basis.
@ Some evidence suggests that SM may be discontinued after 4 months if the isolate is susceptible to all drugs.
** Avoid treating pregnant women with SM because of the risk for ototoxicity to the fetus.
Note: For all patients, if drug-susceptibility results show resistance to any of the first-line drugs, or if the patient remains symptomatic or smear- or
culture-positive after 3 months, consult a TB medical expert.
============================================================================================================================================================
Table_S31 Note:
To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE S3-1. Air changes per hour (ACH) and time in minutes required for removal
efficiencies of 90%, 99%, and 99.9% of airborne contaminants *
======================================================================================================
Minutes required for a removal efficiency of:
---------------------------------------------
ACH 90% 99% 99.9%
----------------------------------------------------------------
1 138 276 414
2 69 138 207
3 46 92 138
4 35 69 104
5 28 55 83
6 23 46 69
7 20 39 59
8 17 35 52
9 15 31 46
10 14 28 41
11 13 25 38
12 12 23 35
13 11 21 32
14 10 20 30
15 9 18 28
16 9 17 26
17 8 16 24
18 8 15 23
19 7 15 22
20 7 14 21
25 6 11 17
30 5 9 14
35 4 8 12
40 3 7 10
45 3 6 9
50 3 6 8
----------------------------------------------------------------
* This table has been adapted from the formula for the rate of purging airborne contaminants
(99). Values have been derived from the formula t(1) = �In (C(2) / C(1)) / (Q / V)� X 60,
with T(1) = 0 and C(2) / C(1) - (removal efficiency / 100), and where:
t(1) = initial timepoint
C(1) = initial concentration of contaminant
C(2) = final concentration of contaminants
Q = air flow rate (cubic feet per hour)
V = room volume (cubic feet)
Q / V = ACH
The times given assume perfect mixing of the air within the space (i.e., mixing factor = 1).
However, perfect mixing usually does not occur, and the mixing factor could be as high as 10
if air distribution is very poor (98). The required time is derived by multiplying the appropriate
time from the table by the mixing factor that has been determined for the booth or room. The
factor and required time should be included in the operating instructions provided by the
manufacturer of the booth or enclosure, and these instructions should be followed.
======================================================================================================
Table_S32 Note:
To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE S3-2. Hierarchy of ventilation methods for tuberculosis (TB) isolation rooms
and treatment rooms
=====================================================================================================
Reducing concentration of � Achieving directional airflow
airborne tubercle bacilli * � using negative pressure +
-----------------------------------------+-----------------------------------------
1. Facility heating, ventilation, and � 1. Facility HVAC system.
air-conditioning (HVAC) system. � 2. Bleed air & from fixed room-air HEPA
2. Fixed room-air high-efficiency � recirculation system.
particulate air (HEPA) recirculation � 3. Bleed air from wall- or
system. � ceiling-mounted room-air HEPA
3. Wall- or ceiling-mounted room-air � recirculation system.
HEPA recirculation system. � 4. Bleed air from portable room-air
4. Portable room-air HEPA recirculation � HEPA recirculation unit. @
unit. � 5. Exhaust air from room through
� window-mounted fan. **
-----------------------------------------+-----------------------------------------
* Ventilation methods are used to reduce the concentration of airborne tubercle bacilli. If the
facility HVAC system cannot achieve the recommended ventilation rate, auxiliary room-air
recirculation methods may be used. These methods are listed in order from the most
desirable to the least desirable. Ultraviolet germicidal irradiation may be used as a
supplement to any of the ventilation methods for air cleaning.
+ Directional airflow using negative pressure can be achieved with the facility HVAC system
and/or the auxiliary air-recirculation--cleaning systems. These methods are listed in order
from the most desirable to the least desirable.
& To remove the amount of return air necessary to achieve negative pressure.
@ The effectiveness of portable room-air HEPA recirculation units can vary depending on the
room's configuration, the furniture and persons in the room, the placement of the unit, the
supply and exhaust grilles, and the achievable ventilation rates and air mixing. Units should
be designed and operated to ensure that persons in the room cannot interfere with or
otherwise compromise the function of the unit. Fixed recirculating systems are preferred
over portable units in TB isolation rooms of facilities in which services are provided regularly
to TB patients.
** This method simply achieves negative pressure and should be used only as a temporary
measure.
=====================================================================================================
Table_S33 Note:
To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE S3-3. Maximum permissible exposure times * for selected values of effective
irradiance
=====================================================================================================
Effective irradiance (Eeff) +
Permissible exposure time per day (uW/cm2)
-------------------------------------------------------------------
8 hrs 0.1
4 hrs 0.2
2 hrs 0.4
1 hr 0.8
30 min 1.7
15 min 3.3
10 min 5.0
5 min 10.0
1 min 50.0
30 sec 100.0
-------------------------------------------------------------------
* Permissible exposure times are designed to prevent acute effects of irradiation to skin and
eyes (136). These recommended limits are wavelength dependent because different wave-
lengths of ultraviolet (UV) radiation have different adverse effects on these organs.
+ Relative spectral effectiveness (S sub 1) is used to compare various UV sources with a source
producing UV radiation at 270 nm, the wavelength of maximum ocular sensitivity. For exam-
ple, the relative spectral effectiveness at 254 nm is 0.5; therefore, twice as much energy is
required at 254 nm to produce an identical biologic effect at 270 nm. At 254 nm, the NIOSH
REL is 0.006 joules per square centimeter (J/cm2); and at 270 nm, it is 0.003 J/cm2. For ger-
micidal lamps that emit radiant energy predominantly at a wavelength of 254 nm, proper use
of the REL requires that the measured irradiance level (E) in microwatts per square centimeter
(uW/cm2) be multiplied by the relative spectral effectiveness at 254 nm (0.5) to obtain Eeff. The
maximum permissible exposure time can be calculated (in seconds) by dividing 0.003 J/cm2
(the NIOSH REL at 270 nm) by Eeff in uW/cm2 (136,150). To protect health-care workers who
are exposed to germicidal UV radiation for 8 hours per work day, the measured irradiance (E)
should be <=0.2 uW/cm2, which is calculated by obtaining Eeff (0.1 uW/cm2), then dividing this
value by S sub 1 (0.5).
=====================================================================================================
Disclaimer
All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.

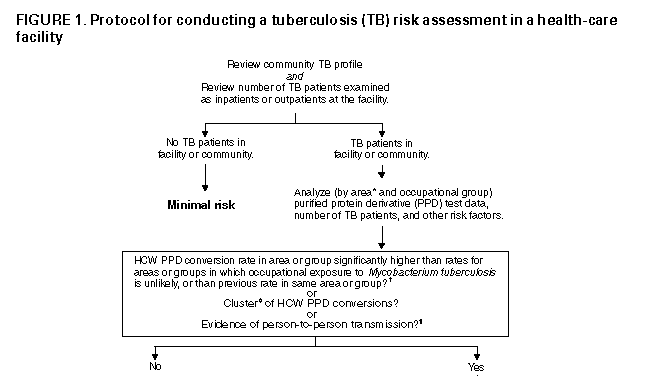
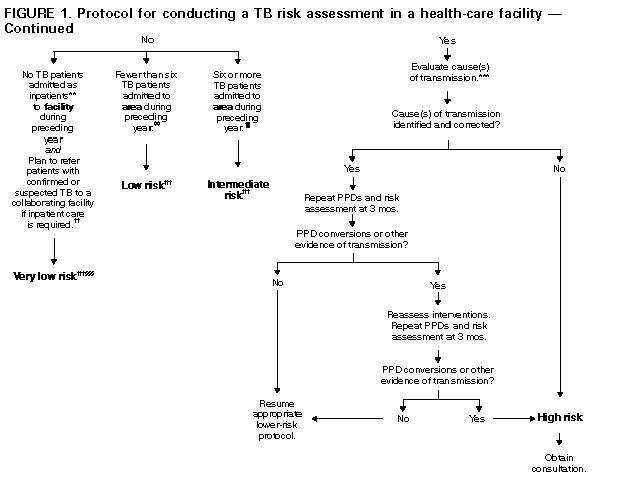
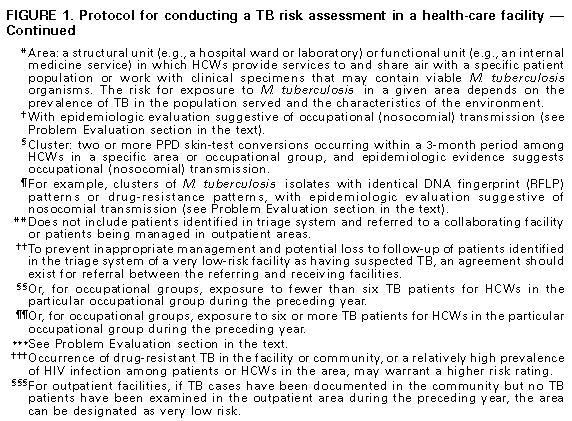
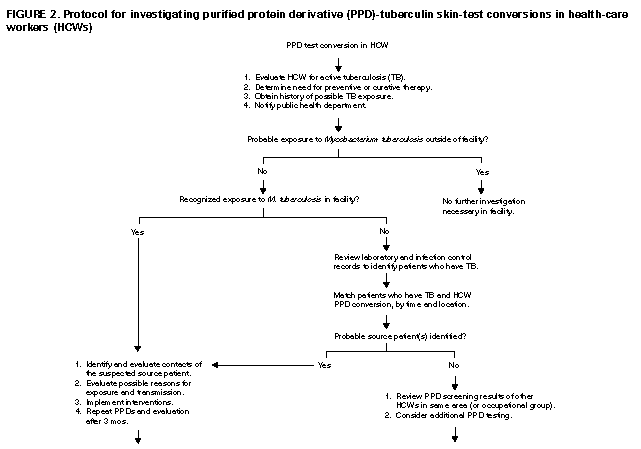
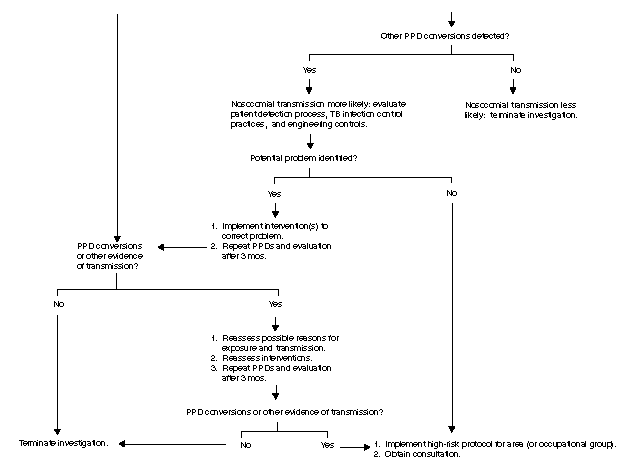
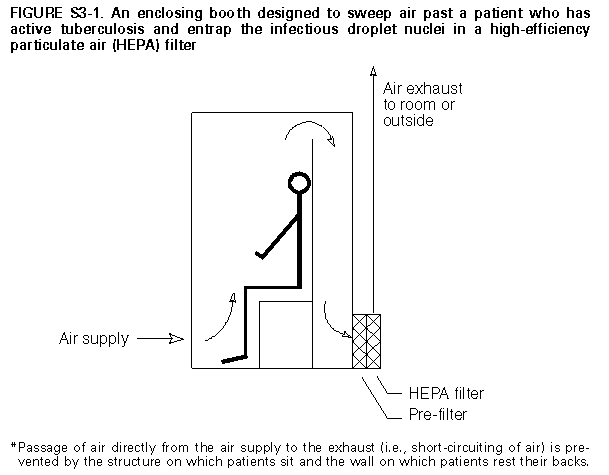
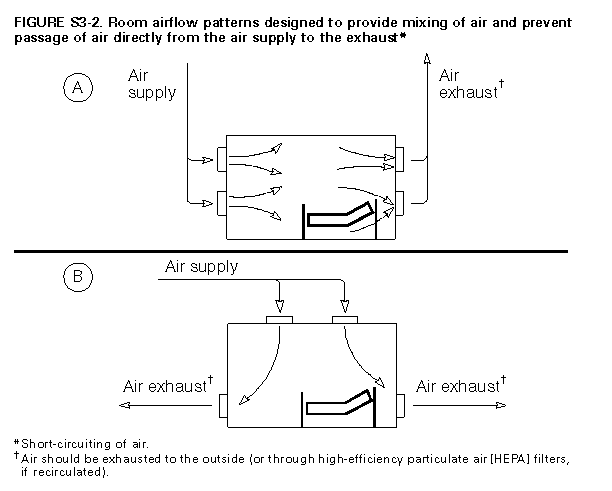
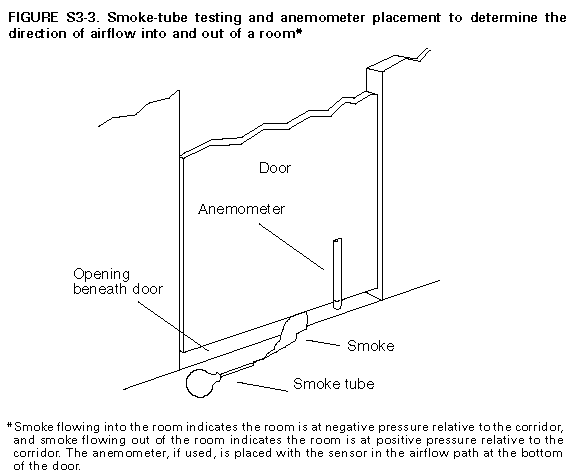
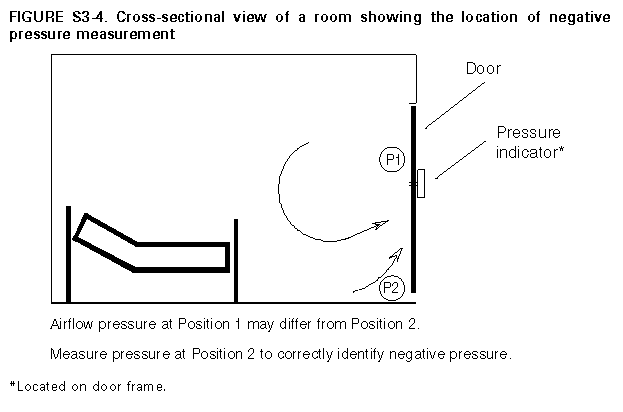
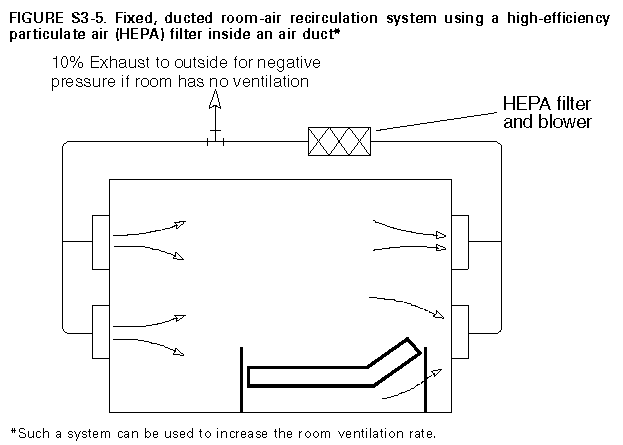
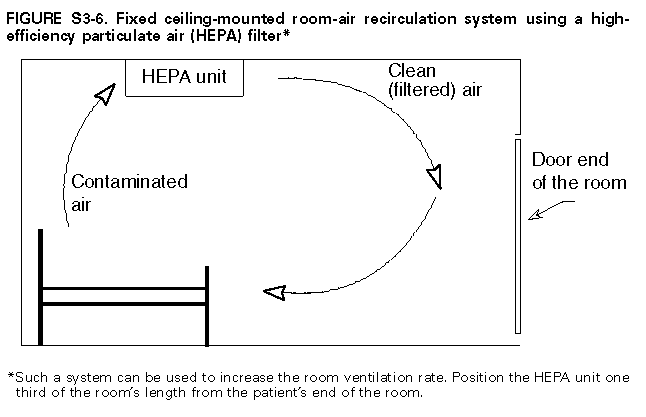
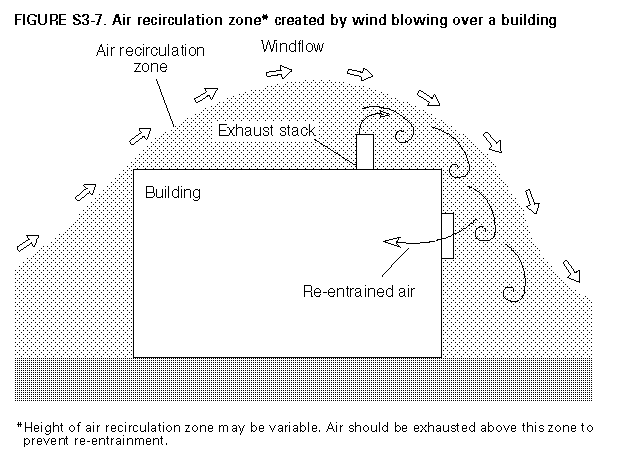
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}