Key points
- Trichophyton mentagrophytes genotype VII (TMVII) is an emerging dermatophyte associated with severe, inflammatory ringworm.
- TMVII primarily spreads through direct skin-to-skin contact with an infected lesion, including during intimate or sexual contact, and through contaminated items such as towels, bedding, clothing, razors, or sex toys.
- Reported cases have often involved inflammatory lesions of the genital, perianal, buttock, facial, or other areas.
- KOH preparation can confirm dermatophyte infection, but species confirmation requires advanced molecular testing.

Overview
Trichophyton mentagrophytes genotype VII, or TMVII (said as "T-M seven"), is an emerging dermatophyte fungus that can cause inflammatory ringworm, often affecting the groin and genital area. Transmission occurs through direct skin-to-skin contact with an infected lesion, including intimate or sexual contact. Transmission can also occur through contaminated items such as towels, bedding, clothing, razors, or objects shared during sexual activity (e.g., sex toys). Recent TMVII cases have often occurred among men who have sex with men; however, anyone can get TMVII.
Compared with more typical causes of ringworm, TMVII may present with more painful, pruritic, and inflammatory lesions and may require prolonged systemic therapy to achieve clearance and prevent recurrence. Current evidence suggests many TMVII infections respond to oral terbinafine, but clinicians should monitor response closely and consider alternatives such as itraconazole if improvement is inadequate.
Clinical features
Consider TMVII in patients with:
- Painful, pruritic, inflammatory, or persistent lesions
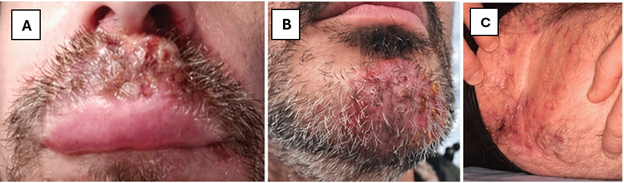
- Lesions involving the genitals, groin, buttocks, perianal area, face, beard, or other hair-bearing sites
- Sharply demarcated scaly plaques, pustules, or folliculitis-like eruptions
- Topical treatment failure
- Exposure history that includes sexual contact, close household contact, or travel
Clinical evaluation
Obtaining patient history
Obtain a focused history to assess exposures and factors that may affect diagnosis or treatment, including:
- Contact with a confirmed or suspected TMVII case, including sexual or household exposure
- Recent domestic or international travel
- Prior use of over-the-counter antifungals, corticosteroids, or antibacterials
- Sexual history, including anatomical sites of exposure
Physical examination
Perform a complete skin examination, including genital and intertriginous areas. Assess for:
- Pruritic, sharply demarcated, scaly plaques or pustules on the trunk, groin, genitals, face, extremities, or hands
- Inflamed, persistent, or painful lesions
- Erythematous papulonodules
- Folliculitis-like eruptions
Differential diagnosis and concurrent infections
The differential diagnosis includes:
- Syphilis
- Eczema
- Monkeypox
- Folliculitis
- Dermatitis
- Psoriasis
- Allergic skin reaction
- Drug eruptions
- HSV
- Dermatophyte infections caused by other species
Coinfections have been reported, including HIV, chlamydia, gonorrhea, syphilis, and monkeypox. Evaluate patients with genital, anal, or perianal lesions, or diffuse rash for STIs per the CDC STI Treatment Guidelines and monkeypox clinical guidance.
Diagnostic approach
Dermatophyte infection may be strongly suspected based on clinical presentation; however, TMVII can be clinically similar to other conditions in the differential diagnosis. When microscopy is available, perform KOH preparation using skin scrapings from affected areas. KOH preparation can confirm dermatophyte infection but does not identify the causative species.
Confirming TMVII requires advanced molecular methods, such as sequencing, available at select academic, commercial, and public health laboratories. If feasible, collect specimens before initiating antifungal treatment, as prior therapy may reduce diagnostic yield.
Clinical diagnosis based on history and physical examination may be sufficient to begin empiric treatment. Because TMVII can be misdiagnosed based on clinical appearance alone, diagnostic testing should still be attempted when feasible; however, treatment should not be delayed if suspicion is high. Confirmation of TMVII infection via diagnostic testing may take weeks. Note that topical antifungals used shortly before sample collection may reduce diagnostic yield.
Treatment
If TMVII is suspected, start oral terbinafine 250 mg daily as initial empiric therapy. If feasible, perform KOH preparation before starting antifungals, but do not delay treatment if microscopy is unavailable onsite. Therapy typically requires 6–12 weeks and may need to be extended until lesions have fully resolved.
Treatment considerations:
- Short courses under 2 weeks are ineffective.
- Some experts recommend continuing oral terbinafine for 2 weeks beyond symptom resolution to reduce the risk of relapse.
- Follicular involvement may contribute to relapse if treatment is stopped too early.
Although liver toxicity is extremely rare, consider baseline liver function testing before oral terbinafine in patients with underlying liver disease or heavy alcohol use.
Topical antifungals may be used as adjunctive therapy in selected patients, but oral therapy is generally preferred for suspected TMVII, especially for extensive, inflammatory, recurrent, or follicular disease. Avoid topical corticosteroids, including combination topical steroid–antifungal products, which can worsen symptoms.
Untreated infection can lead to chronic or spreading local disease, deep follicular inflammation, scarring, secondary bacterial infection, and continued transmission.
Patient follow-up
Reassess patients after approximately 4 weeks of oral terbinafine to evaluate clinical response and adherence. Continue periodic follow-up until clinical resolution.
If there is no meaningful clinical improvement after 4 weeks, reassess the diagnosis, adherence, and potential factors affecting treatment response (e.g., drug interactions, ongoing exposure). Consider obtaining confirmatory testing (if not already done) and consulting infectious disease or switching to an alternative oral antifungal such as itraconazole. If lesions worsen or fail to resolve after an adequate course of therapy (e.g., 6–12 weeks), reconsider the diagnosis and refer to dermatology or infectious disease for further evaluation.
If there is partial improvement, continue therapy and monitor, as prolonged treatment (e.g., 6–12 weeks or longer) may be required for complete resolution.
Refer to primary care, urgent care, or emergency department if patient develops signs and symptoms of a secondary bacterial infection such as:
- High fever
- Lesions that are spreading and not healing
- Very painful lesions
- Drainage from lesion
- Skin that is warm to the touch
Patient counseling
Counsel patients that TMVII can spread through direct skin-to-skin contact, including intimate or sexual contact, and may require prolonged therapy.
Advise patients to:
- Avoid touching or scratching lesions.
- Wash hands after contact with affected skin.
- Avoid sharing towels, bedding, clothing, sex toys, or other personal items that come into contact with affected skin.
- Launder shared items on high heat.
- Avoid sexual or intimate contact until lesions are fully healed and treatment is completed.
- Ensure lesions are fully covered if contact occurs before complete resolution.
Clinicians can also:
- Discuss evaluation of recent intimate or sexual partners who have rash or compatible symptoms.
- Advise that new or unexplained rash in the patient or their partners should prompt evaluation.
- Comfort patients by speaking to them with empathy and understanding. Reassure them that, if they have TMVII, it is treatable.
Additional counseling points:
- Prolonged therapy is often needed, and stopping treatment too early may contribute to persistence or relapse.
- Patients should return for follow-up if lesions do not improve or worsen.