Sewer Worker Dies When Inflatable Sewer Plug Bursts in Washington, D.C.
FACE 9017
SUMMARY
A sewer maintenance worker died while working inside a sewer gate chamber. An inflatable sewer plug downstream from the victim was overinflated and burst allowing sewage to flood the chamber. The worker was part of a 10-man sewer maintenance crew assigned to divert the flow of sewage in a branched, 6-foot diameter sewer main. The crew lowered an inflatable sewer plug into a diversion gate chamber and anchored it several feet into the right leg of the sewer main. An air line, connected to an air compressor at the surface, was attached to an air valve on the inflatable sewer plug. The victim, who was operating the compressor, left it running unattended and entered the gate chamber to inspect the sewer plug. Within a few minutes the plug burst, forcing water and air into the chamber, fatally injuring the worker. NIOSH investigators concluded that, in order to prevent future similar occurrences, employers should:
- use slide gates instead of, or in conjunction with, inflatable sewer plugs
- follow sewer plug manufacturers’ recommendations and other safety precautions on the installation and use of inflatable sewer plugs
- develop and implement specific confined space entry and work procedures.
INTRODUCTION
On November 29, 1989, a 45-year-old male municipal sewer maintenance worker died while working inside a 12-1/2-foot-deep sewer chamber when an inflatable sewer plug burst, allowing sewage to flood the chamber. On November 30, 1989, officials of the Water Pollution Control Federation (WPCF) notified the Division of Safety Research (DSR) of the death, and requested technical assistance. On December 14, 1989, a research industrial hygienist from DSR traveled to the incident site to conduct an investigation. The DSR investigator met with a representative for the municipality, and reviewed a report from the OSHA compliance officer assigned to this case. Photographs and diagrams of the incident site were obtained during the investigation.
The employer involved is a municipal utility with 1100 public works employees. Approximately 200 of the employees are sewer maintenance workers and wastewater treatment plant operators. The victim had been employed by the municipality for 23 years as a sewer maintenance worker. The public works department has a full-time safety and health manager and a full-time safety and health specialist. A safety policy exists but there are no confined space entry procedures for sewer maintenance workers. However, the victim and other sewer maintenance workers had participated in a 2-hour training session on confined space safety within the past year.
INVESTIGATION
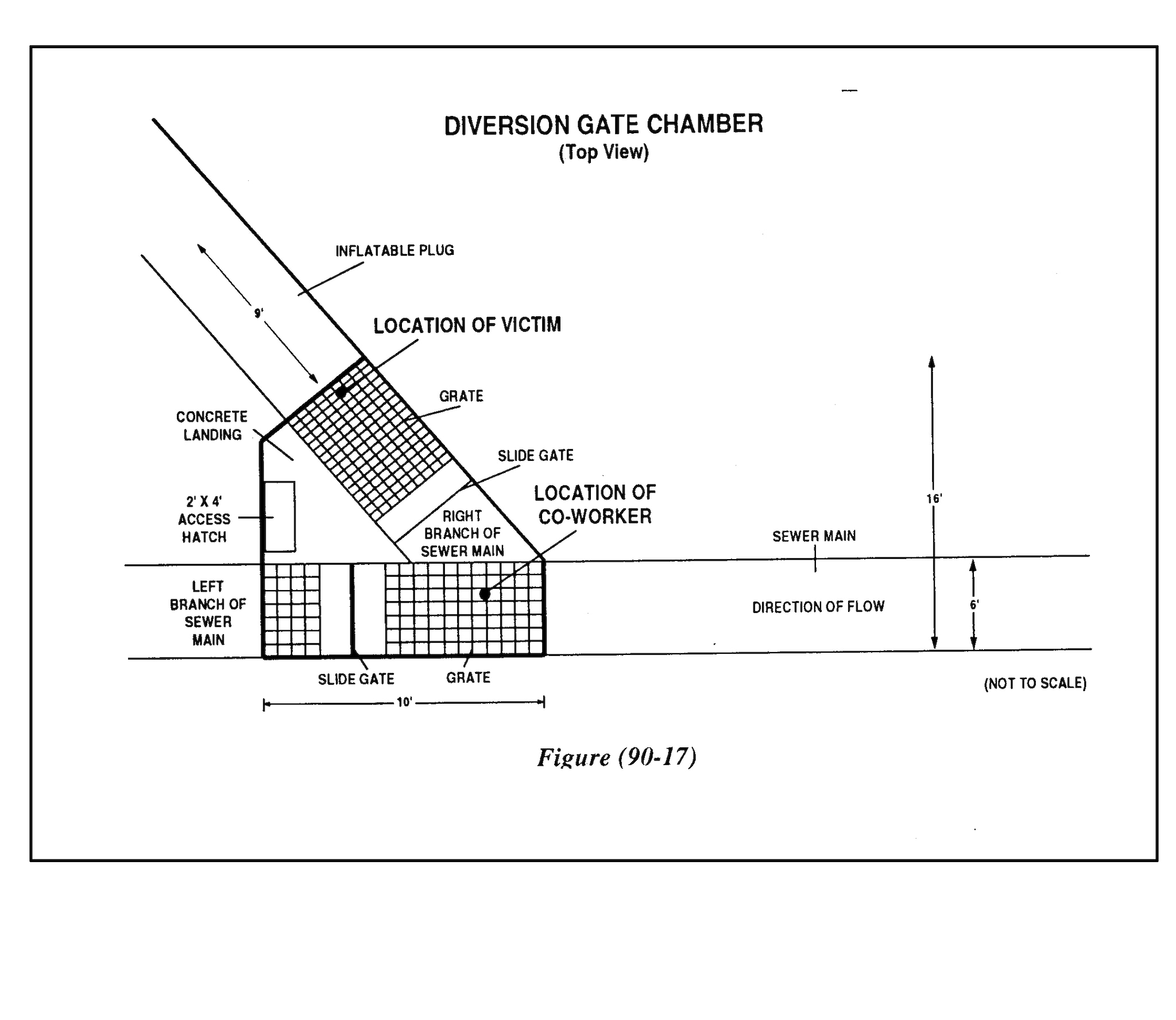
A crew of 10 sewer maintenance workers (including the victim) was assigned the task of diverting the flow of sewage in a 6- foot- diameter sewer main branch in preparation for installing some adjustable weirs (weirs are flow diversion devices). Access into the sewer main was provided by a diversion gate chamber located below a concrete drive area in an underground parking garage for a large building. The gate chamber was 12½ feet deep and approximately 10 feet wide by 16 feet long and located on top of a sewer main diversion branch which formed a “Y” configuration (Figure 1 ). The chamber had a 2-foot by 4-foot hatch with hinged steel covers and steel rungs built into the side of the chamber for access. The bottom of the chamber consisted of a removable aluminum grating over the sewer main and a concrete floor between the branches of the “Y”. The top of the grating in both branches was approximately 12 inches above the surface of the sewage, which normally flows at a height of 5 feet. The chamber housed a 3/8-inch-thick, 6-foot by 9½-foot aluminum slide gate in each branch of the sewer main (Figure 1). The purpose of the slide gates is to divert the flow of sewage for sewer maintenance purposes. Since the slide gates had not been operated for several years they had become stuck in the “open” position. Therefore, the crew used an inflatable sewer plug to block off the right branch of the sewer main, diverting all of the flow to the left branch of the sewer main (Figure 1).
The workers installed the sewer plug by lowering the deflated plug into the gate chamber, floating it several feet downstream into the right branch of the sewer main and anchoring it in place with a tethering line. An air line connected to an air compressor (rated at 90 PSI) on the surface was attached to an air valve on the sewer plug. The victim, who was initially above ground, began operating the compressor to inflate the plug and checking a pressure gauge on the air line at the compressor to ensure that the pressure in the sewer plug did not exceed 7 PSI (according to the sewer plug manufacturer’s recommendations). The foreman sent a sewer maintenance worker (co-worker) into the chamber to check on the plug. The foreman then walked about 30 feet away to examine a manhole. The victim left the compressor running unattended (for unknown reasons), entered the gate chamber, and began inspecting the installation of the sewer plug. By this time, the plug had expanded and closed off the right branch of the sewer main. The diverted sewage was flowing at its normal height of 5 feet into the left branch of the sewer main. The bottom edge of the slide gates were level with the surface of the sewage flow. The victim was standing on the grating between the plug and the right sewer branch slide gate, while the co-worker was standing on the grating in the left sewer branch on the opposite side of the right branch slide gate (Figure 1). A few minutes later (after the compressor had been running for approximately 20 minutes), the plug burst, forcing sewage and air into the chamber and out the access hatch. The force of the explosion broke and lifted the grating the victim was standing on, bulged out (approximately 6 inches) the 3/8-inch-thick aluminum slide gate in the right sewer branch, and broke a fluorescent light fixture on the ceiling of the parking garage 10 feet above the chamber access hatch. Evidence gathered after the incident suggests that the force of the explosion pushed the victim up against the concrete ceiling of the chamber. The victim then fell into the right branch of the sewer main and was washed downstream with the surge of sewage. The co-worker was not injured and was able to climb up the chamber rungs where he was helped out by the foreman.
The rescue squad from the city emergency medical service (EMS) was notified and arrived at the site in 5 minutes. After a 40- minute search, EMS personnel discovered the body of the victim submerged under the sewage flow, against the bar screen of a sewage pumping station approximately 200 yards downstream from the gate chamber. EMS personnel noted that the victim was dead at the scene.
CAUSE OF DEATH
The coroner listed the causes of death as asphyxiation by aspiration of food bolus, and blunt force injuries.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Where worker entry into sewers is necessary, slide gates should be used instead of, or in conjunction with, inflatable sewer plugs.
Discussion: Slide gates provide a more positive method for diverting/controlling the flow of sewage for maintenance purposes, and should be utilized where possible. In this incident, because the slide gates had not been used for quite some time, they had become inoperative. Slide gates of this type should be properly maintained and operated regularly to ensure their proper function.
Recommendation #2: Employers should ensure that sewer workers follow all sewer plug manufacturer’s safety recommendations and other safety precautions relevant to the safe installation and use of inflatable sewer plugs.
Discussion: Although some of the plug manufacturer’s recommendations were followed, an important precaution for the use of this type of sewer plug was not followed. The following precaution is stated on the first page of the sewer plug installation instructions: “Under no circumstances should anyone be in the pipe or manhole when the stopper (plug) is being inflated or deflated.” The victim left the air compressor running unattended. He had been trained in the manufacturer’s recommendations which stipulate that this size plug was to be inflated to only 7 PSI. The air pressure inside the plug may have exceeded the recommended pressure of 7 PSI, thus causing the plug to rupture. (The burst test pressure for this plug is 21 PSI.) Another safety recommendation given by the plug manufacturer (also stated on the first page of the sewer plug instructions) was not followed: “When working under submerged conditions, as a safety precaution, the stopper should be filled with water to its appropriate pressure.” According to the manufacturer, filling the plug with water instead of air when the plug is submerged will greatly reduce the force of a rupture.
Recommendation #3: Employers of sewer maintenance workers should develop and implement a comprehensive confined space entry program as outlined in NIOSH publication 80-106, “Working in Confined Spaces,” and 87-113, “A Guide to Safety in Confined Spaces.”
Discussion: Confined space entry procedures should address each type of confined space that sewer maintenance workers are required to enter (i.e., diversion chambers, wet wells, lift stations, utility vaults, sewer manholes, sewer mains, etc.). At a minimum, the following items should be addressed:
1. Is entry necessary? Can the assigned task be completed from the outside? For example, a sewer monitoring camera could be lowered into a sewer diversion gate chamber which would allow workers to perform inspections from the outside.
2. Is a confined space safe entry permit issued by the employer before each confined space is entered.
3. Are confined spaces posted with warning signs and are confined space procedures posted where they will be noticed by employees?
4. If entry is to be made, has the air quality in the confined space been tested for safety based on the following criteria:
- Oxygen supply at least 19.5%
- Flammable range less than 10% of the lower explosive limit
- Absence of toxic air contaminants
5. Have employees and supervisors been trained in the selection and use of:
- respiratory protection
- lifelines
- emergency rescue equipment
- protective clothing
6. Have employees been trained for confined space entry?
7. Are confined space safe work practices discussed in safety meetings?
8. Have employees been trained in confined space rescue procedures?
9. Is ventilation equipment available and/or used?
10. Is the air quality tested when the ventilation system is operating?
The above items may not have had a direct bearing on preventing this fatality. However, the incident was a routine sewer maintenance procedure having the potential of several additional and more common types of confined space work hazards (i.e., oxygen-deficient atmosphere, toxic and flammable vapors, etc.). These hazards would be safely controlled by following established NIOSH recommendations on working in confined spaces.
REFERENCES
National Institute for Occupational Safety and Health, Criteria for a Recommended Standard … Working in Confined Spaces. DHHS (NIOSH) publication number 80-106, December 1979.
National Institute for Occupational Safety and Health, A Guide to Safety in Confined Spaces. DHHS (NIOSH) publication number 87-113, 1987.