Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Neonatal Herpes Simplex Virus Infection Following Jewish Ritual Circumcisions that Included Direct Orogenital Suction — New York City, 2000–2011
Weekly
June 8, 2012 / 61(22);405-409Herpes simplex virus (HSV) infection commonly causes "cold sores" (HSV type 1 [HSV-1]) and genital herpes (HSV-1 or HSV type 2 [HSV-2]); HSV infection in newborns can result in death or permanent disability. During November 2000–December 2011, a total of 11 newborn males had laboratory-confirmed HSV infection in the weeks following out-of-hospital Jewish ritual circumcision, investigators from the New York City Department of Health and Mental Hygiene (DOHMH) learned. Ten of the 11 newborns were hospitalized; two died. In six of the 11 cases, health-care providers confirmed parental reports that the ritual circumcision included an ultra-Orthodox Jewish practice known as metzitzah b'peh, in which the circumciser (mohel, plural: mohelim) places his mouth directly on the newly circumcised penis and sucks blood away from the circumcision wound (direct orogenital suction). In the remaining cases, other evidence suggested that genital infection was introduced by direct orogenital suction (probable direct orogenital suction). Based on cases reported to DOHMH during April 2006–December 2011, the risk for neonatal herpes caused by HSV-1 and untyped HSV following Jewish ritual circumcision with confirmed or probable direct orogenital suction in New York City was estimated at 1 in 4,098 or 3.4 times greater than the risk among male infants considered unlikely to have had direct orogenital suction. Oral contact with a newborn's open wound risks transmission of HSV and other pathogens. Circumcision is a surgical procedure that should be performed under sterile conditions. Health-care professionals advising parents and parents choosing Jewish ritual circumcision should inquire in advance whether direct orogenital suction will be performed, and orogenital suction should be avoided.
Investigations of Reports
In November 2004, DOHMH was notified of twin male infants who developed disseminated HSV-1 infection following ritual circumcision (Table 1, cases 3 and 4); one died. The twins were born by cesarean delivery with surgical rupture of membranes and discharged at 4 days of life with normal physical examinations. Their mother had no history of oral or genital herpes and no genital lesions at or after delivery. At 8 days of life, the twins were circumcised by mohel A, who performed direct orogenital suction. At 16 days of life, both twins were evaluated for fever and lesions on their abdomen, buttocks, and perineum, including the genitals. HSV-1 was isolated from skin lesions of both twins. Twin A, who had been circumcised first, died from disseminated HSV-1 infection.
Investigation of 14 hospital staff members who cared for the infants after birth found no clinical evidence of current HSV infection and no history of HSV infection in the preceding 2 years. Investigation of hospital records found infection control policies sufficient to prevent HSV transmission from staff to neonates and no evidence of nosocomial HSV transmission to any neonates during the previous 2 years. Histologic examination of the diamniotic-dichorionic placenta showed no evidence of HSV infection. Maternal herpes serology showed HSV-1 antibody 4 weeks after the infants' illness onset. Specimens collected from mohel A 97 days after the twins' circumcisions were positive for antibody to HSV-1 (blood) and negative by culture and polymerase chain reaction (mouth swabs).
During the investigation, DOHMH learned of a 2003 case of neonatal HSV-1 infection following Jewish ritual circumcision that included direct orogenital suction by mohel A (Table 1, case 2). This infant developed vesicles on the penis, perineum, buttocks, back, and foot, beginning 10 days after circumcision. On investigation, the mother was negative for HSV-1 antibody. Hospital staff members who cared for the infant had no clinical evidence of herpes infection, and no evidence was found of nosocomial HSV transmission to neonates 2 years before and after the infant's birth.
In 2005, DOHMH learned of three additional cases of neonatal herpes infection following Jewish ritual circumcision with confirmed or probable direct orogenital suction. One case was an untyped HSV infection from 2000 (Table 1, case 1) and two cases were HSV-1 infections from 2005 (Table 1, cases 5 and 6).
Surveillance
In April 2006, DOHMH established population-based surveillance for neonatal herpes by modifying the New York City Health Code to mandate that laboratories report any laboratory test result indicating the presence of HSV in specimens from infants aged ≤60 days and that health-care providers report any infant aged ≤60 days receiving a diagnosis of herpes infection, even if laboratory confirmation is lacking. During April 2006–December 2011, a total of 84 laboratory-confirmed cases of neonatal herpes were reported. Forty-five cases were in males (HSV-1: 22; HSV-2: 15; and untyped HSV: eight), and 39 cases were in females (HSV-1: 15; HSV-2: 18; and untyped HSV: six).
Cases of laboratory-confirmed HSV-1 or untyped HSV infection in male infants were investigated to determine date of illness onset and whether ritual circumcision had been performed and had included direct orogenital suction. For five (11%) of the 45 male cases (HSV-1: 4 and untyped HSV: 1) reported during April 2006–December 2011, confirmed or probable direct orogenital suction was ascertained. Among the five cases were two from 2011. One of those patients died (Table 1, case 11); the other patient (Table 1, case 10) was the brother of a 2008 case (Table 1, case 8). The brothers were both circumcised by the same mohel (mohel X), whom their parents declined to identify. All four HSV-1 cases (18% of the 22 cases of HSV-1 infections in male newborns during April 2006–December 2011) were in residents of a single zip code area that accounts for only 2.5% of all live male births to New York City residents. No other neonatal herpes cases were reported from that zip code area during April 2006–December 2011.
Estimate of Relative Risk
To estimate the relative risk for neonatal herpes following Jewish ritual circumcision with confirmed or probable direct orogenital suction, neonatal HSV cases reported from April 2006 through December 2011 were used to construct incidence rate numerators, and New York City vital statistics for live male births were used for incidence denominators. The incidence of laboratory-confirmed neonatal herpes (HSV-1 or untyped HSV) among males who had ritual circumcision with confirmed or probable direct orogenital suction was compared with the incidence of laboratory-confirmed HSV-1 or untyped HSV infection among males unlikely to have had direct orogenital suction.
To estimate the number of males potentially exposed to direct orogenital suction each year, first the number of males entering full-day or half-day kindergarten in Jewish day schools in New York City in 2010 was obtained (6,197) (1). Next, the proportion of those children attending schools that could be considered ultra-Orthodox (Hassidic, 2,665 [43%] and Yeshiva, 1,797 [29%]) was derived from New York City data included in a national census of Jewish day schools (2). Next, an assumption was made that 100% of males entering Hassidic schools (2,665), and 50% of those entering Yeshiva schools (899) would have had direct orogenital suction, yielding an estimated annual population at risk of 3,564. This estimate was multiplied by 5.75 (years) to estimate the number of male infants (20,493) likely exposed to direct orogenital suction during the April 2006–December 2011 surveillance period (Table 2).
The number of male infants unlikely to have been exposed to direct oral suction (352,411) was estimated using vital statistics data for the number of live male births (372,904) in New York City during the 5.75-year surveillance period, after subtracting the number of males estimated to have been exposed to direct oral suction (20,493).* The risk for neonatal HSV-1 or untyped HSV infection following Jewish ritual circumcision with confirmed or probable direct orogenital suction during April 2006–December 2011 in New York City was estimated to be 24.4 per 100,000, a risk 3.4 (95% confidence interval = 1.3–9.0) times greater than the risk for HSV-1 or untyped HSV infection among male infants unlikely to have had direct orogenital suction (Table 2).
Additional Findings and Public Health Actions
Of the 11 known cases of HSV (nine HSV-1 and two untyped HSV) following Jewish ritual circumcision with confirmed or probable orogenital suction during 2000–2011, the interval from circumcision to appearance of herpes lesions ranged from 5 to 20 days (median: 8 days) (Figure). Two sets of parents said they were unaware beforehand that direct orogenital suction would be performed. In five cases, the identity of the mohel could not be determined; beginning in 2005, parents interviewed by DOHMH for the purposes of case investigation refused to explicitly state whether direct orogenital suction had been performed. Because mohel X could have been mohel A, the number of mohelim involved in the 11 cases could not be determined with certainty but was at least three and not more than eight.
Efforts made by DOHMH to prevent neonatal herpes included meetings with ultra-Orthodox Jewish community leaders to urge mohel A to stop practicing direct orogenital suction during circumcision and issuing an alert to health-care providers and an open letter to the Jewish community warning that the practice poses a health risk. In addition, a legally binding directive was issued by the New York City Commissioner of Health directing mohel A to cease and desist from direct orogenital suction.
Reported by
Susan Blank, MD, Julie E. Myers, MD, Preeti Pathela, PhD, Kate Washburn, MPH, Jay K. Varma, MD, James L. Hadler, MD, Thomas A Farley, MD, New York City Dept of Health and Mental Hygiene, New York, New York. Julia A. Schillinger, MD, Div of Sexually Transmitted Disease Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, CDC. Corresponding contributor: Julia A. Schillinger, jschilli@health.nyc.gov, 347-396-4078.
Editorial Note
Previous reports have described neonatal HSV-1 infection following Jewish ritual circumcision that included direct orogenital suction (3,4), including two additional cases in New York City occurring 10 years apart (5) that are not included in this report. The findings of this investigation and the previously published reports are consistent with a cause-and-effect relationship between Jewish ritual circumcision with direct orogenital suction and neonatal HSV-1 infection. The previous reports and these 11 additional cases strongly suggest HSV-1 can be transmitted to a neonate when circumcision involves direct orogenital suction of the penile incision.
Most neonatal HSV infections (85%) are transmitted during delivery from a mother with genital herpes; 5% of infections are congenital, and 10% are acquired after birth, usually from adult care-givers. The majority of infections present in the first 2 weeks of life. In mothers with genital herpes lesions at term, risk for perinatal transmission can be reduced by cesarean delivery (6).
For the 11 cases described in this report, transmission from the mother or health-care workers was largely excluded, and the preponderance of evidence pointed to acquisition during orogenital suction. First, in the cluster of three cases associated with mohel A, the twins were born by cesarean delivery, and the mother of the other HSV-infected neonate was HSV seronegative. Second, neonatal HSV-1 infection in males is uncommon, with a median of three cases each year in New York City, making it improbable that a single mohel would be associated with more than one case of male HSV-1 neonatal herpes in 2 years by chance alone. Although mohel A had no evidence of shedding HSV when tested, oral HSV shedding is intermittent and difficult to detect without repeated sampling (7). Third, the timing of symptom onset in all cases was consistent with acquisition during circumcision. Fourth, the location of herpes lesions on the neonates' genitals and related dermatomes is unusual and suggests infection was introduced at the genitals. Finally, all nine typed cases were HSV-1, which usually is transmitted orally.
The findings in this report are subject to at least one limitation. Although this report is the first to quantify the risk associated with the practice of direct orogenital suction during Jewish ritual circumcision, the relative risk depends, in part, on assumptions used to estimate the number of male infants who undergo circumcision with direct orogenital suction, and those assumptions might not be valid. For example, because not all of the cases were in ultra-Orthodox Jewish families, estimates of the exposed population might be underestimated. However, if the exposed population was overestimated, the risk associated with the practice of direct orogenital suction might be greater than described in this report.
Rabbinical authorities in some ultra-Orthodox Jewish communities maintain that direct orogenital suction is an integral part of ritual circumcision; other ultra-Orthodox authorities permit removal of blood by other means (e.g., a glass tube). Oral suction of an open wound poses an inherent risk for transmission of HSV-1 and other pathogens to a newborn infant and is not safe. Circumcision is a surgical procedure that involves cutting intact skin; sterile technique should be used to minimize infection risk.
Preventing the practice of direct orogenital suction is difficult, because ritual circumcision is a religious practice that usually occurs outside of health-care facilities. Continued efforts are needed to work with mohelim to adopt safe practices and educate parents regarding the risks for direct orogenital suction. Before circumcision, mohelim should inform both parents whether they perform direct orogenital suction and explain the risk of herpes transmission, so that parents can choose not to have their newborn exposed. In 2004, the prevalence of HSV-1 infection was 73% in New York City adults aged ≥20 years (8). Given the high prevalence of HSV-1 infection in the general population and risk for asymptomatic shedding, mohelim should assume they are infected and at risk for transmitting HSV.
Physicians should counsel parents considering out-of-hospital Jewish ritual circumcision about the risks associated with direct orogenital suction and, when evaluating a recently circumcised male infant with herpes infection, inquire about direct orogenital suction. Because approximately 20% of neonatal herpes patients do not have skin lesions (9), physicians should consider herpes infection when evaluating a newborn infant with fever following Jewish ritual circumcision. Even where neonatal HSV reporting is not mandated, physicians should notify local health departments about cases potentially associated with direct orogenital suction to prevent further cases. Local health departments should then notify the mohel who performed the procedure, so that he can voluntarily cease putting infants at risk. To protect infants' health, public health departments might need to take legal measures to ensure mohelim associated with cases of neonatal herpes cease the practice of direct orogenital suction.
References
- New York State Education Department, Information and Reporting Services. Basic educational data system. Albany, NY: New York State Education Department; 2012. Available at http://www.p12.nysed.gov/irs/beds
 . Accessed June 4, 2012.
. Accessed June 4, 2012. - Schick M. A census of Jewish day schools in the United States, 2008–2009. New York, NY: The Avi Chai Foundation; 2009. Available at http://avichai.org/wp-content/uploads/2010/06/Census-of-JDS-in-the-US-2008-09-Final.pdf
 . Accessed June 4, 2012.
. Accessed June 4, 2012. - Gesundheit B, Grisaru-Soen G, Greenberg D, et al. Neonatal genital herpes simplex virus type 1 infection after Jewish ritual circumcision: modern medicine and religious tradition. Pediatrics 2004;114:259–63.
- Distel R, Hofer V, Bogger-Goren S, Shalit I, Garty BZ. Primary genital herpes simplex infection associated with Jewish ritual circumcision. Isr Med Assoc J 2003;5:893–4.
- Rubin L, Lanzkowsky P. Cutaneous neonatal herpes simplex infection associated with ritual circumcision. Pediatr Infect Dis 2000;19:266–8.
- Brown ZA, Wald A, Morrow RA, Selke S, Zeh J, Corey L. Effect of serologic status and cesarean delivery on transmission rates of herpes simplex virus from mother to infant. JAMA 2003;289:203–9.
- Miller C, Danaher R. Asymptomatic shedding of herpes simplex virus (HSV) in the oral cavity. Oral Surgery Oral Med Oral Pathol Oral Radiol Endod 2008;105:43–50.
- New York City Department of Health and Mental Hygiene. New York City Health and Nutrition Examination Survey. New York, NY: New York City Department of Health and Mental Hygiene; 2004. Available at http://www.nyc.gov/html/doh/html/hanes/hanes.shtml. Accessed June 4, 2012.
- Kimberlin DW. Neonatal herpes simplex infection. Clin Microbiol Rev 2004;17:1–13.
* 2010 live birth data were used for 2011 because 2011 data were not yet available.
What is already known on this topic?
Cases of neonatal herpes simplex type 1 (HSV-1) infection following Jewish ritual circumcision with direct orogenital suctioning of the circumcision site have been reported in the United States, Canada, and Israel.
What is added by this report?
This report describes the largest series of cases (11) of neonatal herpes associated with Jewish ritual circumcision with direct orogenital suction, and is the first to estimate relative risk. During April 2006–December 2011, infant males who underwent circumcision with confirmed or probable direct orogenital suction had an estimated risk 3.4 times greater than the risk for HSV-1 or untyped HSV infection among male infants unlikely to have had direct orogenital suction.
What are the implications for public health practice?
Circumcision is a surgical procedure that can transmit infection if not performed under sterile conditions. Oral contact with an open wound in a neonate risks transmission of HSV and other pathogens. Professionals advising parents and parents choosing Jewish ritual circumcision should be aware of this risk, and direct orogenital suction should be avoided.
|
TABLE 2. Number of reported cases of laboratory-confirmed neonatal herpes simplex virus type 1 (HSV-1) or untyped HSV infection among male infants aged ≤60 days, by exposure status — New York City, April 2006–December 2011 |
|||
|---|---|---|---|
|
Exposure |
No. of cases of male HSV-1 or untyped HSV infection |
Estimated male infant population at risk |
Rate per 100,000 |
|
Ritual circumcision with confirmed or probable direct orogenital suction |
5 |
20,493 |
24.4 |
|
Unlikely to have had direct orogenital suction |
25 |
352,411 |
7.1 |
|
Total |
30 |
372,904 |
8.0 |
|
Sources: New York City mandatory reporting of cases by laboratories. New York State Education Department, Information and Reporting Services. Basic educational data system. Albany, NY: New York State Education Department; 2012. Available at http://www.p12.nysed.gov/irs/beds Schick M. A census of Jewish day schools in the United States, 2008–2009. New York, NY: The Avi Chai Foundation; 2009. Available at http://avichai.org/wp-content/uploads/2010/06/Census-of-JDS-in-the-US-2008-09-Final.pdf |
|||
FIGURE. Number of days between Jewish ritual circumcision* and appearance of herpes lesions, among male infants with neonatal herpes following Jewish ritual circumcision with confirmed or probable orogenital suction — New York City, 2000–2011
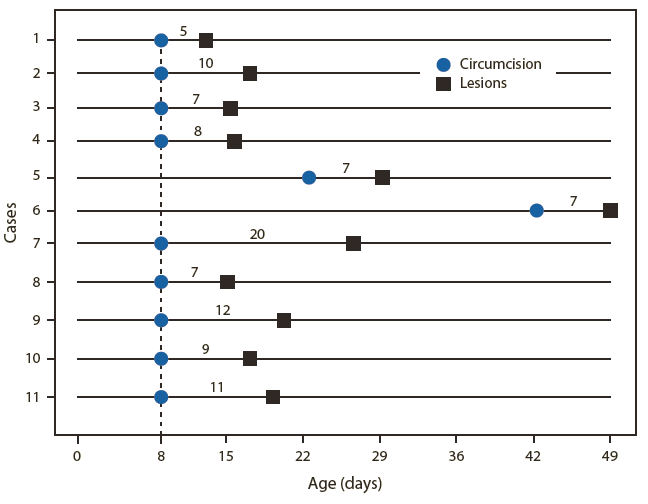
* For some cases, date of circumcision was reported only as "eighth day of life," which might differ from the age calculated by medical convention. Jewish law has various rules for scheduling circumcision; for example, circumcision might be delayed if an infant is ill.
Alternate text: The figure above consists of 11 timelines, showing the number of days between Jewish ritual circumcision and appearance of herpes lesions, among 11 male infants with neonatal herpes following Jewish ritual circumcision with confirmed or probable orogenital suction in New York City, during 2000-2011. The number of days from circumcision to lesions rangs from 5 to 20, with a median of 8 days.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
