FIGURE. Age-standardized prevalence of no leisure time physical activity among adults with arthritis — Behavioral Risk Factor Surveillance System, United States, 2009
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
State-Specific Prevalence of No Leisure-Time Physical Activity Among Adults With and Without Doctor-Diagnosed Arthritis — United States, 2009
The prevalence of no leisure-time physical activity (LTPA) among U.S. residents decreased from 31% in 1989 to 25% in 2002 and was still at 25% in 2008, based on Behavioral Risk Factor Surveillance System (BRFSS) data. Further reduction in the prevalence of no LTPA among all adults might be hindered by population subgroups that have exceptionally high rates of no LTPA, such as adults with arthritis. Approximately 50 million adults have arthritis, the majority of whom have arthritis-specific barriers to being physically active, such as pain and fear of making their arthritis worse (1,2). Despite the known benefits of physical activity for arthritis (e.g., reduced pain), persons with arthritis are more likely to report no LTPA (3–5). To assess state-specific prevalence of no LTPA among adults with and without doctor-diagnosed arthritis, CDC analyzed BRFSS data from 2009. This report summarizes the results of that analysis, which found that among adults with arthritis 1) prevalence of no LTPA is significantly higher compared with adults without arthritis in every state and the District of Columbia (DC), 2) the disparity in prevalence of no LTPA between adults with and without arthritis is large (median: 53% disparity gap), 3) 23 (45%) states had an age-standardized prevalence of no LTPA ≥30.0%, and 4) adults with arthritis reporting no LTPA comprised a substantial proportion (median: 35.2%) of all adults reporting no LTPA in each state. To reduce the prevalence of no LTPA among all adults, physical activity promotion initiatives should include interventions such as targeted health communication campaigns and community-based group exercise programs proven safe and effective for adults with arthritis.
BRFSS is an annual, random-digit–dialed landline telephone survey representative of the noninstitutionalized adult population aged ≥18 years that is conducted in all 50 states, DC, and the U.S. territories.* Data from 2009 (432,607 respondents) were used to assess prevalence of no LTPA (50 states and DC) by arthritis status and to produce age-standardized prevalence of no LTPA maps. For 2009, the median Council of American Survey and Research Organizations (CASRO)† response rate was 52.5% and the median CASRO cooperation rate was 75.0%. Respondents were defined as having arthritis if they reported a "yes" response to the question, "Have you ever been told by a doctor or other health professional that you have some form of arthritis, rheumatoid arthritis, gout, lupus, or fibromyalgia?" Respondents were classified as "no LTPA" if they answered "no" to the question, "During the past month, other than your regular job, did you participate in any physical activities or exercises such as running, calisthenics, golf, gardening, or walking for exercise?"
The unstandardized prevalence of no LTPA with 95% confidence intervals (CIs) was estimated for each state, by arthritis status, using sampling weights, which take into account the complex sample design, nonresponse, and noncoverage. State-specific and median relative percent differences (percent disparity gap) in unstandardized prevalence of no LTPA were calculated using the following formula: (prevalence of no LTPA with arthritis - prevalence of no LTPA without arthritis) / prevalence of no LTPA without arthritis × 100. The contribution (percent arthritis impact) of adults with arthritis reporting no LTPA on the overall prevalence of no LTPA in each state was calculated using the following formula: weighted number of adults with arthritis reporting no LTPA / weighted number of all adults reporting no LTPA × 100. Statistical significance was determined using t-tests. For mapping, age-standardized (based on the 2000 U.S. standard population), state-specific prevalence of no LTPA estimates among adults with arthritis were used to allow comparison of state data (Figure).
The unstandardized prevalence of no LTPA was significantly higher among adults with arthritis (median: 31.8% [CI = 30.2%–32.9%]; range: 21.1% in Minnesota to 42.6% in Tennessee) compared with adults without arthritis (median: 20.7% [CI = 19.6%–21.8%]; range: 13.9% in Oregon to 28.8% in West Virginia) in all states and DC (Table). The age-standardized prevalence of no LTPA was similar to unstandardized estimates (age-standardized prevalence, adults with arthritis range: 16.5% to 42.0%; adults without arthritis range: 14.3% to 29.3%).
The unstandardized prevalence of no LTPA for all states was approximately 53% higher (median percent disparity gap: 52.9% [CI = 47.6%–59.6%]; range: 27.9% in New York to 83.5% in Oregon) among adults with arthritis than adults without arthritis. Adults with arthritis reporting no LTPA comprised a substantial proportion of all adults reporting no LTPA in each state (percent arthritis impact: 35.2% [CI = 34.5%–36.4%]; range: 25.4% in California to 46.8% in Kentucky).
In 2009, the age-standardized prevalence of no LTPA among adults with arthritis was ≥30% in 23 states (including ≥40% in one state) (Figure). No state had an age-standardized prevalence of no LTPA ≥30% among adults without arthritis.
Reported by
Jennifer M. Hootman, PhD, Arthritis Program, Div of Adult and Community Health, Kathleen B. Watson, PhD, Carmen Harris, MPH, Div of Nutrition, Physical Activity, and Obesity, National Center for Chronic Disease Prevention and Health Promotion, Kamil E. Barbour, PhD, EIS Officer, CDC. Corresponding contributor: Jennifer M. Hootman, jhootman@cdc.gov, 770-488-6038.
Editorial Note
This report describes the relatively large (approximately 53% disparity gap) disparity in prevalence of no LTPA between adults with and without arthritis. Age-standardized prevalence of no LTPA among adults with arthritis was ≥30% in 23 states; in contrast, among adults without arthritis, the prevalence of no LTPA was <30% in all states. Furthermore, adults with arthritis comprise a substantial proportion (≥33%) of all adults reporting no LTPA in each state. These results are not surprising, given that adults with arthritis have disease-specific barriers to being physically active, such as joint pain, fear of injury, concern about making their arthritis worse, and lack of knowledge concerning safe types and appropriate amounts of physical activity (2). However, these barriers can be addressed through targeted health communication messages; increased access to arthritis-appropriate, individually adapted behavior change programs; and relevant policy and environmental changes (6).
CDC provides funds to 12 state health departments to support evidence-based health communication campaigns and physical activity programs in local communities. CDC's Arthritis Program has developed and evaluated two health communications campaigns, one targeting English-speaking adults with arthritis (Physical Activity. The Arthritis Pain Reliever), the other targeting Spanish-speaking adults with arthritis (Buenas Dias Artritis). Both have been shown to reach the intended audience, increase knowledge about physical activity, and increase initiation of physical activity (7). All campaign materials are updated regularly, customizable, and available free of charge§ Six structured physical activity programs¶ have been proven safe and effective (reduced pain, improved function, improved mood, etc.) for adults with arthritis, have standardized training and evaluation, are packaged to be delivered in local communities, and can be considered examples of behavioral approaches to increasing physical activity, as defined in The Guide to Community Preventive Services (6). These group exercise programs also provide social support facilitating physical activity among adults with arthritis (2).
CDC's Arthritis Program is working with the Arthritis Foundation and other national organizations to identify and promote policy strategies to help expand the reach of effective arthritis-appropriate physical activity programs. For example, one third of adults with arthritis state that their local fitness centers and other local community organizations do not offer arthritis "friendly" exercise classes (e.g., low impact) or have instructors that are knowledgeable about exercising with arthritis (2). Organizational-level policies can address these barriers and promote increased access to effective programs. For example, parks and recreation departments can institute a policy that they offer at least one arthritis-appropriate exercise program. To address the lack of knowledgeable instructors, the American Council on Exercise, working with the Arthritis Foundation and the Association of Rheumatology Health Professionals, developed an online knowledge-based continuing education program for fitness professionals (The Fitness Professional's Guide to Training Clients with Osteoarthritis).** In 2012, the CDC Arthritis Program will initiate work with the American College of Sports Medicine to develop an arthritis-specific, skills-based training and certification program for fitness professionals.
The findings in this report are subject to at least four limitations. First, all information in the BRFSS is self-reported and might be prone to recall or social desirability bias. However, among adults with arthritis, self-reported physical inactivity prevalence (44%) (5) is similar to accelerometer-measured physical inactivity prevalence (48%) (4). Self-reported physical activity also has been associated with lower rates of mortality, chronic disease, obesity, and arthritis symptoms (3,8), and these estimates are the most realistic to use for population level surveillance. Second, occupational, household, and transportation-related physical activities can contribute to health, but are not captured with the single LTPA question used for population surveillance (9). However, LTPA might be the most feasible physical activity area for most persons to modify. Despite these limitations, this study is consistent with others (4,5) showing that adults with arthritis have high rates (40%–50%) of physical inactivity. Third, no LTPA might result from factors other than arthritis, although arthritis symptoms (e.g., pain or fatigue) are the primary barrier to being physically active reported by adults with arthritis (2). Finally, BRFSS does not capture institutionalized persons or households without a landline telephone. However, data from the National Health Interview Survey showed that when landline data were weighted to match demographic characteristics of the full population, noncoverage bias generally was less than 2 percentage points (10).
This report used data from a large sample, which allows for reliable and precise calculation of state-level estimates. The impact measure is a function of each state's prevalence of arthritis†† and prevalence of no LTPA. For example, DC has the second lowest prevalence of arthritis (20.8%) but a relatively high percent arthritis impact on no LTPA (31.1%). In contrast, Kentucky has the highest arthritis prevalence (35.6%) and a similarly high impact (46.8%). This is useful information for public health practice, priority setting, partnerships, and physical activity program planning at the state level because states might have similar impact but widely different arthritis prevalence.
Implementing effective communitywide campaigns with arthritis-specific messages, increasing access to arthritis-appropriate physical activity programs, and fostering policy and environmental initiatives likely to benefit adults with arthritis are essential to reducing the overall rate of no LTPA among all U.S. adults. The findings in this report suggest that, to reduce the prevalence of no LTPA among all adults, adults with arthritis are a high-need group that should be targeted with arthritis-specific physical activity promotion initiatives. Health-care providers and public health physical activity practitioners should counsel arthritis patients regarding the benefits of physical activity and refer them to physical or occupational therapy if indicated or to locally available arthritis-appropriate physical activity programs.
References
- CDC. Prevalence of doctor-diagnosed arthritis and arthritis-attributable activity limitation—United States, 2007–2009. MMWR 2010;59:1261–5.
- Brittain DR, Gyurcsik NC, McElroy M, Hillard SA. General and arthritis-specific barriers to moderate physical activity in women with arthritis. Womens Health Issues 2011;21:57–63.
- Kelley GA, Kelley KS, Hootman JM, Jones DL. Effects of community-deliverable exercise on pain and physical function in adults with arthritis and other rheumatic diseases: a meta-analysis. Arthritis Care Res 2011;63:79–93.
- Dunlop DD, Song J, Semanik PA, et al. Objective physical activity measurement in the osteoarthritis initiative: are guidelines being met? Arthritis Rheum 2011;63:3372–82.
- Shih M, Hootman JM, Kruger J, Helmick CG. Physical activity in men and women with arthritis: National Health Interview Survey, 2002. Am J Prev Med 2006;30:385–93.
- Community Preventive Services Task Force. Promoting physical activity. In: The guide to community preventive services. Atlanta, GA: US Department of Health and Human Services, CDC; 2011. Available at http://www.thecommunityguide.org/pa/index.html. Accessed December 2, 2011.
- Brady TJ. Moving from identifying to addressing health disparities: a public health perspective, Arth Care Res 2007;57:544–6.
- Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee report, 2008. Washington, DC: US Department of Health and Human Services; 2008. Available at http://www.health.gov/paguidelines/report/pdf/committeereport.pdf. Accessed December 2, 2011.
- Carlson SA, Densmore D, Fulton JE, Yore MM, Kohl HW. Differences in physical activity prevalence and trends from 3 U.S. surveillance systems: NHIS, NHANES, and BRFSS. J Phys Act Health 2009;6(Suppl 1):S18–27.
- Blumberg SJ, Luke JV. Reevaluating the need for concern regarding noncoverage bias in landline surveys. Am J Public Health 2009;99:1806–10.
* Additional information is available at http://www.cdc.gov/brfss/technical_infodata/surveydata.htm.
† CASRO response rates are defined as the percentage of completed interviews among all eligible persons. CASRO cooperation rates are defined as the percentage of completed interviews among all eligible persons who were actually contacted.
§ Additional information about the CDC Arthritis Program's health communications campaigns is available at http://www.cdc.gov/arthritis/interventions/campaigns.htm.
¶ Additional information about CDC's evidence-based, arthritis-appropriate physical activity programs is available at http://www.cdc.gov/arthritis/interventions/physical_activity.htm.
** Additional information is available at http://www.acefitness.org/continuingeducation/continuingeducationcoursedetail.aspx?courseid=4a5x87w7.
†† State arthritis statistics are available at http://www.cdc.gov/arthritis/data_statistics/state_data_list.htm.
What is already known on this topic?
Physical activity improves pain management, function, and mood, and reduces disability among adults with arthritis. Despite this, adults with arthritis have high rates of physical inactivity.
What is added by this report?
In every state, adults with arthritis have significantly higher prevalence of no leisure-time physical activity (LTPA) compared with adults without arthritis. In 23 states, the prevalence of no LTPA among adults with arthritis is particularly high (≥30%). Adults with arthritis comprise a large proportion (≥33%) of all adults reporting no LTPA in every state.
What are the implications for public health practice?
To further reduce the prevalence of no LTPA in the population, adults with arthritis should be targeted with disease-specific physical activity promotion initiatives.
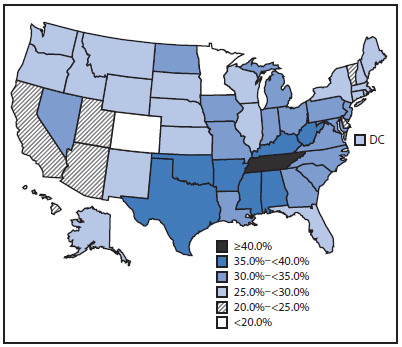
Alternate Text: The figure above shows age-standardized prevalence of no leisure time physical activity (LTPA) among U.S. adults with arthritis during 2009, based on data from the Behavioral Risk Factor Surveillance System. For mapping, age-standardized (based on the 2000 U.S. standard population), state-specific no LTPA prevalence estimates among adults with arthritis were used to allow comparison of state data. Prevalence ranged from less than 20% in Colorado and Minnesota to 40% or more in Tennessee.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
