 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Pedal-Cycle Injuries Among Children Aged <6 Years --- Wisconsin, 2002--2004Measures to improve pedal-cycle* safety and increase helmet use often target school-age children rather than younger children (1), even though preschool children wearing helmets have fewer injuries (2) and are more likely to wear helmets in the future (3), compared with children who do not wear helmets. Children aged <6 years also use pedal cycles; whether they are passengers on a parent's bicycle, riding a tricycle or pedal car, or learning to ride a bicycle, these young cyclists often sustain injuries (1). To provide guidance for intervention strategies targeted to young children in Wisconsin, CDC and the Wisconsin Division of Public Health analyzed data collected from January 1, 2002 through December 31, 2004, from all nonfederal emergency departments (EDs) and hospitals in Wisconsin regarding pedal-cycle injuries among children aged <6 years. This report describes the results of that analysis, which indicated that, during 2002--2004, a total of 2,046 ED visits by Wisconsin residents aged <6 years for pedal-cycle injuries occurred; for 1,305 (63.8%) of these visits, the primary diagnosis was a head or neck injury. These findings underscore the need for interventions designed to reduce head and neck injuries in the youngest users of pedal cycles. The Wisconsin Bureau of Health Information and Policy maintains data from ED visits and hospital discharges through a statewide mandatory reporting system for nonfederal hospitals. An injury event was defined as a 2002--2004 ED visit or hospitalization for a Wisconsin resident aged <6 years with an International Classification of Diseases, Ninth Revision, Clinical Modification code from 800 to 959 indicating injury as one of the diagnoses for the encounter and an E-code indicating an injury sustained by a rider or passenger on a pedal cycle† (4). In addition, the Wisconsin Vital Records Office collects mortality information for the state; pedal-cycle deaths were defined as reports with International Classification of Diseases and Related Health Problems, Tenth Revision codes V10--V19 as the underlying or contributing cause of death. U.S. Census Bureau population estimates from 2002 were used to calculate incidence rates (5). The Barell Injury Diagnosis Matrix was used to classify the primary diagnosis by body location and nature of the injury (6). Secondary diagnoses were excluded for the purpose of this analysis. For comparison, the number and proportion of ED visits for head and neck injuries for Wisconsin children aged 6--18 years were calculated using the same methodology. In addition, for two areas, Port Washington (population: 10,518) and Milwaukee County (population: 934,352), the number of pedal-cycle--related ED visits and the proportion of head and neck injuries in residents aged <6 years were examined separately to determine whether a mandatory helmet law in Port Washington and the urban environment of Milwaukee County influenced the number and types of pedal-cycle injuries (7,8). These areas were included in the state totals. During 2002--2004, a total of 546,950 ED visits associated with a child aged <6 years occurred; 116,395 of these visits listed an injury as the primary diagnosis. Of these injury visits, 2,046 (1.8%) were attributed to injuries resulting from a pedal-cycle crash, accounting for an annual incidence rate of 16.7 per 10,000 population aged <6 years. Of these pedal-cycle injury visits, 1,305 (63.8%) were for a primary diagnosis of head or neck injury, and 74 (3.6%) were for a primary diagnosis of traumatic brain injury. In comparison, 682,257 visits to an ED associated with Wisconsin residents aged 6--18 years occurred; 284,127 (41.6%) were for injuries. For this older population, 13,872 (4.9%) injury visits were for pedal-cycle injuries, and 4,290 (30.9%) of the pedal-cycle injury visits had a primary diagnosis of a head or neck injury. During 2002--2004, ED charges associated with the primary diagnosis of a pedal-cycle injury for patients aged <6 years totaled $1,093,258 ($654,636 for visits with the primary diagnosis of a head and neck injury). Of the pedal-cycle injury ED visits for patients aged <6 years, 1,424 (69.6%) visits were for boys, and 622 (30.4%) visits were for girls. Injuries occurred more frequently during April--September (Figure). The youngest patient was aged 11 months, and the number of visits increased with age (Table). Forty visits were attributed to a pedal-cycle crash with a motor vehicle in traffic; 23 of these had a head injury as the primary diagnosis. Forty-eight hospitalizations occurred (17 for head and neck injuries), with charges totaling $439,860 ($151,853 for head and neck injuries). Traffic-related motor-vehicle crashes led to a total of seven hospitalizations. During 2002--2004, no children aged <6 years died of pedal-cycle injuries. No differences were observed in injury rates between either Port Washington or Milwaukee County and the rest of the state. During 2002--2004, four pedal-cycle ED visits were associated with Port Washington residents aged <6 years (annual incidence rate: 15 per 10,000); two of those visits were for a head injury. Milwaukee County, the most urban county in Wisconsin, had the same rate of ED visits for pedal-cycle injuries and pedal-cycle head and neck injuries as the rest of the state. Reported by: R Glysch, MS, H Anderson, MD, Wisconsin Div of Public Health. W Daley, DVM, Office of Workforce and Career Development; A Wendel, MD, EIS Officer, CDC. Editorial Note:During 2002--2004, Wisconsin children aged <6 years accounted for 2,046 ED visits for pedal-cycle injuries, and the primary diagnosis for nearly two thirds of these injuries was head or neck injury. Previous studies also have indicated that head injuries are the predominant category of injury in young pedal cyclists (1,9). Further study is needed to develop effective prevention strategies for young children to determine whether interventions targeted to children aged <6 years will provide a foundation for future safe cycling behaviors. In Wisconsin, most pedal-cycle injury ED visits for children aged <6 years did not involve motor vehicles. These findings are consistent with a study using 1993--1997 data from the National Hospital Ambulatory Medical Care Survey (NHAMCS) (1). In addition, the NHAMCS study indicated that only 24% of bicycle-related injuries among children aged <4 years occurred in a street (1). The findings in this report are subject to at least six limitations. First, ED data likely are underestimates of the total number of injuries and might be overestimates of the proportion of head and neck injuries. Parents might not seek medical attention for minor injuries, or they might take the child to their regular doctor. Second, the ED database does not contain information on whether the child wore a helmet or where the incident occurred, preventing analysis of these two factors. Third, the number of children in each community who are pedal cyclists is unknown, limiting injury rate comparisons between communities. Fourth, the assessment of the effect of bicycle helmet legislation was restricted by the small population affected by these laws. Fifth, this analysis did not distinguish between head and neck injuries. Finally, only the primary diagnosis was included in the analysis; head and neck injuries that were not primary diagnoses were excluded, potentially underestimating the total number of head and neck injuries. Even young children are at risk for injuries from pedal-cycle injuries, which are predominantly head and neck injuries. Helmets might protect children from a subset of these injuries because helmets have been determined to prevent pedal-cycle--related head and facial injuries (2). Children aged <1 year should not be transported on a pedal cycle because they lack the neck strength to support a helmet (10). When fitted properly, the front part of the helmet should be low on the forehead so that if the child falls forward, the helmet strikes first, protecting the head and much of the upper face from impact. Although measures to improve bicycle safety often focus on teaching helmet use and safe bicycling techniques to children aged >5 years (1), the findings in this report demonstrate that potentially preventable injuries occur among children at younger ages. Acknowledgments This report is based, in part, on data contributed by the Wisconsin Bureau of Health Information and Policy. References
* Any wheeled, pedal-powered vehicle, including tricycles, bicycles, pedal cars, and trailers or sidecars attached to these vehicles. † E800.3, E801.3, E802.3, E803.3, E804.3, E805.3, E806.3, E807.3, E810.6, E811.6, E812.6, E813.6, E814.6, E815.6, E816.6, E817.6, E818.6, E819.6, E820.6, E821.6, E822.6, E823.6, E824.6, E825.6, E826.1, E827.1, E828.1, and E829.1.
Table 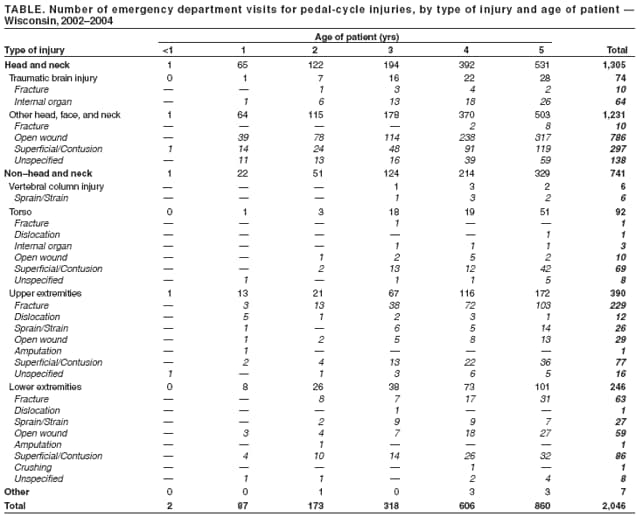 Return to top. Figure 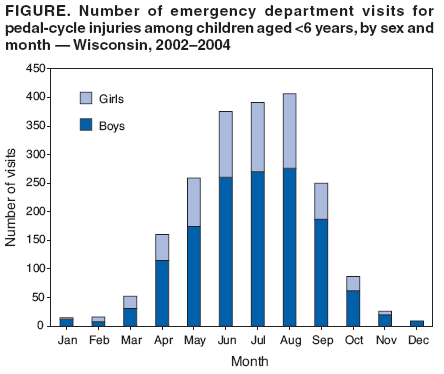 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 12/20/2006 |
|||||||||
|