 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Improvement in Local Public Health Preparedness and Response Capacity --- Kansas, 2002--2003After the terrorist attacks of September 11, 2001, increased funding was provided to federal, state, and local health departments to improve their capacities for terrorism preparedness and emergency response. To evaluate the effect of this funding and to identify priority program areas in Kansas, the Kansas Association of Local Health Departments (KALHD) contracted with the Kansas Health Institute (KHI) to perform an independent assessment of local health department (LHD) preparedness capacity using a CDC assessment tool. This report summarizes the results of two surveys of LHDs and changes in preparedness capacity from 2002 to 2003. The findings indicated a substantial increase in local preparedness capacity, although increases among counties varied widely. Repeated assessments of preparedness using standardized tools can provide useful information to help guide federal, state, and local public health policies and investments. In 2002, CDC developed the Public Health Preparedness and Response Capacity Inventory (1) to provide rapid assessment of a local public health agency's capacity to respond to public health threats and emergencies. The assessment tool is organized into six sections, which correspond to six focus areas (FAs) (i.e., planning and assessment [FA A], surveillance and epidemiology [FA B], laboratory capacity [FA C], communication and information technology [FA E], risk communication and health information dissemination [FA F], and education and training [FA G]), as defined in the CDC cooperative agreement that funds many state terrorism preparedness activities. The six FAs include a total of 15 critical capacities targeted for achievement. The assessment tool was field-tested, revised, and made available for national distribution in August 2002. Its validity has been described elsewhere (2). The assessment tool includes 79 questions and approximately 700 subquestions. Thirty additional questions were added to target Kansas-specific preparedness capacities not fully addressed by the assessment tool (e.g., adoption of Kansas-specific disease intervention protocols or computer security standard procedures). The printed questionnaire was converted to electronic form to support data submission from LHDs via a secure, Internet-based, communication system. Answers were submitted electronically during the second half of 2002 and the second half of 2003, leaving approximately 1 year between the two assessments. LHDs representing 103 of 105 (98%) Kansas counties (i.e., one LHD per county) responded to both surveys. Most questions in the assessment tool have a limited number of multiple-choice answers and are qualitative in nature; for example, respondents were asked to specify the extent to which a certain activity had been completed. To calculate measures of LHD capacity, the KHI project team, in consultation with representatives from LHDs, developed a method for aggregating responses from multiple questions into summary scores. Each question was assigned to one or more of the 15 critical capacities. Representatives from KALHD and KHI developed a method for converting responses to each survey question to dichotomous, "achieved" or "not achieved" classifications. These criteria were included in a computerized algorithm used to analyze all the answers from all LHDs. Through the computerized analysis, a preparedness index was calculated for each LHD for every critical capacity. FA preparedness indexes were computed by calculating the unweighted average of the critical capacities indexes included in that FA. Finally, an overall, county-level preparedness capacity index was computed as the average of the indexes for all the FAs for each LHD. To summarize local preparedness capacity in Kansas, state averages of the critical capacities and FAs indexes were computed as the unweighted averages of the corresponding county-level indexes. State overall preparedness indexes were calculated as the average of all county overall preparedness indexes. From 2002 to 2003, a total of 89 (86.4%) of the 103 participating counties improved their county preparedness capacity indexes (median change = 27%). The state average for the overall local preparedness capacity index increased by 27.7%, from 33.9% to 43.3%. Improvement was observed for each FA index, with the largest increase (48.3%) in FA G (education and training) and the smallest (10.4%) in FA C (laboratory capacity) (Table). Substantial differences were observed in county preparedness capacity indexes; in 2003, indexes ranged from 17.3% to 75.5% (median = 42%). Rural areas lagged in preparedness improvement. In 2003, the 33 counties in the lowest population density group achieved an average preparedness index capacity of 38%, in contrast with the average index of 56% achieved by the six urban counties in the highest population density group. From 2002 to 2003, this gap appeared to widen; the ratio of the mean preparedness index for urban and rural counties increased from 1.3 to 1.5. Reported by: G Pezzino, MD, B Starrett, MHA, B LaClair, MHA, M Velasco, Kansas Health Institute; E Snethen, Kansas Assoc of Local Health Depts; JM Connor, MBA, Unified Government Public Health Dept, Wyandotte County; S Cline, Ottawa County Health Dept; K Kent, Douglas County Health Dept; M Reece, Kansas Dept of Health and Environment. Editorial Note:Approximately $2 billion was distributed to state and local governments during 2002--2003 to improve public health capacity for terrorism preparedness and emergency response. The findings in this report suggest that this investment has resulted in measurable improvement of preparedness capacity in the majority of counties in Kansas. These achievements, however, should be balanced with the finding that state overall preparedness is only 43.3%, and disparities persist among different areas of the state. Rural areas are experiencing difficulty improving their preparedness levels, and many FA and critical capacity scores remain low. The findings in this report are subject to at least four limitations. First, the CDC assessment tool was designed to measure preparedness capacity in health departments nationwide serving various types and sizes of jurisdictions; in certain instances, inventory questions might not have been directly applicable to the responsibilities, needs, and capacities of LHDs in Kansas, especially for parts of FA C (laboratory capacity) and E (communication and information technology). Second, all information analyzed was self-reported, and no answer validation or verification occurred. However, the assessment tool has been validated elsewhere (2), and nearly all the observed changes point consistently to an increase in the preparedness capacity index scores, with few internal inconsistencies in the survey results. Third, no accepted standards exist for what constitutes adequate preparedness for LHDs. The preparedness capacity indexes and thresholds used in this study were created by local officials and are among the first such measures to be used to assess terrorism preparedness at the local level. Although the use of these indexes allows easy comparisons between the 2002 and the 2003 surveys and among groups of respondents, the criteria used to compute the indexes are arbitrary. The adoption of different criteria, or the movement up or down of the achievement thresholds for individual questions, could produce different results. Finally, all indexes were computed by using unweighted means, and because the number of elements that compose each index varies, single responses might affect summary indexes disproportionately. While determining the optimal level of preparedness capacity for LHDs in Kansas was not an objective of this study, the findings suggest that when attention and funds are allocated, preparedness capacity improves in specific and measurable ways. Investments in such a critical field as public health preparedness should be accompanied by consistent evaluation methods. For this purpose, CDC is shifting attention from assessment of public health capacity to evaluation of actual public health performance that can be expected as a result of the increased capacity. These findings also demonstrate that when the same measurable indicators are used repeatedly, important information can be obtained regarding successes and areas in need of further improvement. References
Table 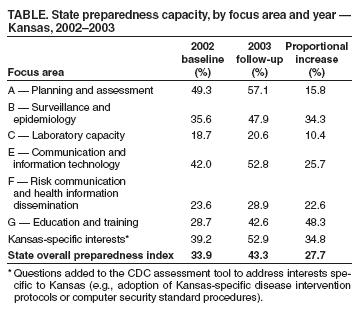 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 5/12/2005 |
|||||||||
|