 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Rapid Assessment of the Needs and Health Status of Older Adults After Hurricane Charley --- Charlotte, DeSoto, and Hardee Counties, Florida, August 27--31, 2004On August 13, 2004, Hurricane Charley, a Category 4 storm with sustained winds of 145 mph, made landfall at a Gulf of Mexico barrier island in Florida, resulting in an estimated 31 deaths statewide and extensive property damage in Charlotte, DeSoto, and Hardee counties. The Florida Department of Health (FLDOH) requested that CDC conduct a rapid needs assessment of older adults (i.e., aged >60 years) because this vulnerable age group constitutes a substantial proportion of the population in the most severely affected counties (Charlotte County [43% older adult residents of 141,627 total population], DeSoto County [24% of 32,209], and Hardee County [18% of 36,938]) (1). This report summarizes the findings and recommendations from three rapid needs assessments in these Florida counties. Older adult residents experienced disruptions in both quality-of-life status and medical care for preexisting conditions (e.g., cardiovascular disease, diabetes, and physical disabilities). On the basis of these findings, recommendations were provided to FLDOH for immediate use in deploying resources for response to Hurricane Charley and in planning responses to future disasters. The objectives of the assessment were to 1) characterize post-hurricane living conditions, 2) identify and evaluate immediate needs (e.g., access to basic services and health care), 3) provide recommendations for managing emergency response and recovery, and 4) provide expertise on disaster response and training on rapid needs assessment. Separate assessments were conducted in each county because Charlotte, DeSoto, and Hardee counties differ in population size, demographics, and socioeconomic status. Census blocks within each county were grouped into clusters of five and weighted by the number of housing units with an older adult resident (1). By using probability proportionate to housing units with an older adult resident, 30 clusters and several replacement clusters were selected without replacement in each county. The clusters were representative of 38,301 (Charlotte), 4,909 (DeSoto), and 3,134 (Hardee) housing units with an older adult resident. Street maps of census blocks were printed and provided to 10 assessment teams. Teams consisted of volunteers (e.g., nurses and epidemiologists) from county health departments and FLDOH and CDC personnel. Teams began in the central area of each assigned cluster, chose a random direction in which to proceed, moved sequentially along roadways to identify individual housing units, and attempted to conduct an interview with a household representative at seven homes with an older adult resident in each cluster. Survey teams conducted interviews in Charlotte County on August 27, in DeSoto County on August 28, and in Hardee County during August 29--31. Assessment teams administered a questionnaire to household respondents about 1) dwelling type and structural damage; 2) utilities and services (e.g., water, electricity, telephone, garbage, and transportation); 3) injuries and illnesses incurred since the hurricane; 4) the impact of the hurricane on home health-care services (e.g., meal service, dressing changes, and delivery of supplies such as oxygen) and social support networks (e.g., group memberships, church activities, and regular social activities); 5) access to food and finances for immediate needs; and 6) the use of disaster-relief services. Household respondents also were asked about whether any older adult household members had preexisting disabilities, impairments, or health conditions and whether the hurricane exacerbated these conditions or prevented receipt of routine care. EpiInfo 2002 was used for data entry, and weighted cluster analysis was conducted by using SAS and SUDAAN. For immediate needs pertaining to public health and medical issues and general assistance (e.g., roof repair and yard cleanup), interviewers completed referral forms and forwarded them to local emergency management agencies or the Sarasota Health Recovery Team Operations Center (SHRTOC) for appropriate response. Assessment teams obtained information from 198, 192, and 205 households in Charlotte, DeSoto, and Hardee counties, respectively (Table). Preliminary findings follow. Charlotte County. Nearly 93% of households reported hurricane-related damage. Approximately 90% of households were in compliance with a public health advisory for drinking bottled water. One third of households reported a disruption in social support networks. Among households having at least one older adult household member with a preexisting medical condition, one third reported that at least one older adult's medical condition worsened because of the hurricane, and 28% of households reported that at least one older adult was prevented from receiving routine care for a preexisting condition. DeSoto County. Nearly 48% of households surveyed were in mobile homes, and 19% of all households reported uninhabitable homes. Approximately 54% of households were still awaiting restoration of sanitation services at the time of the survey. Bottled (81%) and well (17%) water were the most common drinking water sources. Hardee County. Nearly 45% of households with an older adult resident were in single-family homes, and 53% were in mobile homes. The majority of households surveyed (80%) were in damaged but habitable homes; 12% were in damaged and uninhabitable homes. Electricity and water had been restored to the majority of households (94%) at the time of the survey. Bottled (66%), well (20%), and public (14%) water were the most common sources of drinking water. Nine percent of households reported at least one older adult who did not have access to prescription medications. Reported by: B Little, MPH, Sarasota County Health Dept, Sarasota; J Gill, PhD, Florida Dept of Health. J Schulte, DO, Epidemiology Program Office; S Young, MPH, J Horton, MS, L Harris, MPH, D Batts-Osborne, MD, C Sanchez, MD, J Malilay, PhD, Div of Environmental Hazards and Health Effects, National Center for Environmental Health; T Bayleyegn, MD, EIS Officer, CDC. Editorial Note:Preliminary results of the assessments identified the needs and effects of the hurricane on preexisting medical conditions and health care for households with an older adult resident in the three counties. These preliminary findings suggest that local health-care providers and public health agencies should 1) accelerate restoration of medical-care services, including improving access to prescription medications; 2) improve sanitation services (i.e., garbage and storm-debris pickup); 3) improve awareness of public health advisories concerning use of bottled water for drinking and cooking until local sources (e.g., well water and public supplies) are determined to be safe; and 4) encourage reconnecting to social networks that offer support during the post-hurricane recovery period. The findings in this report are subject to at least three limitations. First, logistic difficulties prevented interviewers from reaching certain areas targeted for the assessment. Some clusters were inaccessible because of muddy, impassable roads, and locally available maps did not have the level of detail necessary to navigate to all clusters mapped by using the 2000 U.S. Census. In these instances, replacement clusters were substituted. Second, although probability-based cluster selection increased the likelihood of survey teams encountering households with a resident aged >60 years, it did not guarantee that seven interviews could be completed in each cluster. As a result, the desired 210 interviews were not completed in each assessment. Finally, this assessment represents the first time the cluster survey technique described here has been used to identify the needs of a specific subgroup within an affected population. Additional inquiry is necessary to determine the suitability of this approach. Rapid needs assessments are critical in evaluating the health status and immediate needs of communities affected by disasters (2--4). A modified cluster-sampling method estimates both the percentage of the population and the number of households with a particular need (5,6). Data obtained through rapid needs assessments are used by decision-makers to identify where to provide immediate services and for planning for future post-disaster relief services. These assessments after Hurricane Charley provided critical information to SHRTOC and FLDOH about the status of households with older adult residents in hurricane-affected communities. SHRTOC is sharing the results of the assessments with the three counties and will use results in response planning and improving public health communications in affected communities. If the assessments had been performed earlier (e.g., 3--5 days after the hurricane) instead of 10--14 days after, results might have been useful in guiding deployment decisions involving medical responders and mental health counselors. Follow-up to the initial assessments should be performed to ensure that identified needs have been addressed and to measure restoration of services and quality of life among older adults. Acknowledgment This report is based, in part, on contributions by the Hurricane Charley Rapid Needs Assessment Interview Teams. References
Table 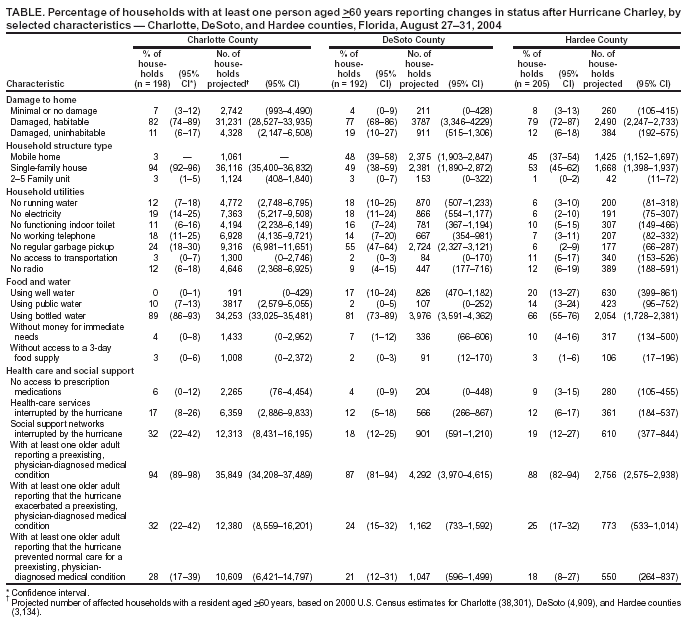 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 9/16/2004 |
|||||||||
This page last reviewed 9/16/2004
|