 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Nonfatal and Fatal Drownings in Recreational Water Settings --- United States, 2001--2002Drowning is the seventh leading cause of unintentional injury deaths for all ages and the second leading cause of all injury deaths in children aged 1--14 years (1). Many of these injuries occur in recreational water settings, including pools, spas/hot tubs, and natural water settings (e.g., lakes, rivers, or oceans). To examine the incidence and characteristics of nonfatal and fatal unintentional drownings in recreational water settings, CDC analyzed 2001--2002 data from the National Electronic Injury Surveillance System All Injury Program (NEISS-AIP) and National Vital Statistics System (NVSS) death certificate data from 2001. This report summarizes that analysis, which indicated that, during 2001--2002, an estimated 4,174 persons on average per year were treated in U.S. hospital emergency departments (EDs) for nonfatal unintentional drowning injuries in recreational water settings. Approximately 53% of persons required hospitalization or transfer for more specialized care. During 2001, a total of 3,372 persons suffered fatal unintentional drownings in recreational settings. Nonfatal and fatal injury rates were highest for children aged <4 years and for males of all ages. To reduce the number of drownings, environmental protections (e.g., isolation pool-fences and lifeguards) should be adopted; alcohol use should be avoided while swimming, boating, or water skiing or while supervising children; and all participants, caregivers, and supervisors should be knowledgeable regarding water-safety skills and be trained in cardiopulmonary resuscitation (CPR) (Box). NEISS-AIP is operated by the U.S. Consumer Product Safety Commission and collects data about initial visits for all types and causes of injuries treated in U.S. EDs (2). Data are drawn from a nationally representative subsample of 66 hospitals out of 100 NEISS hospitals that were selected as a stratified probability sample of hospitals in the United States and its territories; the hospitals have a minimum of six beds and a 24-hour ED. NEISS-AIP provides data on approximately 500,000 injury- and consumer product--related ED cases each year. Death certificate data were obtained from NVSS (3). Rates were calculated by using 2001 and 2002 U.S. Census bridged-race population estimates from the National Center for Health Statistics (1). Nonfatal cases were identified in the NEISS-AIP data if they had a precipitating or immediate cause of "drowning/near-drowning," a diagnosis of "submersion," or the mention of "drown" or "submersion" in the comment field. Cases were reviewed, and any intentional or nonrecreational drownings (e.g., in bathtub, bucket, toilet, or related to motor-vehicle crash) were excluded. In addition, because deaths are not captured completely by NEISS-AIP, persons who were dead on arrival or who died in the ED also were excluded. Each case was assigned a sample weight on the basis of the inverse probability of selection; these weights were summed to provide national estimates of nonfatal drownings. Estimates were based on weighted data for 206 patients with drowning injuries in recreational water settings treated at NEISS-AIP hospital EDs during 2001--2002. Two years of data were necessary to provide stable rates. Confidence intervals (CIs) were calculated by using a direct variance estimation procedure that accounted for the sample weights and complex sample design. Estimates for the 2 years were annualized by dividing the sample weights by two. Because of the small sample size, percentages of nonfatal injuries by location (Figure) were based on unweighted data for NEISS-AIP cases and, thus, are not nationally representative. Drowning deaths in recreational water settings were defined as those for which the underlying cause recorded on death certificates by a physician or coroner was one of the following International Classification of Diseases, Tenth Revision (ICD-10) codes: W67--W74, V90, or V92. Because NVSS is a complete census of all deaths, it is not subject to sampling error; however, CIs were calculated to account for random error (3). This report uses the terms "nonfatal drowning" and "fatal drowning" to describe the events captured by using these methods. During 2001--2002, an estimated 4,174 persons on average were treated annually in U.S. EDs for nonfatal unintentional drowning injuries in recreational settings, and 3,372 persons died in 2001 (Table). Children aged <4 years accounted for nearly 50% of the ED visits, and children aged 5--14 years an additional 25%. Fatal rates also were highest in children aged <4 years. The nonfatal drowning rate for males was nearly twice that for females, and the fatal rate for males was almost five times that for females. These injuries in recreational settings occurred most commonly on weekends (Friday--Sunday), accounting for 56% of nonfatal injuries, and in summer months (June--August), accounting for 56% of nonfatal injuries and 51% of fatalities. For those cases that were known to occur either in a pool or natural water setting, an estimated 75% of nonfatal injuries occurred in pools, whereas 70% of the fatalities occurred in natural water settings. Nearly 40% of reported nonfatal injuries to children aged <4 years occurred in private pools; both nonfatal and fatal injuries in natural water settings increased with age (Figure). Approximately 53% of ED-treated patients required hospitalization or transfer to another hospital for more specialized care. Reported by: J Gilchrist, MD, Div of Unintentional Injury Prevention; K Gotsch, MPH, G Ryan, PhD, Office of Statistics and Programming, National Center for Injury Prevention and Control, CDC. Editorial Note:Drownings have been a leading cause of injury death in the United States for decades (1). The findings in this report are consistent with previous reports of fatal drownings, indicating that small children are at highest risk, particularly around residential pools (4). In addition, males are at higher risk than females, possibly because of their choices of activities with higher risk and increased use of alcohol (5). This report is the first to provide national estimates of the number and characteristics of nonfatal unintentional drowning injuries in recreational settings treated in EDs. During 2001--2002, approximately 4,000 persons were treated annually for nonfatal drownings, with approximately 50% requiring hospitalization or transfer for more specialized care, compared with 5% hospitalized or transferred for all unintentional injuries (1). Nonfatal drownings put victims at risk for infection of the respiratory tract and complications associated with lack of oxygen, including permanent brain damage. Because treatment measures such as advanced in-hospital care do not seem to substantially affect the outcome of drowning injuries (6), primary and secondary prevention strategies are critical to reducing morbidity and mortality associated with these injuries. Primary prevention aims to decrease unintentional entry into the water, which is especially important in preventing drowning injuries in children aged <4 years that commonly occur when unintended access to residential pools is possible (4). Four-sided isolation pool-fencing and other barriers (e.g., weight-bearing pool covers, automatic door locks, and alarms) are necessary to prevent drownings when lapses in supervision occur (7). Once a person is in the water, secondary prevention measures can avert drownings. Strategies such as consistently using personal flotation devices when on or around the water and avoiding use of alcoholic beverages are especially relevant for those involved in boating (8). In addition, swimming instruction and water-safety training can prepare a participant to deal with hazardous aquatic environments (e.g., rip currents, waves, and underwater obstacles like riverbed rocks). Participants can further reduce risk by choosing swimming sites that have lifeguard services (9); however, lifeguard services often are not feasible at natural water sites. Environmental modifications (e.g., lakefront slope gradients to prevent sudden, unseen underwater drop-offs) at natural water sites can help prevent drownings (9). Finally, immediate bystander-initiated CPR, before the arrival of first responders, has been associated with improved outcomes (10). The findings in this report are subject to at least four limitations. First, whereas fatalities occurring in EDs are excluded from the nonfatal data presented, those occurring during or after hospitalization were not excluded; data for fatal and nonfatal drownings might not be mutually exclusive. Second, limited data were available regarding circumstances and possible use of prevention strategies (e.g., life jackets, fencing, or CPR). Third, although drowning risks vary at the state and local levels, NEISS-AIP is designed to provide only national estimates and does not provide state or local estimates. Finally, although the extent of exposure to recreational water settings might vary by age, sex, season, skill level, or other factors, these data were not available; as a result, the analysis did not account for exposure. Because even nonfatal drownings can be serious, with many requiring hospitalization and some resulting in brain damage or other long-term adverse effects, prevention is critical. Participants, parents, caregivers, and supervisors should be aware of the hazards, use appropriate prevention strategies, and be prepared with the skills to save lives in the event of emergencies. Acknowledgments This report is based on data contributed by T Schroeder, MS, C Downs, A McDonald, MA, Div of Hazard and Injury Data Systems, U.S. Consumer Product Safety Commission. E Sogolow, PhD, Div of Unintentional Injury Prevention; JL Annest, PhD, Office of Statistics and Programming, National Center for Injury Prevention and Control, CDC. References
Table 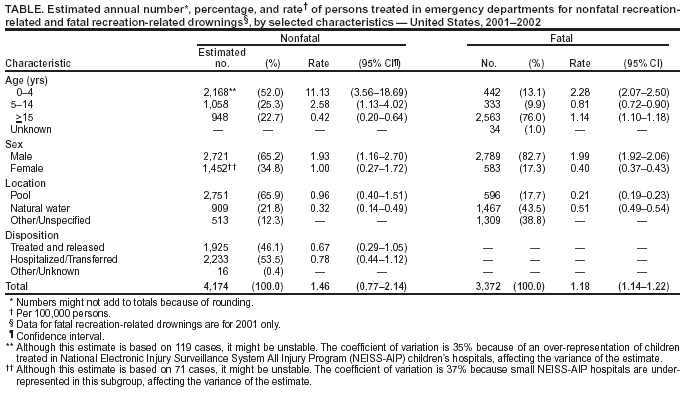 Return to top. Figure 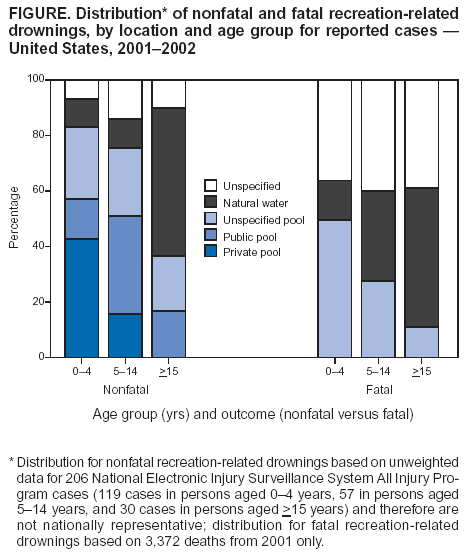 Return to top. Box 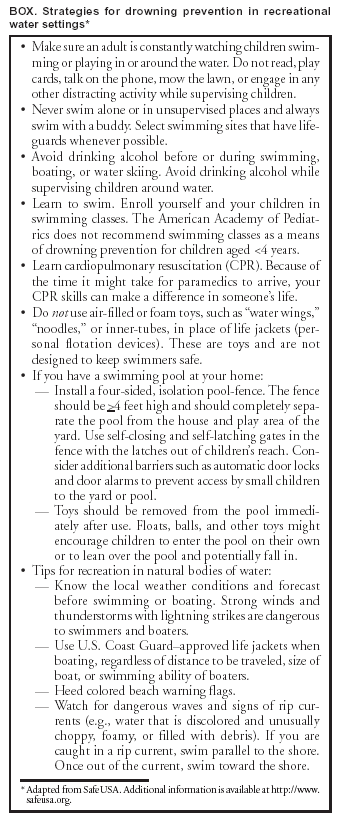 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 6/3/2004 |
|||||||||
This page last reviewed 6/3/2004
|