|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
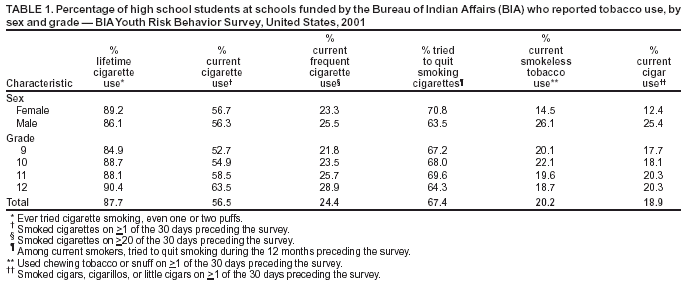
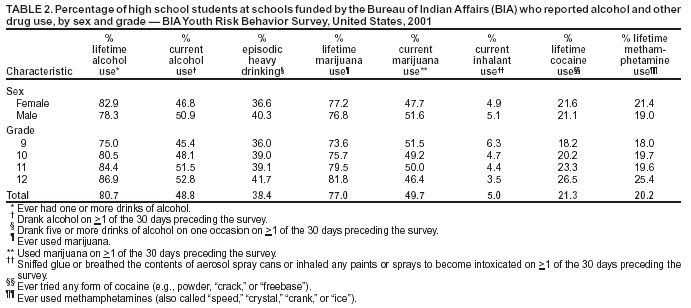
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Tobacco, Alcohol, and Other Drug Use Among High School Students in Bureau of Indian Affairs--Funded Schools --- United States, 2001In the United States, use of alcohol and other drugs is associated with the three leading causes of death and disability (i.e., unintentional injuries, primarily from motor vehicle crashes; suicide; and homicide) among American Indian/Alaska Native (AI/AN) persons aged 15--24 years (1), and tobacco use is associated with the two leading causes of death (i.e., heart disease and cancer) (1,2) among AI/AN adults. This report presents data about the prevalence of tobacco, alcohol, and other drug use among high school students at schools funded by the Bureau of Indian Affairs (BIA). The findings indicate that a substantial number of these students engage in behaviors that put them at risk for premature death and disability and underscore the need for expanded health education and counseling programs and policies in AI communities and BIA-funded schools. The Youth Risk Behavior Surveillance System measures the prevalence of health-risk behaviors among adolescents through representative school-based surveys conducted at the national, state, and local levels and among certain populations. In 2001, BIA conducted the Youth Risk Behavior Survey (YRBS) among students in grades 9--12 attending schools funded by BIA. BIA-funded schools (i.e., day schools, boarding schools, and dormitories) are located on 63 reservations in 23 states. These schools are operated either by BIA or by AI tribes or tribal organizations under contract or grant with BIA. BIA funds 185 schools with approximately 50,000 students in kindergarten and grades 1--12, including approximately 8,500 high school students. Principals in participating schools sent information about YRBS to parents, including a permission form. The survey was administered by using standard YRBS procedures (3). Students voluntarily completed an anonymous, self-administered questionnaire that included questions about tobacco, alcohol, and other drug use (i.e., marijuana, inhalant, cocaine, and methamphetamine use). For each substance, lifetime use was defined as ever having used the substance, and current use was defined as having used the substance on >1 day during the 30 days preceding the survey. Current frequent cigarette use was defined as having smoked on >20 of the 30 days preceding the survey. Among current smokers, tried to quit smoking was defined as trying to quit during the 12 months preceding the survey. Episodic heavy drinking was defined as drinking at least five alcohol drinks on at least one occasion on >1 day during the 30 days preceding the survey. For this survey, BIA attempted a census of high school students; all BIA-funded high schools and all students in grades 9--12 attending those schools were eligible to participate. However, four small BIA-funded schools with <10 students in grades 9--12 were excluded because of concerns related to student privacy. Questionnaires were completed by 5,654 (66.4%) of 8,511 eligible students from 66 (91.7%) of 72 eligible schools. The overall response rate was 60.8%. Data were weighted to provide national estimates of AI high school students attending BIA-funded schools. The majority of students reported lifetime (87.7%) and current (56.5%) cigarette use, and 24.4% reported current frequent cigarette use (Table 1). More students in grade 12 reported lifetime, current, and frequent cigarette use than students in grade 9. Among current smokers, more than two thirds (67.4%) reported attempting to quit smoking during the 12 months preceding the survey, with more females than males reporting a quit attempt. Approximately one in five students reported current use of smokeless tobacco (20.2%) and cigars (18.9%). More males than females reported current smokeless tobacco and cigar use. Lifetime alcohol use was reported by 80.7% of students, current alcohol use by 48.8%, and episodic heavy drinking by 38.4%. Current alcohol use and episodic heavy drinking were more common among males than females (Table 2). Rates of lifetime alcohol use, current alcohol use, and episodic heavy drinking increased with grade level. More than three fourths (77.0%) of students reported lifetime marijuana use, and approximately half (49.7%) reported current marijuana use. Approximately one fifth of students reported lifetime cocaine (21.3%) and methamphetamine (20.2%) use. Lifetime marijuana, cocaine, and methamphetamine use increased by grade; however, current marijuana and inhalant use were more common among students in grade 9 than grade 12. Reported by: L Shaughnessy, MA, Office of Indian Education Programs, Bur of Indian Affairs. S Everett Jones, PhD, Div of Adolescent and School Health, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:The findings in this report indicate that a substantial number of high school students at BIA-funded schools engage in behaviors that put them at risk for premature death and disability. The rates of cigarette smoking; smokeless tobacco use; and marijuana, cocaine, and methamphetamine use are substantially higher among BIA students than among high school students nationwide; rates of current cigar, alcohol, and inhalant use are similar among BIA students and students nationwide (3). The findings in this report are subject to at least two limitations. First, these data represent only AI students attending BIA-funded schools with >10 students enrolled in grades 9--12 and therefore are not representative of all AI high school students. Second, because behaviors were self-reported, the extent of underreporting or overreporting of behaviors cannot be determined; however, the survey questions have demonstrated good test-retest reliability among non-AI high school students (4). BIA efforts to reduce adolescent health-risk behaviors include training school staff to implement school health programs and establishing outdoor adventure--based counseling. Funds received through the Safe and Drug Free Schools and Communities Act* are distributed to all BIA-funded schools. Since 1997, BIA and CDC have supported character education, teacher training, and school-based programs to prevent cigarette, alcohol, and other drug use. BIA also has established a therapeutic model program in three BIA-funded boarding schools to develop schoolwide systems of behavior supports and interventions to reduce high-risk behaviors and improve students' academic performance. The BIA YRBS can be used to track progress in reducing tobacco, alcohol, and other drug use among high school students who attend BIA-funded schools. If these survey efforts are maintained, BIA and AI tribes and villages served by BIA-funded schools will have data to monitor the effectiveness of tobacco-, alcohol-, and other drug-use prevention and counseling programs for young persons. References
* Title IV (20 U.S.C. 7101 et seq.) as amended by Public Law 107-110 (January 8, 2002).
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 11/6/2003 |
|||||||||
This page last reviewed 11/6/2003
|