|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
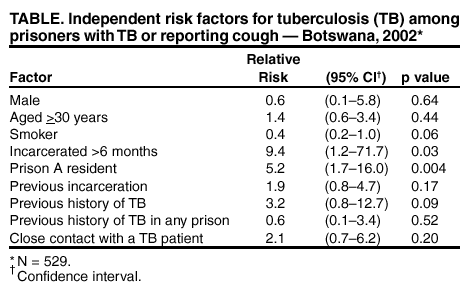
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Rapid Assessment of Tuberculosis in a Large Prison System --- Botswana, 2002Prisons are settings in which tuberculosis (TB) transmission occurs, and TB rates in prisons are often five to 10 times higher than national rates (1). Data on the prevalence of TB in prisons in Africa are limited; however, studies from Malawi, Ivory Coast, and Tanzania that used active screening found TB rates >10 times higher than national rates (2--4). During 1989--2001, TB rates in Botswana increased threefold, from 199 cases per 100,000 population to 620 (Botswana National TB Program, unpublished data, 2002). This increase has been associated with the human immunodeficiency virus (HIV) epidemic (5). In Botswana, prisoners are not screened routinely for TB. To determine the prevalence of TB and drug-resistant TB in the Botswana prison system and to improve future screening for TB among prisoners and guards, CDC, in collaboration with the Botswana Ministry of Health and the Division of Prisons and Rehabilitation, screened prisoners and guards at four prisons during April--May 2002. This report summarizes the results of the survey, which indicate a high point prevalence of TB among prisoners in Botswana of 3,797 cases per 100,000 population and support the need for improved screening. New and existing pulmonary TB cases among prisoners aged >16 years and all guards at the four locations in the capital city (Gaborone) prison system were asked to complete an active case-finding questionnaire-based survey. Persons who consented to screening were interviewed privately to ascertain demographic characteristics, prison incarceration or work history, previous medical history, and whether symptoms consistent with pulmonary TB were present. Persons who reported a current cough were asked to provide three separate expectorated sputum samples, which were sent to the national TB laboratory for sputum smear microscopy (all specimens) and mycobacterial culture (the first two specimens). Drug susceptibility testing (DST) for first-line drugs (isoniazid, rifampin, ethambutol, and streptomycin) was performed on one isolate per patient. Sputum was not obtained from those without cough. Persons who reported a cough but were unable to produce sputum were scheduled for chest radiographs, which were obtained within 1 month from persons with cough persistent at the time of examination. Cases were classified as smear-positive, smear-negative and culture-positive, or smear--not done with chest radiograph consistent with pulmonary TB (i.e., clinical). Prisoners and guards who had TB diagnosed were started on short-course, directly observed therapy according to the Botswana National TB Program protocol (6). TB patients also were offered voluntary counseling and testing (VCT) for HIV. During April--May 2002, a total of 1,027 (88%) of 1,173 prisoners and 263 (91%) of 288 guards were interviewed. Acceptance of screening by prisoners and guards was similar by prison location. The majority of prisoners were men (96%), from Botswana (87%), and incarcerated for the first time (83%). The median age was 26 years (range: 16--78 years), and the median duration of incarceration was 15 months (range: 1 day--22 years). A total of 509 (50%) prisoners reported cough; 371 (73%) provided sputum samples, and 33 (6%) who were unable to produce sputum had chest radiographs; 17 (52%) of the 33 radiographs showed abnormalities (15 infiltrates and two with hilar adenopathy). However, because the majority of these patients improved (by resolution of cough) without TB therapy (11 [79%] of 14 with follow-up) and were not started on TB treatment on the basis of the chest radiograph results, none was counted as a TB patient. A total of 39 (4%) prisoners had TB; 20 (51%) were receiving treatment at the time of screening, and 19 (49%) had TB detected by screening. Of the 19, eight (42%) were smear-positive, and 11 (58%) were smear-negative and culture-positive. Mycobacterium tuberculosis isolates from 13 prisoners underwent DST; two (15%) were resistant to isoniazid only. Of the 39 patients with TB who were offered VCT, 14 (36%) declined, including three who reported previously testing HIV-positive. Among 20 prisoners with results available, six (30%) were HIV-positive. HIV test results were unknown for five prisoners. Although prisoners moved into and out of the prison system frequently, the size of the overall prison population remained stable during the survey period. The minimum point prevalence of TB among prisoners was 3,797 cases per 100,000 (39 cases among 1,027 prisoners). Independent risk factors for TB among prisoners reporting cough or those on TB treatment at screening initiation (with or without cough) included incarceration for >6 months and residence in prison A (Table). Of the 263 guards who were screened, 45 (17%) reported cough; of these, sputum was obtained from 25 (56%). Five (2%) guards were being treated for TB at the time of screening. Two cases (both sputum smear-negative and culture-positive) were identified through screening. Among guards who reported a cough but were unable to produce sputum, six underwent chest radiography, of which five (83%) were abnormal (all infiltrates). However, none was classified as having TB. The isolates from two guards were available for DST; one was fully susceptible, and one was resistant to isoniazid, ethambutol, and streptomycin. The minimum point prevalence of TB among guards was 2,662 cases per 100,000 (seven cases among 263 guards). Observation in the prison documented crowded cells (a minimum of one prisoner/m2 of space with only natural ventilation through small windows); the one prison sick ward (<15m2) had four beds and no ceiling fans. The kitchen and other work sites in which prisoners congregated frequently had no mechanical ventilation. On the basis of the high prevalence of TB identified, CDC recommended several interventions, including 1) screening for TB at prison entry or transfer and periodically thereafter (e.g., annually) using a symptom-based questionnaire, 2) contact investigations of newly identified smear-positive cases, 3) assessment of administrative and environmental measures to reduce ongoing transmission within the prison (7), and 4) implementation of isoniazid preventive therapy among HIV-infected prisoners and guards according to existing Ministry of Health guidelines. Reported by: EA Wang, CH McCrann, M Notha, BOTUSA Project; MJ Mwasekaga, National TB Reference Laboratory; RA Mwansa, MD, Botswana Ministry of Health. NJ Binkin, MD, National Institute of Health, Rome, Italy. KF Laserson, ScD, CD Wells, MD, EA Talbot, MD, Div of TB Elimination, National Center for HIV, STD, and TB Prevention; AM Andre, MD, LJ Nelson, MD, EIS officers, CDC. Editorial Note:TB is a major health problem for prisoners and guards in Botswana, and TB point prevalence was four to six times higher than annual TB incidence of 620 per 100,000 population for the civilian population. Although DST was performed on only 15 isolates, drug resistance was infrequent, probably reflecting the relatively low level of drug resistance in Botswana (8). Longer duration of incarceration and residence in prison A were the strongest risk factors for TB. Symptom screening of prisoners and guards helped to identify 21 new cases of TB in prisons. Only 40% of TB cases were sputum smear-positive at diagnosis, and chest radiography did not identify additional cases. However, in settings in which mycobacterial cultures are difficult to obtain, chest radiography might be a useful screening tool in persons who are sputum smear-negative but have persistent symptoms (9). The findings in this report are subject to at least three limitations. First, sputum was obtained only from persons who reported cough; as a result, TB cases might have been missed. Second, some patients with abnormal chest radiographs might have been misclassified as non-TB cases, causing the prevalence of TB to be underestimated. Finally, this survey did not compare different screening approaches; therefore, direct comparisons cannot be made among different screening modalities. Because the risk for TB was greater with a longer duration of incarceration and within one facility, screening at entry alone would be insufficient to control transmission, and ongoing screening would be useful. Because TB also occurred among guards, this population also could benefit from periodic screening and inclusion in contact tracing. Enclosed spaces, such as those observed in this prison system, and inadequate ventilation are associated with a higher risk for transmission (10). To further characterize these risks, a detailed environmental assessment of prison facilities in Botswana and a subsequent infection-control plan are warranted. Acknowledgments This report is based on assistance provided by the National TB Reference Laboratory, Div of Prisons and Rehabilitation, Botswana Ministry of Health. National Institute of Occupational Safety and Health; P Kilmarx, MD, R Manchanda, A Davis, P Letsatsie, B Chengeta, T Mokatse, BOTUSA Project; P Jensen, PhD, Div of TB Elimination, National Center for HIV, STD, and TB Prevention, CDC. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
Page converted: 3/27/2003
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 3/27/2003