Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Notice to Readers: Alcohol Involvement in Fatal Motor-Vehicle Crashes
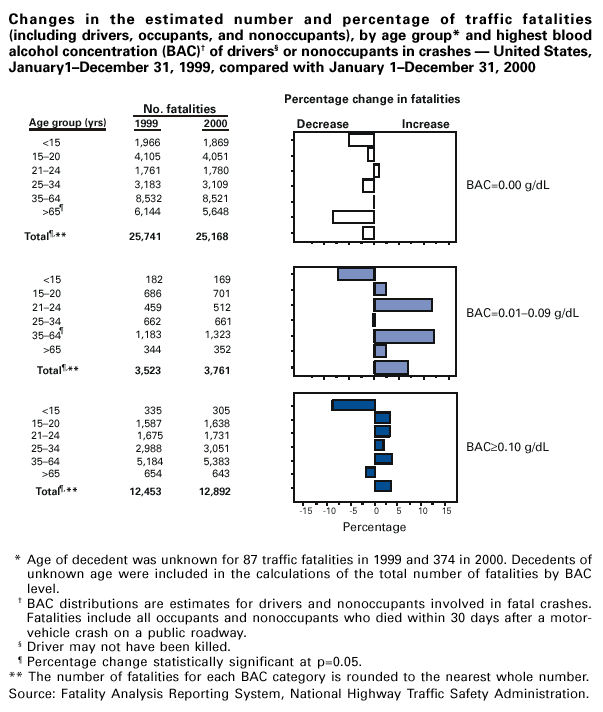
---United States, 1999--2000
The following table compares alcohol involvement in fatal motor-vehicle
crashes by age group and blood alcohol concentration (BAC) levels for 1999 and 2000. A
fatal crash is considered alcohol-related by the National Highway Traffic
Safety Administration (NHTSA) if either a driver or nonoccupant (e.g., pedestrian) had a
BAC of >0.01 g/dL in a police-reported traffic crash. Because BACs are not available for
all persons in fatal crashes, NHTSA estimates the number of alcohol-related
traffic fatalities on the basis of a discriminant analysis of information from all cases for
which driver or nonoccupant BAC data are available
(1).
Overall during 1999--2000, the number of alcohol-related traffic fatalities
increased by 4% (95% confidence interval [CI]=2%--7%). For BACs
>0.10 g/dL (the legal limit for intoxication in most states in 1999 and 2000), fatalities increased by 4% (95%
CI=1%--6%); for BACs of 0.01--0.09 g/dL, fatalities increased by 7% (95% CI=2%--12%).
A broad range of public health and traffic safety strategies will be needed to stem
further increases and reduce the number of alcohol-related traffic fatalities
(2).
References
Klein TM. A method for estimating posterior BAC distributions for persons involved
in fatal traffic accidents: final report. Washington, DC: US Department of
Transportation, National Highway Traffic Safety Administration, 1986; publication no. DOT-HS-807-094.
Shults RA, Elder RW, Sleet DA, et al. Reviews of evidence regarding interventions
to reduce alcohol-impaired driving. Am J Prev Med 2001;21(4S):66--88.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites.
Disclaimer
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.