 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Smallpox Surveillance -- WorldwideMMWR 1978;27:8 (January 6, 1978) A total of 3,234 cases of smallpox have been reported from Eastern Africa to the World Health Organization (WHO) in the period January 1-December 6, 1977. Since October 16, 1975 -- more than 2 years ago -- when a case occurred in Bangladesh, smallpox has been detected only in Ethiopia, Kenya, and Somalia, 3 countries which together with Djibouti are linked by the Ogaden Desert to form one epidemiologic unit. To date, the last known case of smallpox occurred in Somalia on October 26 in the Merca District. The source of this case was a known outbreak in the nearby district of Kurtuware. All 211 contacts were traced, revaccinated, and kept under surveillance. There have been no secondary cases. As of December 6, there were 6 pending outbreaks* in Somalia -- the one in Merca and 5 in Bardere. During October and November surveillance in Somalia has been severely hampered by heavy rains that have made it difficult or impossible to travel by vehicle. Since work has had to be continued on foot, there have been some delays in reporting and incomplete search coverage in certain areas. To combat this, personnel have been concentrated in those areas considered to be at highest risk of having undetected foci or where information is most limited. Currently there are 1,670 national staff and 24 WHO epidemiologists involved in the program. Increased mobility with restoration of complete active searches will be necessary to ensure that all foci have been detected. Accordingly, intensified activities are planned during the dry season, January through April 1978. The last known case of smallpox in Ethiopia occurred on August 9, 1976, in El Kere Region. In Kenya, the last case was on February 5, 1977, in the Mandera District. Reported by the World Health Organization in the Weekly Epidemiological Record 52:389-391, 1977 * An outbreak is defined as one or more cases; a pending outbreak is one in which 6 weeks has not elapsed since the onset of rash of the last case. Smallpox Surveillance -- WorldwideMMWR 1978;27:133 (May 5, 1978) As of April 14, 1978, no cases of smallpox have been reported to the World Health Organization (WHO) from anywhere in the world since the last case had onset of rash on October 26, 1977, in Merka town, Somalia. However, a total of 2 years of effective surveillance must elapse before this last endemic area can be confirmed to be smallpox-free. Worldwide, since January 1, 1976, smallpox cases have been detected only in certain areas of Ethiopia, Kenya, and Somalia (Figure_1). One year and 9 months has elapsed since cases were detected in Ethiopia; 1 year and 1 month has elapsed since 5 cases were detected in Kenya after an importation from Somalia; and 6 months has passed since the last case was found in Somalia. With the apparent interruption of transmission of the disease on a global basis, smallpox activities are being directed toward promptly certifying and providing authoritative endorsement of this historic event. In January 1978 the Executive Board of WHO endorsed the recommendations of a consultant group on worldwide certification of smallpox eradication which met in October 1977. Recognizing that this certification is based on verifying that 2 years has elapsed with no case of smallpox being detected by a surveillance system which would have detected any case had it occurred, the recommendations called for the establishment of a Global Commission. This independent group of experts is to monitor and review the following steps to be undertaken in 1978 and 1979: (1) certification by international commissions in the 15 countries not yet visited by commissions; (2) special documentation or visits to be required for 16 countries; (3) the request for statements from other countries declaring their smallpox-free status. If no more cases of smallpox are detected, the countries of Somalia, Ethiopia, Djibouti, Kenya, Yemen, and Democratic Yemen will be eligible for certification in October 1979. These will be the last of the 15 countries to be certified by an international commission, and priority attention is being given to surveillance in these areas. Reported by the World Health Organization in the Weekly Epidemiological Record 53:97-99, 108, 1978. Editorial Note -- 1997William F Foege, MD, Rollins School of Public Health, Emory University, and former Director, CDC. Walter R Dowdle, PhD, Director of Programs, Task Force on Child Survival and Development, and former Deputy Director, CDC. Some things need be done only once in the entire history of the world. The development of smallpox vaccine and the eradication of smallpox disease are on the list. Perspective is elusive, even when one contemplates 20 years without a single case of smallpox in the world. Part of the reason is that we all begin our reading "in the middle of the book." Although the full story that went before can never be known, smallpox eradication became possible, and then inevitable, when Edward Jenner, using his clinical powers of observation over a 25-year period during the 18th century, became convinced that an infection with cowpox could protect against smallpox. He then took the next step, inducing immunity by transferring cowpox from the hand of Sarah Nelmes to the arm of James Phipps -- creating a tool that would change the health of entire populations (1). In a real sense, the history of modern public health started on that day, May 14, 1796. Word spread quickly, despite communication barriers. By 1806, Jefferson was able to visualize the last case of the disease when he wrote to Jenner, "future generations will know by history only that this loathsome disease has existed" (1). It is a sad commentary that it took 170 years to finally organize to accomplish Jefferson's vision. But when it happened, it brought out the best in science and public health. The resolution at the World Health Assembly in 1965 was unanimous and led to excellent cooperation between the United States and the Soviet Union, even in the midst of Cold War politics. The value of WHO, which represented the health needs of every person in the world, was demonstrated. Workers and resources from around the world were organized for use in the areas of greatest need. The public health situation, rather than political concerns, dictated how the program was to be executed. The United States can be proud of its role in this exciting program, contributing hundreds of workers and millions of dollars for the eradication of a disease that no longer involved our nation. Twenty years have passed since the last naturally acquired case of smallpox occurred, as reported in the January 6 and May 5, 1978, issues of MMWR. Smallpox has not re-emerged from an unrecognized human or animal reservoir, from a variolator's store of infected scabs, or infected cadaver, either unearthed or thawed. There continues to be no evidence to support the theory of a "niche" for human pathogens that, when vacated, will be filled by another. Although speculation increased when monkeypox was recognized as causing human disease, fears decreased when monkeypox was shown to have a low secondary attack rate among unvaccinated humans (2). In addition, monkeypox virus, probably arising from a squirrel reservoir, is not ancestral to smallpox virus based on genomic studies (3). The issue of monkeypox again emerged with outbreaks in 1996 (4) and 1997 (5) in the eastern Democratic Republic of the Congo with speculation about the need for smallpox vaccine to provide cross-protection for the populations at highest risks. Such recommendations must be considered carefully because of the adverse risks of the vaccine, particularly in persons who may be immunocompromised by human immunodeficiency virus infection (5). A better understanding of the current epidemiology/epizoology of monkeypox is needed. Smallpox has been eradicated, but the etiologic agent is not extinct. The virus continues to exist in freezers in secure facilities at one institution in the United States and another in the Russian Federation. During the past 10 years, various individuals and three WHO committees have recommended destruction of virus stocks on the grounds that the world needs to be assured that smallpox will never again be a threat to humankind. In opposition to virus destruction are equally strong views that laboratory stocks serve as a counterbalance to terrorism and a source of unknown future benefits to humankind. In May 1996, the World Health Assembly recommended, subject to further review, that all stocks be destroyed in June 1999. The legacy of the smallpox program, beyond eradication, has been enduring and includes the Expanded Program on Immunization (with its remarkable reductions of measles and other vaccine-preventable illnesses), the impending eradication of Guinea worm disease and poliomyelitis, and improved global disease surveillance and public health logistics systems. The growing interest in eradication as a global health strategy led to the creation of the International Task Force for Disease Eradication, which reviewed greater than 80 potential candidate diseases and concluded in 1993 that six were eradicable (6). The science of infectious diseases eradication was the subject of a multidisciplinary Dahlem Workshop in Berlin in March 1997. As a follow-up to the Dahlem Workshop, a conference is scheduled in Atlanta in early 1998 on Global Disease Elimination/Eradication as Public Health Strategies; this conference will explore the potential synergistic relations between disease elimination/eradication and primary health-care programs throughout the world. The health benefits of smallpox eradication have been enormous and the economic benefits satisfying. Because of smallpox eradication, the United States saves more each year than its annual dues to WHO. For the first time, social justice in public health has been achieved, with everyone benefiting from a body of scientific knowledge and experience. The benefits will continue to be enjoyed by every person who will ever be born. "Future generations will know by history only" that world cooperation reached an unprecedented level in the 20th century, making this bequest possible. References
Original reports published with new editorial note in MMWR 1997;46:991-4 (October 24, 1997). Figure_1 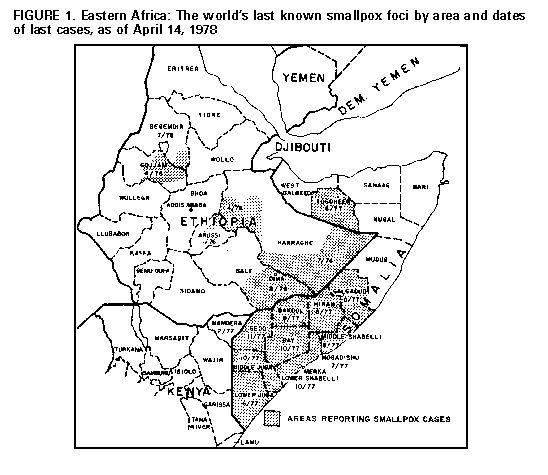 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 04/20/99 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}