 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
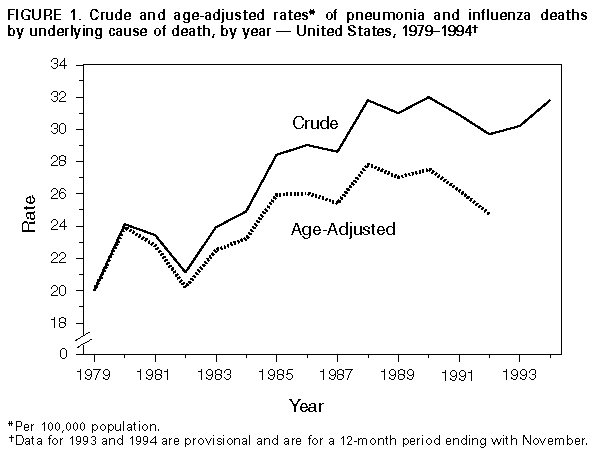
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Pneumonia and Influenza Death Rates -- United States, 1979-1994The combined cause-of-death category pneumonia and influenza (P&I) (International Classification of Diseases, Ninth Revision, codes 480-487) ranks as the sixth leading cause of death in the United States following heart disease, cancer, stroke, unintentional injuries, and chronic obstructive pulmonary disease (1). Changes in the epidemiology of Streptococcus pneumoniae and other recognized respiratory pathogens, the increasing occurrence of drug-resistant microorganisms, and the detection of new respiratory pathogens have heightened awareness of the public health importance of severe respiratory infections (2-5). To characterize the epidemiology of P&I deaths in the United States, CDC further analyzed underlying and multiple cause-of-death mortality files for 1979-1994. This report summarizes the results of this analysis. From 1979 to 1994, the overall crude death rates for P&I (based on underlying cause of death) increased 59%, from 20.0 to 31.8 deaths per 100,000 population Figure_1. From 1979 to 1992 (the most recent year for which age-adjusted data are available), the P&I death rate, age-adjusted to a 1980 standard population, increased 22%, from 20.4 to 24.8. In 1992, persons aged greater than or equal to 65 years accounted for 89% of all P&I deaths. From 1979 to 1992, P&I death rates for persons aged greater than or equal to 65 years increased 44%, from 145.6 deaths per 100,000 population to 209.1. During this period, rates also increased for persons aged 20-44 years; however, the small number of deaths among persons in this age group (2148 in 1992) limited the contribution to the overall trend. To control for the highly variable seasonal contribution of influenza-associated deaths, the trend for mean weekly number of P&I deaths for noninfluenza months (May-October) was analyzed. From 1979 through 1992, age-adjusted P&I death rates during these months increased steadily from 3.1 to 5.0 per 1 million population. Analysis of P&I deaths listed in any position on the death certificate (multiple cause-of-death data) indicated a similar increase. During 1979-1992, the diagnostic code for pneumonia of unspecified etiology (ICD-9 code 486) accounted for most of the overall increase: age-adjusted death rates in this diagnostic category increased 74%. In addition, in 1992, 84% of all P&I deaths were assigned this code, compared with 59% in 1979. Reported by: Childhood and Respiratory Diseases Br, Div of Bacterial and Mycotic Diseases, and Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Mortality Statistics Br, Div of Vital Statistics, National Center for Health Statistics, CDC. Editorial NoteEditorial Note: The findings in this report document the recent increase in mortality attributed to P&I in the United States. This increase reflects both growth in the proportion of persons in older age groups (from 1970 to 1990, the proportion of persons in the United States population aged greater than or equal to 65 years increased from 9.8% to 12.5%) and higher P&I death rates in these age groups. A high proportion of these deaths was attributed to pneumonia of unspecified etiology, which probably includes both pneumonias caused by known pathogens not specified on the death certificate and pneumonias caused by new or unrecognized agents. Changes in the epidemiology of recognized respiratory pathogens (e.g., S. pneumoniae), for which precise diagnoses are difficult to make in clinical settings, may have contributed to the increasing death rate in older persons. Although the proportion of the increase in P&I death rates accounted for by all vaccine-preventable respiratory diseases is unknown, the increased rates also underscore the need for more complete use of pneumococcal and influenza vaccines as recommended by the Immunization Practices Advisory Committee (ACIP) (6,7). One of the national health objectives for the year 2000 is to vaccinate 60% of persons at risk for pneumococcal disease and influenza (objective 20.11) (8). Although coverage levels for influenza vaccinations among persons aged greater than or equal to 65 years have increased (in 1993, 52% reported having received influenza vaccine in the previous year), only 28% reported ever having received the pneumococcal vaccine in 1993 (9). In addition to known but undiagnosed causes of respiratory infection, new or previously uncharacterized agents probably account for some of the increase in age-adjusted death rates attributed to pneumonia of unspecified etiology. For example, since the 1970s, several bacterial and viral agents have been identified as causes of lower respiratory infections, including Legionella pneumophila, Chlamydia pneumoniae, and Sin Nombre virus (the etiologic agent of hantavirus pulmonary syndrome). Recent prospective studies of community-acquired pneumonia have suggested that an etiology cannot be identified in 40%-50% of cases (10), probably reflecting both the lack of sensitive diagnostic tests for some known respiratory pathogens and the occurrence of respiratory infections for which the etiologies have not yet been identified. Based on shifts in the age distribution of the total U.S. population, respiratory infectious diseases among the elderly probably will increase the need for health-care services and require the development of more effective prevention strategies. Improvements in understanding the epidemiology of morbidity and mortality associated with unspecified pneumonias will require further examination of diagnostic and reporting practices for certification of causes of death and analyses of additional data sources (e.g., hospital discharge records). In addition, improved characterization of bacterial and viral causes of pneumonia may result from prospective epidemiologic and laboratory studies, development of more sensitive diagnostic tests, and wider use of available tests. References
+-------------------------------------------------------------------
-------+
|
|
| Erratum: Vol. 44, No. 28
|
|
|
| SOURCE: MMWR 44(41);782 DATE: Oct 20, 1995
|
|
|
| For the article, "Pneumonia and Influenza Death Rates --
United |
| States, 1979-1994," reexamination of the database detected an
error in |
| the age-adjustment procedure used to calculate the weekly mean
pneumonia |
| and influenza (P&I) death rates for noninfluenza periods. The
following |
| corrected paragraph replaces the first paragraph on page 536:
|
| "To control for the highly variable seasonal contribution of
|
| influenza-associated deaths, the trend for mean weekly number of
P&I |
| deaths for the noninfluenza period (weeks 26-39) was analyzed.
From 1979 |
| through 1992, age-adjusted P&I death rates during these weeks
increased |
| from 3.1 to 3.7 per 1 million population. Analysis of P&I deaths
listed |
| in any position on the death certificate (multiple-cause-of-death
data) |
| indicated a similar increase."
|
|
|
+-------------------------------------------------------------------
-------+ Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}