 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
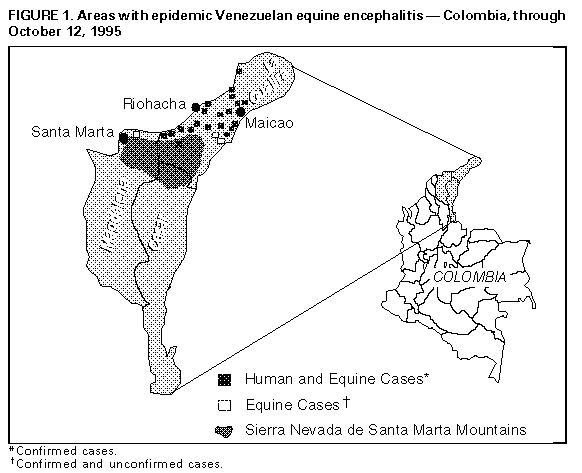
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update: Venezuelan Equine Encephalitis -- Colombia, 1995During September 1-October 12, 1995, a total of 12,403 patient visits for Venezuelan equine encephalitis (VEE) were reported from La Guajira state, Colombia. The actual number of incident cases, estimated from epidemiologic surveys, may exceed 45,000. This report updates the ongoing investigation of this outbreak (1). Household surveys in urban areas of Manaure, Maicao, Riohacha, and Uribia during September 26-October 3 indicated an overall attack rate of 18%, ranging from 13% in Riohacha (the largest of the towns) to 57% in Manaure. In 101 patients in Manaure, Maicao, and Riohacha who sought medical care within 3 days of onset of acute febrile illness, the point prevalence of VEE-specific immunoglobulin M antibody was 45%, providing a minimum estimate of the specificity of the clinical case definition. Of the 18 VEE virus strains isolated from humans, three were identified antigenically as IC-subtype viruses, which have been the principal cause of epizootics in northern South America. Partial nucleotide sequencing of the strains indicated they were closely related to strains isolated from Venezuela earlier in 1995. The outbreak has spread southwest along the coastline at a rate of approximately 3 miles (5 km) each day (Figure_1). In the coastal towns of Manaure, Mayapo, El Pajaro, and Dibulia, entomologic surveys have detected large populations of the vector mosquito Aedes taeniorhynchus. The initiation of mosquito-control programs was followed by declines in emergency department visits for acute febrile illness in Manaure, Maicao, Riohacha, and Uribia. In addition, entomologic surveys indicated 99%-100% declines in Ae. taeniorhynchus larval densities after breeding sites were treated with Bacillus sphaericus (a larvicide). In the inland region south of Maicao, the outbreak has extended to the municipality of Riohacha, near El Cerrejon coal mine in Hatonuevo. Surveys in Maicao and the south of La Guajira Department have identified extensive breeding habitats for Psorophora confinnis and abundant larvae. Households in Maicao, Riohacha, and Uribia that had more than one case were studied to determine whether secondary person-to-person transmission had occurred. A secondary case was defined as onset of acute febrile illness 1-5 days after onset of illness in the first case(s) in the household. Primary cases occurring within 5 days of the interview were excluded. The apparent secondary attack rate was 5% (50 of 992). Public health efforts have focused on limiting the spread of the outbreak from La Guajira peninsula to the Magdalena Valley to the south at passes formed by the Sierra Nevada de Santa Marta Mountains (Figure_1). Ongoing active surveillance of all hospitals in La Guajira through October 12 indicated no evidence of human cases in the southern part of the state. Unconfirmed equine cases were reported near Santa Marta, but no human cases acquired in Magdalena have been confirmed. Sporadic equine deaths in Cordoba, Cesar, and Magdalena states have been confirmed serologically as cases of eastern equine encephalitis. In the area beyond the advance of the outbreak (Figure_1), approximately 5000 equines in La Guajira have been vaccinated with TC-83 vaccine; in neighboring Magdalena and Cesar states, 20,000 and 70,000 equines, respectively, have been vaccinated. Reported by: E Daza, I Lopez, A Alcala, A PatiNo, V Frias, La Guajira Health Svc; G Alvarez, MA Garcia, V RiaNo, Vector-Borne Disease Control Program; R Rodriguez, Ministry of Health; J Boshell, Virology Laboratory, VA Olano, E Martinez, LI Villarreal, Entomology Laboratory, LA Diaz, F Rivas, V Cardenas, Field Epidemiology Training Program, National Institute of Health, Colombia. JF Smith, GV Ludwig, B Roberts, US Army Medical Research Institute for Infectious Diseases, Frederick, Maryland. R Rico-Hesse, Yale Arbovirus Research Unit, Yale Univ, New Haven, Connecticut. S Weaver, Medical Br, Univ of Texas, Galveston, Texas. Div of Vector-Borne Infectious Diseases, National Center for Infectious Diseases, CDC. Editorial NoteEditorial Note: Although the VEE outbreak has spread rapidly through La Guajira, control measures have contained the outbreak within this northern-most state of Colombia, with no evidence of human cases in adjoining Magdalena and Cesar states. Equine vaccination creates an immune barrier against the spread of the virus by removing the most important vertebrate amplifying host from the epizootic transmission cycle. Larvicidal treatment of breeding sites reduces the number of vector mosquitoes, but its continued effectiveness may be difficult to maintain during the wet season -- which in La Guajira usually lasts through November. VEE appeared in Venezuela in April 1995 and spread westward, with the first cases in Colombia recognized in August at the common border of the two countries. The virus most likely was transferred in a viremic equine or human and spread from there to the western coast of La Guajira. Comparisons of viral strains from Colombia and Venezuela indicate a close genetic relation (2). Because VEE virus has been recovered from pharyngeal cultures in 40% of patients (3) and aerosols of VEE virus have infected laboratory personnel, direct human-to-human transmission of VEE virus may be possible. However, it is unknown whether infectious VEE aerosols or respiratory droplets can be produced by infected humans. Human-to-human transmission by mosquitoes may occur during some epidemics, as suggested in previous outbreaks (4); however, the household survey in La Guajira found no evidence of direct person-to-person transmission. References
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}