|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
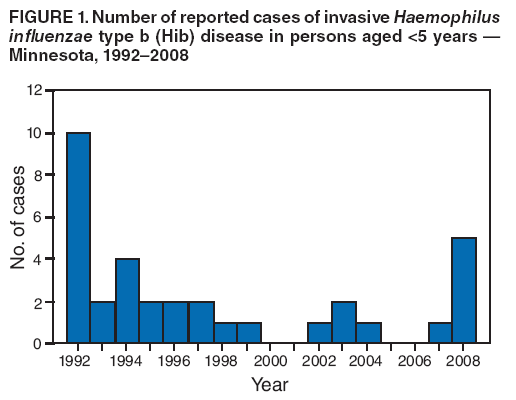
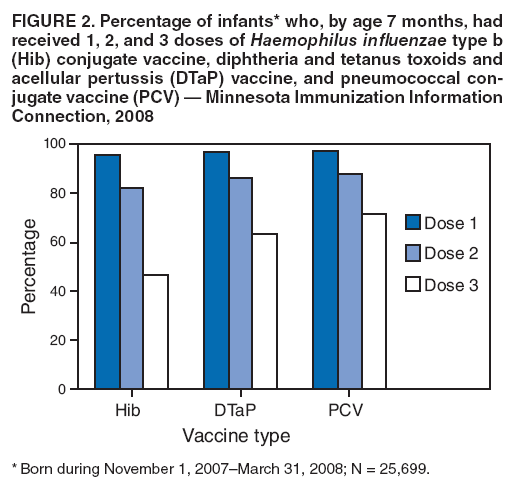
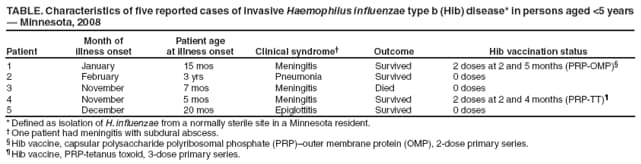
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Invasive Haemophilus influenzae Type B Disease in Five Young Children --- Minnesota, 2008On January 23, this report was posted as an MMWR Early Release on the MMWR website (http://www.cdc.gov/mmwr). In 2008, five children aged <5 years were reported to the Minnesota Department of Health (MDH) with invasive Haemophilus influenzae type b (Hib) disease; one died. Only one of the children had completed the primary Hib immunization series; three had received no doses of Hib-containing vaccine (1). The five Hib cases are the largest number among children aged <5 years reported from Minnesota since 1992. The cases occurred during a Hib vaccine recall and continuing nationwide shortage that began in December 2007. The recall of certain lots of the two Hib-containing vaccines manufactured by Merck & Co., Inc. (West Point, Pennsylvania) and cessation of production of both vaccines left only one manufacturer of Hib vaccine in the United States (Sanofi Pasteur, Swiftwater, Pennsylvania) (2,3). In response, CDC recommended that health-care providers defer the routine 12--15 month booster dose for children not at increased risk for Hib disease (2,3). CDC also emphasized that all children should complete the primary series with available Hib-containing vaccines. However, Minnesota vaccination data indicate that primary Hib series coverage was lower during 2008 than coverage with other vaccines administered at the same ages and lower than Hib coverage in previous years. Increases in Hib cases like the one in Minnesota do not appear to have occurred in other states. The increase highlights the need to ensure that all children complete the primary Hib immunization series. Additional investigation to better elucidate the factors that led to these cases is being conducted by MDH and CDC. Minnesota conducts surveillance for invasive H. influenzae disease as part of the Active Bacterial Core surveillance system of CDC's Emerging Infections Program (4). A Hib case is defined as isolation of H. influenzae from a normally sterile site in a resident of the state. Merck products are both Hib PRP-OMP* vaccines, for which a primary series consists of 2 doses at 2 and 4 months. Sanofi Pasteur products are Hib PRP-TT† vaccines, for which a primary series consists of a 3-dose primary series at 2, 4, and 6 months. For both Hib vaccine series, a routine booster is recommended at age 12--15 months During 2008 in Minnesota, five children aged 5 months to 3 years were reported with invasive Hib disease; one died (Table). The patients resided in five different counties in Minnesota and had no known relationship to each other. Three patients had received no vaccinations because of parent or guardian deferral or refusal. One child was aged 5 months and had received 2 doses of Hib PRP-TT vaccine in accordance with the primary series schedule. Another child had received 2 doses of Hib PRP-OMP vaccine, but no booster dose, per CDC recommendations during the shortage. Subsequent to Hib infection, this child was diagnosed with hypogammaglobulinemia. None of the five were enrolled in group child care. The five cases in 2008 were the most reported for 1 year from Minnesota since 1992, when 10 cases were reported (Figure 1). Although the recall and cessation of production of Merck Hib-containing vaccines in December 2007 resulted in a nationwide Hib vaccine shortage, supply of the remaining two products manufactured by Sanofi Pasteur is adequate for all infants to complete the 3-dose primary vaccine series. However, in February 2008 the Minnesota Vaccines for Children program began receiving reports from vaccine providers regarding shortages of vaccine in their offices. In response, MDH advised providers to ensure completion of the primary series as recommended whenever possible and to track and recall infants who had not completed the primary series so that they could be vaccinated as soon as doses were available. On January 13, MDH examined 2008 vaccination coverage data in the Minnesota Immunization Information Connection (MIIC), Minnesota's immunization registry. Data were reviewed for 25,699 children born between November 1, 2007 and March 31, 2008 (Figure 2). Among children aged 7 months, 3-dose primary Hib series coverage was 46.5%, which is lower than the age-appropriate coverage for children who had received pneumococcal conjugate or diphtheria and tetanus toxoids and acellular pertussis (DTaP) vaccination. In contrast, data from the 2007 National Immunization Survey, conducted prior to the shortage, showed that Hib vaccination coverage among children in Minnesota aged 19 months to 35 months was high and did not differ from the national average, suggesting that coverage has declined as a result of the shortage. Reported by: J Rainbow, MPH, R Danila, PhD, L Bahta, K White, MPH, K Ehresmann, MPH, R Lynfield, MD, Minnesota Dept of Health. F Coronado, MD, A Cohn, MD, T Clark, MD, N Messonnier, MD, Div of Bacterial Diseases, J Santoli, MD, L Rodewald, MD, Immunization Svcs Div, National Center for Immunization and Respiratory Diseases; M Jackson, PhD, S Lowther, PhD, EIS officers, CDC. Editorial Note:Before development of Hib conjugate vaccines, Hib was the most common cause of bacterial meningitis in children aged <5 years. Since implementation of the Hib conjugate vaccine immunization program in the United States in the early 1990s, the incidence of Hib disease has declined from a peak of 41 cases per 100,000 children aged <5 years in 1987 to approximately 0.11 cases per 100,000 in 2007 (3,5). As with other bacterial diseases in which acquisition of carriage is necessary for development of invasive disease, reductions in asymptomatic carriage and transmission are substantial contributors to the reduction in Hib disease achieved through vaccination programs (6--8). This herd immunity provided by high vaccination coverage provides additional protection both for fully vaccinated and undervaccinated persons (6--8). Three of the five Hib cases in Minnesota occurred in children who had not been vaccinated. One case occurred in a child who was too young to complete the primary series, and a fifth case occurred in a child with an immunodeficiency. Given the prolonged booster dose deferral and reduced primary series coverage in the state, the increase in the number of Hib cases likely reflects increasing carriage and transmission affecting those with suboptimal primary series vaccination coverage, or a weakening of herd immunity. None of the children failed to receive vaccine because of the vaccine shortage. However, MDH is planning evaluations to describe the extent of Hib carriage in the affected communities and understand reasons why some children are not vaccinated. While the shortage continues, completion of the primary series in all children is essential to safeguard individual protection as well as to strengthen herd immunity. The current Hib vaccine supply in the United States is sufficient to ensure completion of the primary series for all children, but not yet to resume the booster dose. However, vaccine shortages are difficult to manage. Health-care providers must maintain sufficient stocks on hand for every child brought for vaccination each day. During shortages, local supply/demand mismatches can occur, resulting in missed doses (9,10). Hib vaccine supply problems can be further complicated because the primary series for the recalled products consists of 2 doses, but the primary series for the available products consists of 3 doses. Regardless of brand or product used, full vaccination with the primary series of Hib vaccine by age 7 months is critical to protect children from disease. Providers who have questions regarding Hib vaccine supply needed to complete the primary vaccine series should contact their state health departments. Combination products may be used for any or all doses of the Hib primary series. Further, if combination vaccines are the only vaccines available to providers, a combination product should be used to complete the primary Hib series, even when this results in receipt of additional doses of another antigen. In response to the findings described in this report, MDH is working with vaccination providers and other partners to resolve any local supply problems. As the vaccine supply resolves, MDH will expedite resumption of the booster dose in communities where Hib cases have been reported. Invasive Hib disease in children aged <5 years is a nationally notifiable condition. Health-care providers should promptly report all suspected cases of Hib to their local health department. CDC routinely analyzes national surveillance data for invasive Hib disease in children aged <5 years. As of January 13, 2009, no other increases in Hib cases in children aged <5 years had been reported from other states or territories. CDC is working with health departments to identify areas of suboptimal primary Hib series coverage that might lead to increased transmission and disease. Prompt recognition and reporting of Hib cases is important both in understanding the impact of the Hib vaccine shortage and in guiding recommendations for resuming routine booster vaccination and catch-up of undervaccinated children. Acknowledgments This report is based, in part, on contributions by S Jawahir, S Ersted, L Triden, J Harper, MS, K Como-Sabetti, MPH, Minnesota Dept of Health. References
* Capsular polysaccharide polyribosomal phosphate (PRP)--outer membrane protein (OMP). † PRP-tetanus toxoid.
Figure 1
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 1/28/2009 |
|||||||||
|