|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
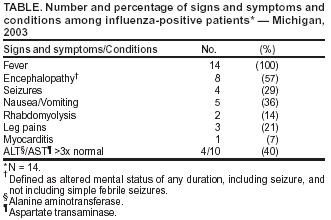
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Severe Morbidity and Mortality Associated with Influenza in Children and Young Adults --- Michigan, 2003During late January 2003, the Michigan Department of Community Health (MDCH) received reports of severe unexplained illnesses and deaths in children and young adults aged <21 years residing in Michigan. Subsequently, two of the deaths were found to be associated with influenza, including one with neurologic complications. To identify cases of severe influenza in otherwise healthy children and young adults aged <21 years, MDCH conducted enhanced surveillance for influenza-associated illness. This report summarizes the findings of this ongoing investigation, which indicate the need to better define the frequency of serious complications from influenza in healthy children and to incorporate such findings into evaluations of current vaccine recommendations for children. Enhanced surveillance for influenza-associated severe illnesses and deaths focused on children and young adults aged <21 years at low risk* for influenza complications who had illness onset or death after January 1, 2003. Severe influenza-associated illnesses included nonrespiratory complications requiring hospital admission (e.g., myocarditis, rhabdomyolysis, encephalitis, encephalopathy, and prolonged seizures) or any complications requiring intensive care unit (ICU) admission. Influenza infections were confirmed by viral culture, rapid antigen test, immunofluorescence, or immunohistochemical staining (IHC). Surveillance for unexplained deaths also was conducted because of the possibility that such deaths were associated with influenza infection. An unexplained death was defined as a fatal, community-acquired illness in a person aged <21 years with evidence of an infectious process† but for which no specific etiology had been identified. MDCH performed case finding by contacting local health departments, infection-control practitioners, health-care providers, and clinical laboratory directors through the Michigan Health Alert Network, broadcast fax, and e-mail listservs. Medical charts and medical examiner reports were reviewed, health-care providers were interviewed, and clinicians were asked to perform influenza testing on children who were experiencing severe complications from influenza-like illness (ILI). In addition, one Michigan county initiated active emergency department (ED) surveillance in two large tertiary care hospitals by laboratory testing all patients with ILI and evaluating all hospitalized children testing positive for influenza to determine if they had illness consistent with the case definition for influenza-associated severe illness. Available respiratory specimens were obtained and cultured for influenza and other respiratory viruses at local clinical and MDCH laboratories. CDC characterized influenza isolates and evaluated available autopsy specimens by using IHC. Enhanced surveillance identified 14 influenza cases, comprising four deaths and 10 severe illnesses with onset during January 17--February 21 among children and young adults aged <21 years in Michigan. Of these 14 cases, eight (57%) had evidence of encephalopathy§, including two deaths, and one case had evidence of myocarditis. In addition, four other unexplained deaths are under investigation. This report describes the four influenza-associated deaths and the 10 severe influenza illnesses. Influenza-Associated Fatality ReportsCase 1. In January, a previously healthy male teenager had onset of fever, nasal congestion, cough, nausea, vomiting, and leg pain. He took over-the-counter (OTC) medications containing pseudoephedrine and acetaminophen that evening and the following morning. On that morning, he was found unresponsive and was transported to an ED, where he could not be resuscitated. ED laboratory tests showed a markedly elevated white blood cell count (WBC) of 34, 000 cells/mm3, (normal range: 4,000--10,500 cells/mm3) with a neutrophilic predominance, a substantially elevated troponin of 98.5 ng/ml (normal range: 0--0.39 ng/ml), and a negative toxicology screen. Evaluation of autopsy specimens indicated interstitial pneumonia and focal myocyte necrosis without frank myocarditis. IHC of respiratory epithelial cells of bronchi from centrally located lung tissue was positive for influenza A virus. Review of available records revealed no history of influenza vaccination. Case 2. In January, a previously healthy girl aged 6 years with a 1-day history of fever, sore throat, and cough was examined by her primary-care physician and noted to have harsh upper airway sounds. A rapid test of a throat swab for Group A Streptococcus was negative. The patient received oral prednisone for the treatment of croup and an OTC cold medicine containing acetaminophen without salicylates. Later the same day, she complained of leg pain. The next morning, she was found apneic. When paramedics arrived, the patient was in cardiopulmonary arrest and was intubated, resuscitated, and transported to an ED. Her WBC count was 15,900 cells/mm3. She was transferred to the pediatric ICU, where she died the same day. A viral culture of an endotracheal aspirate was positive for influenza A virus that was antigenically similar to the vaccine strain A/New Caledonia/20/99 (H1N1)-like. A bacterial culture of a throat swab taken at her primary-care physician's office was positive for Group A Streptococcus. Evaluation of autopsy specimens indicated bronchopneumonia with numerous intracellular bacteria in the intra-alveolar infiltrate. IHC of bronchiolar epithelial cells from lung tissue was positive for influenza A virus but negative for Group A Streptococcus. Review of available records revealed no history of influenza vaccination. Case 3. In February, a girl aged 5 years with no underlying health conditions had onset of a low-grade fever. During the evening, she became disoriented and lethargic and vomited at least seven times. She had recently completed a course of amoxicillin for treatment of streptococcal pharyngitis. The patient received medications containing ibuprofen; no information about aspirin exposure was available. On arrival to an ED the next day, she had a temperature of 104.1º F (40.05º C) and a WBC count of 13,100 cells/mm3 and again vomited. Antibiotics were administered. A nasopharyngeal swab was positive for influenza A virus by a rapid antigen test, and treatment with oseltamivir was initiated. Liver function tests showed an elevated aspartate transaminase of 494 U/L (normal range: 20--45 U/L) and elevated alanine aminotransferase of 383 U/L ( normal range: 5--25 U/L). The patient's neurologic status deteriorated rapidly, and she progressed to respiratory arrest. After intubation, a computerized tomography scan indicated uncal herniation. The patient died 19 hours after admission. Autopsy was declined. A viral culture of the nasopharyngeal specimen obtained during the hospitalization was positive for influenza A virus that was antigenically similar to the vaccine strain influenza A/ New Caledonia/20/99 (H1N1)-like. The patient's illness was consistent with influenza-associated encephalopathy; however, Reye syndrome could not categorically be ruled out because no autopsy was performed. Review of available records revealed no history of influenza vaccination. Case 4. In February, a boy aged 2 years with a history of resolved reactive airway disease had onset of a fever and cough. The next evening and on the third morning, the patient received a children's formulation of an OTC combination cold medication. After several hours of lethargy, the boy was found unresponsive at home. Paramedics transported the child to the hospital, where attempts to resuscitate were unsuccessful. A postmortem lung swab was positive for influenza A virus by a rapid antigen test, but viral culture was negative. Evaluation of autopsy specimens indicated tracheobronchitis and massive brain edema without evidence of inflammation. IHC of respiratory epithelial cells of trachea and bronchi from centrally located lung tissue was positive for influenza A virus. The patient had not been vaccinated against influenza. Severe Nonfatal Influenza IllnessSurveillance identified 10 children with severe illnesses that were likely complications of influenza (Table). The median age of these children was 2.5 years (range: 14 months--9 years); eight patients were female. Nine patients were influenza A virus--positive, and one was influenza B virus--positive. Of the nine influenza A virus cases, eight were confirmed by culture and one by rapid antigen test. Three influenza A virus isolates were H1N1, four were H1N2, and one was H3N2. Of those antigenically characterized, the H1N1 virus isolates and H3N2 virus isolates were similar to the 2002--03 influenza vaccine strains A/New Caledonia/20/99 (H1N1) and A/Panama/2007/99 (H3N2). Of the H1N2 isolates, the H1 antigen was similar to that from the A/New Caledonia/20/99 (H1N1) vaccine strain, and the N2 antigen was similar to that from the A/Panama/2007/99 (H3N2) vaccine strain; the vaccine should provide protection against influenza A(H1N2) virus. The influenza B isolate was most similar antigenically to the reference strain B/Brisbane/32/2002, a minor variant of the B/Hong Kong/330/2001 vaccine strain. Vaccination history of these 10 children is unknown. Reported by: MJ Wilkins, DVM, ML Boulton, MD, GA Stoltman, PhD, SA Bidol, MPH, KS Enger, MPH, JJ Lai, MPH, Michigan Dept of Community Health. T Uyeki, MD, S Harper, MD, Div of Viral and Rickettsial Diseases; M Fischer, MD, SP Reagan, MPH, Div of Bacterial and Mycotic Diseases; J Jones, MD, P Terebuh, MD, SD Stonecipher, DVM, EIS officers, CDC. Editorial Note:Nationally, the 2002--03 influenza season was mild; however, this investigation documented severe influenza-associated morbidity and mortality, including encephalopathy, among children and young adults aged <21 years in Michigan (1). In Japan, influenza-associated acute encephalopathy among children is a substantial public health problem; in the winter of 1998--99, for example, a total of 148 cases of encephalitis/encephalopathy associated with influenza were reported (2). Few such cases have been reported in the United States (3,4). The reasons for these differences are unclear. Influenza-associated deaths and severe illnesses in children might be underreported in the United States. Because baseline data on such events are not generally available, whether the cases described in this report represent an increase or are the result of enhanced surveillance is unknown. In addition, because influenza is not a nationally reportable disease, the estimated numbers of annual deaths from influenza are derived from modeling techniques (5). Of the four deaths associated with influenza, none were in children considered to be at high risk for influenza, nor were they in the age group for which influenza vaccination is encouraged by the Advisory Committee on Immunization Practices (ACIP) (6). The risk factors for severe complications and death from influenza in previously healthy children have not been well described. The viruses isolated from these cases were of different types and subtypes and were antigenically similar to viruses in circulation throughout the United States during 2002--03. Vaccination for influenza is recommended for persons at high risk for complications from influenza. Young, otherwise healthy children aged 6--23 months are at increased risk for influenza-related hospitalization. For this reason, influenza vaccination of healthy children aged 6--23 months is encouraged when feasible (6). The results of this ongoing investigation indicate the need for further studies to better define the frequency of serious complications from influenza in children and young adults and to incorporate such findings into evaluations of current vaccine recommendations for children. Acknowledgments This report is based on data contributed by LE Bauman, S Reedy, Washtenaw County Public Health Dept, Ypsilanti; Newaygo County Health Dept, Cadillac; Oakland County Health Dept, Pontiac; MG Stobierski, DVM, T Bolen, MS, J Beggs, MPH, B Carlson, MPH, H Kapoor, MD, PA Somsel, DrPH, P Clark, MPH, VM Vavricka, MS, A Casey, DS Wilkinson, Michigan Dept of Community Health. K Fukuda, MD, S Zaki, MD, WJ Shieh, MD, J Guarner, MD, C Paddock, MD, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; K Kurpel, VMD, Epidemiology Program Office, CDC. References
* Not a member of a high-risk group (i.e., residents of chronic care facilities; persons with chronic disorders of the circulatory or respiratory system, including asthma; persons with chronic metabolic disorders, renal dysfunction, hemoglobinopathies, or immunosuppression; children on aspirin therapy for chronic conditions; and women who are pregnant (1). † Includes any of the following: fever, leukocytosis or leukopenia, histopathologic evidence of acute infection or inflammation, inflammation of usually sterile fluids, or imaging studies consistent with infection or inflammation. § Defined as altered mental status of any duration, including seizure but not including simple febrile seizures.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 9/4/2003 |
|||||||||
This page last reviewed 9/4/2003
|