 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Poliomyelitis Eradication ---Eastern Mediterranean Region, January 2000--September 2001The World Health Assembly resolved to eradicate poliomyelitis in 1988, and the goal of the regional committee for the Eastern Mediterranean Region (EMR)* of the World Health Organization (WHO) was to eradicate polio from that region by 2000. This report summarizes EMR polio eradication activity during January 2000--September 2001; poliovirus transmission has been interrupted in 18 of the 23 EMR countries and has become localized in the remaining five. Despite these achievements, the countries of EMR must overcome many challenges to interrupt virus transmission by the end of 2002. During 2000, 79% of infants received 3 doses of oral poliovirus vaccine (OPV) through routine vaccination. Coverage of <80% was reported from Afghanistan (32%), Djibouti (46%), Pakistan (74%), Somalia (18%, northern regions only), Sudan (65%), and Yemen (76%). These countries represent approximately half the regional population (estimated 2000 population: 488 million)†. During 1999--mid-2001, supplemental vaccination activities were conducted in all EMR countries except Cyprus, Oman, and the United Arab Emirates. Intensified activities were conducted in countries where polio is endemic. Four national immunization days (NIDs)§ and subnational campaigns took place in Egypt, Iraq, and Sudan (including warring sections of southern Sudan). Afghanistan and Pakistan conducted four rounds of intensified NIDs, and Somalia conducted subnational campaigns and three rounds of NIDs. By the end of 2001, each of the six countries (Afghanistan, Egypt, Iraq, Pakistan, Somalia, and Sudan) will have conducted four to five NID rounds, subnational, or mopping-up (i.e., focal mass campaigns in high-risk areas) campaigns. Some polio-free countries have reduced the scope of activities from national to subnational, targeting low vaccination coverage provinces or areas at high risk for poliovirus importation. Coordination and synchronization of NIDs within EMR countries and among its neighbors have been highly successful. All EMR countries have established acute flaccid paralysis (AFP) surveillance and have implemented surveillance in countries affected by war and in areas with rudimentary or nearly nonexistent health-care services (e.g., Afghanistan, Somalia, and southern Sudan). During 2000, a total of 16 countries (Afghanistan, Bahrain, Egypt, Iran, Iraq, Jordan, Kuwait, Lebanon, Oman, Pakistan, Saudi Arabia, Somalia, Sudan, Syria, Tunisia, and Yemen) reached or exceeded the WHO-established minimum AFP reporting rate of one nonpolio AFP case per 100,000 children aged <15 years, which indicates a sensitive surveillance system (Table 1); the annualized 2001 regional rate is 1.8 compared with 1.4 in 2000. The second key indicator of the quality of AFP surveillance is a minimum of 80% adequate stool specimens collected for all persons with AFP. In 2000, a total of 11 countries or areas (Bahrain, Egypt, Iraq, Jordan, Kuwait, Lebanon, Libya, Palestine, Saudi Arabia, Syria, and Tunisia) met or exceeded the target rate; in four other countries (Iran, Oman, Pakistan, and Yemen), adequate specimens were collected from 60%--80% of persons with AFP. Regionwide, the percentage of persons with AFP with adequate stool specimens increased from 67% in 1999 to 70% in 2000. During January--September 2001, five additional countries (Iran, Morocco, Oman, Pakistan, and Yemen) reached the target rate, and Afghanistan and Sudan improved markedly, which resulted in a regional rate of 83%. The regional laboratory network consists of eight national and four regional reference laboratories. In 2000, a total of 11 network laboratories were accredited fully by WHO with provisional accreditation for one laboratory. During January--September 2001, a total of 5,503 stool specimens were obtained and tested from 99% of 2,767 AFP cases from 21 countries. The specimens from Somalia and southern Sudan were tested in the laboratory of the WHO African region. Laboratory results were reported within 28 days of receipt for >80% of stool specimens tested during 2000 and 2001. The number of confirmed cases of polio reported in EMR countries decreased from 914 in 1999 to 505 in 2000. During January--September 2001, a total of 91 virus-confirmed cases of polio were reported from five countries (Afghanistan, Egypt, Pakistan, Somalia, and Sudan), approximately a third the number reported from seven countries during the same period in 2000. A polio outbreak in Iraq during the second half of 1999 (1) ended following high-quality NIDs and mopping-up activities; the last confirmed cases occurred in January 2000. Since late 1999, wild poliovirus transmission in Egypt has been localized to Upper Egypt. During 2001, continued circulation of several lineages of wild type 1 poliovirus in Egypt was confirmed by virus isolates from both AFP cases and wastewater samples. Through expanded surveillance in south and central Somalia, a polio outbreak was identified in Mogadishu during 2000 (54 confirmed cases during March--June) (2). The outbreak has been controlled with sporadic cases in or near Mogadishu. Unique transmission chains of poliovirus types 1 and 3 have been identified in Sudan and Somalia. Low-level transmission of wild virus continued in Sudan with a 9-month gap between the last two confirmed cases, one from the north in July 2000 and the last from the south in April 2001. Recent genetic data indicate the continued existence of virus reservoirs shared between Pakistan and Afghanistan. Pakistan reported the largest number of cases in 2000, although the number of confirmed cases (199) declined approximately 40% compared with 1999 (324). During January--September 2001, the number of confirmed cases declined 43% (74 versus 130) compared with the same period in 2000. Most districts appear polio-free, with the most intense transmission localized to a few districts in each province. In Afghanistan, the number of virus isolates and affected districts have been reduced substantially. Nine confirmed cases have been reported from Afghanistan during January 2000--September 2001 compared with 21 during the preceding study period. All cases from 2001 have come from districts in three adjacent provinces in the southern region. WHO is supporting countries to develop and implement national plans for the laboratory containment of poliovirus (3). As of September 2001, a total of 18 of the 23 countries of the region have prepared national containment plans. The first phase of the plan is being implemented in Jordan, Kuwait, Lebanon, Libya, Syria, Tunisia, and United Arab Emirates. Oman, Qatar, Bahrain, Cyprus, Morocco, and Saudi Arabia have completed the first phase of the plan and have submitted a national inventory of laboratories storing poliovirus infectious or potentially infectious materials; 11 of the 12 WHO-designated poliovirus network laboratories in the region have provided inventories of stored materials. Reported by: Regional Office for the Eastern Mediterranean Region, Cairo, Egypt. Dept of Vaccines and Biologicals, World Health Organization, Geneva, Switzerland. Respiratory and Enteric Viruses Br, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Global Immunization Div, National Immunization Program, CDC. Editorial Note:EMR countries have made rapid and substantial progress toward polio eradication during 2000. The intensity and geographic extent of virus transmission continued to decrease, and if eradication activities continue, EMR should move closer to stopping wild poliovirus transmission. Four of the 10 global priority countries for polio eradication are in EMR: Pakistan, considered one of the global virus reservoirs; and Afghanistan, Somalia, and Sudan, countries affected by conflict. Armed conflict, high population density, poor sanitation, low OPV coverage, and weak or absent health infrastructures have posed obstacles to interrupting virus transmission. Increasing the number of supplementary campaigns and improving their quality have intensified eradication activities in countries where polio is endemic. Measures to improve supplementary vaccination activities and increase coverage, especially among hard-to-reach and high-risk populations, included advanced preparation, better local planning, extensive supervision, community mobilization, heightened political commitment, and the use of house-to-house vaccination. Surveillance in most countries now reliably identifies or excludes ongoing virus transmission, allowing monitoring of progress and targeting of vaccination activities. The accelerated efforts have required additional technical, financial, and administrative support¶. With WHO support, approximately 100 international experts and 600 national staff have been placed at national and subnational levels in all priority countries. Despite these advances, the eradication program faces a number of challenges such as 1) improving the quality of supplementary vaccination, surveillance, certification, and containment activities; 2) securing access to all children, particularly in areas affected by war and conflict; 3) strengthening the political commitment to reach the eradication goal in polio-free countries and in countries where polio is endemic and; 4) providing the necessary financial resources from all partner agencies and bilateral donors. Meeting these challenges should enable countries of the EMR to interrupt poliovirus transmission by the end of 2002. References
* Djibouti, Egypt, Libya, Morocco, Somalia, Sudan, and Tunisia in northern and eastern Africa; Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, United Arab Emirates, and Yemen in the Arabian peninsula; Cyrus, Iraq, Jordan, Lebanon, Syria, and the Palestinian National Authority in the Middle East; Afghanistan and Iran. † U.S. Bureau of the Census. § Mass campaigns over a short period (days) in which 2 doses of OPV are administered to all children in the target age group (usually aged <5 years) regardless of vaccination history with an interval of 4--6 weeks between doses. ¶ Support of polio eradication activities in EMR is provided mainly by governments of member states and by Rotary International, CDC, the government of the United Kingdom through the Department of Foreign and International Development, the government of Japan through the Japanese International Cooperative Agency, the government of Canada through the Canadian International Development Agency, the government of Denmark through Danish International Development Assistance, Sultanate of Oman, the governments of Norway and Italy, the United Nations Foundation, and the U.S. Agency for International Development. Table 1 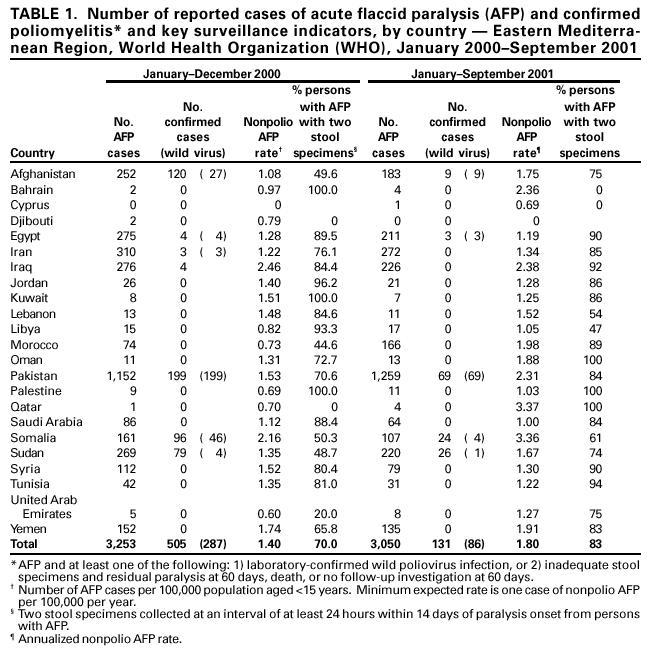 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 12/13/2001 |
|||||||||
This page last reviewed 12/13/2001
|