Key points
- Ringworm is caused by fungi (not a worm).
- It is a common fungal infection of scalp, skin, or nails.
- Athlete's foot, jock itch, and most fungal nail infections are forms of ringworm.
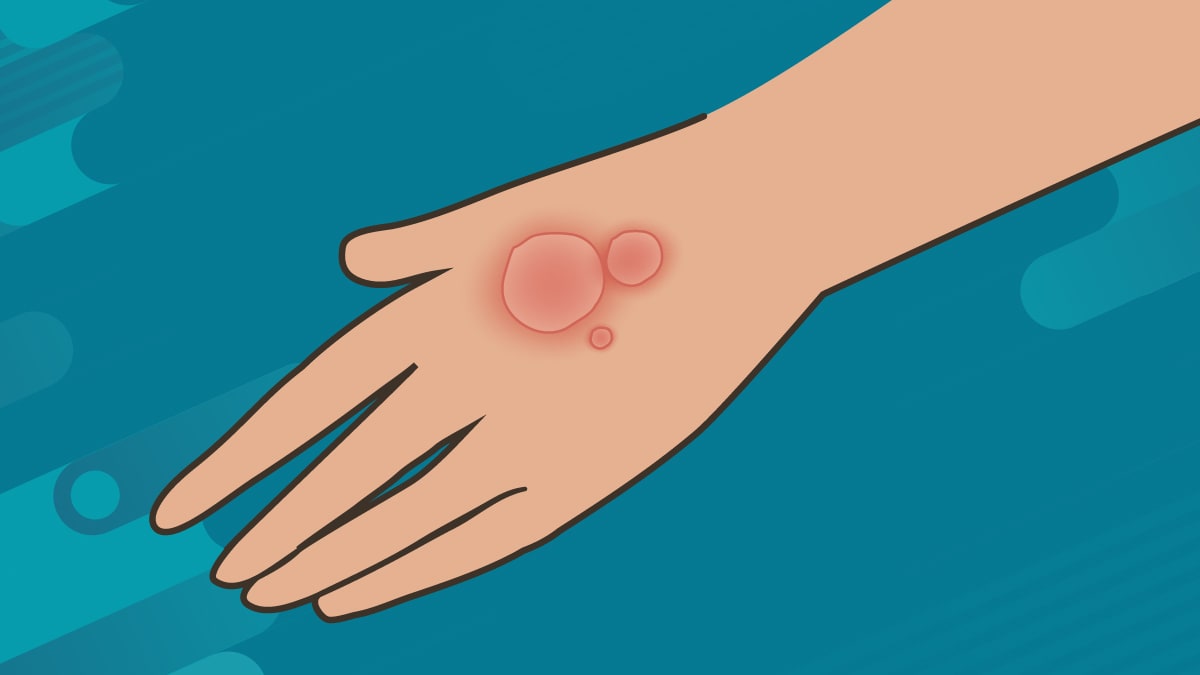
- On the skin, it causes an itchy, scaly, often ring-shaped rash.
- Nail infections may cause nails to change colors, become thick, and break easily.
What it is
Ringworm is a common fungal infection of the scalp, skin, or nails (onychomycosis). It gets its name because it causes a ring-shaped, itchy rash. It typically looks red on light skin and appears gray or brown on darker skin.
Skin and scalp infections
Skin infections are more common on certain parts of the body like on the foot or groin. Ringworm on feet (tinea pedis) is often referred to as athlete's foot. Ringworm on the groin (tinea cruris) is often called jock itch. Tinea of the scalp, tinea capitis, is also common. The medical term for each type of ringworm starts with 'tinea' followed by the Latin name for the part of the body infected.
Nail infections
Ringworm is also a common type of fungal nail infection (onychomycosis). It can cause nails to change colors, become thick, and break easily. Although infections are much more common in toenails, fingernails can get infected.
Causes
Ringworm is caused by fungi (not a worm). The scientific names for the most common fungi that cause ringworm are Trichophyton, Microsporum, and Epidermophyton.
Ringworm is very common and can be spread by:
- Skin-to-skin contact with people or animals with the infection.
- Shared objects like towels and bedsheets.
- Shared surfaces like locker room or public bathroom floors.
Recently, there have been reports of ringworm linked to sexual contact.
Risk factors include:
- Use of public showers or locker rooms without protective footwear.
- Participating in contact sports like wrestling.
- Wearing tight shoes and socks.
- Excessive sweating.
- Close contact with infected animals.
Anyone can get ringworm, but people who have weakened immune systems may be especially at risk for infection. They may also have problems fighting off a ringworm infection. Learn more about how to prevent ringworm.
Prevention
Ringworm spreads easily but there are simple ways to help prevent ringworm:
- Keep skin clean and dry
- Wear protective footwear in areas like public showers or locker rooms.
- Wash your hands after touching pets.
- Do not share sports gear or other personal items (like towels or socks).
- Change socks and underwear every day.
- Keep fingernails short and clean.
It is also important to avoid skin-to-skin contact, including intimate or sexual contact, with anyone with known or suspected ringworm.

Testing
If you have a rash, nail infection, or symptoms of ringworm, go to a healthcare provider for testing. You may go to your primary care provider, dermatologist, or podiatrist. Symptoms of ringworm are similar to symptoms for other skin or nail conditions. Testing can help make sure you get the right treatment.
Healthcare providers may take a small skin scraping or nail sample for testing.
Treatment
The treatment for ringworm depends on its location on the body and how serious the infection is. Some forms of ringworm can be treated with non-prescription (over-the-counter) antifungal medications. However, other forms of ringworm need treatment with prescription antifungal medication.