Key points
- The type of specimen collected when testing for current or past infection with SARS-CoV-2 is based on the test being performed and its manufacturer's instructions. Some of the specimen types listed below will not be appropriate for all tests.
- Check with the testing laboratory’s test directory to ensure they can accept a specimen before collection.
- For diagnostic testing for current SARS-CoV-2 infections, CDC recommends collecting and testing an upper respiratory specimen.
- This guidance is intended for healthcare providers or health department staff who are collecting specimens from others in a healthcare setting or at the point-of-care.
Collecting and Handling Specimens Safely
For healthcare providers collecting specimens or working within 6 feet of patients suspected to be infected with SARS-CoV-2, maintain proper infection control and use recommended personal protective equipment (PPE), which includes an N95 or higher- level respirator (or face mask if a respirator is not available), eye protection, gloves, and a gown.
Sensitivity and specificity differ among different tests and different specimens. Decisions on which tests to use and which specimens to collect are at the discretion of health departments and healthcare providers.
For healthcare providers who are handling specimens but are not directly involved in collection (e.g. handling self-collected specimens) and not working within 6 feet of the patient, follow Isolation Precautions. Healthcare providers should wear a form of source control (face mask) at all times while in the healthcare facility.
Healthcare providers can minimize PPE use if patients collect their own specimens while maintaining at least 6 feet of separation. For example, the provider should wear a face mask, gloves, and a gown.
Respiratory Specimen Collection
Respiratory specimens should be collected as soon as a decision has been made to test someone, regardless of the time of symptom onset. The guidance below addresses options for collecting specimens.
Proper specimen collection is the most important step in the laboratory diagnosis of infectious diseases. A specimen that is not collected correctly may be rejected for testing or lead to false or inconclusive test results. The following specimen collection guidelines follow standard recommended procedures.
For diagnostic testing for current SARS-CoV-2 infections, CDC recommends collecting and testing an upper respiratory specimen. Contact the testing laboratory to confirm accepted specimen types and follow the manufacturer instructions for specimen collection. Sterile swabs should be used for the collection of upper respiratory specimens. This is important both to ensure patient safety and preserve specimen integrity. Note that nasopharyngeal and oropharyngeal specimens are not appropriate for self-collection.
Testing lower respiratory tract specimens is also an option. For patients who develop a productive cough, sputum can be collected and tested for SARS-CoV-2 when available. However, the induction of sputum is not recommended due to the possibility of aerosol production during the procedure. Under certain clinical circumstances (e.g., for those receiving invasive mechanical ventilation), a lower respiratory tract aspirate or bronchoalveolar lavage specimen can be collected and tested as a lower respiratory tract specimen.
A. Upper respiratory tract
Nasopharyngeal specimen (NP) collection / oropharyngeal (OP) (throat) specimen collection (performed by a trained healthcare provider only)
Use only synthetic fiber swabs with thin plastic or wire shafts that have been designed for sampling the nasopharyngeal mucosa. Do not use calcium alginate swabs or swabs with wooden shafts, as they may contain substances that inactivate some viruses and may inhibit molecular tests. CDC recommends collecting only the NP specimen, although an OP specimen is an acceptable specimen type. If both NP and OP specimens are collected, combine them in a single tube to maximize test sensitivity and limit use of testing resources.
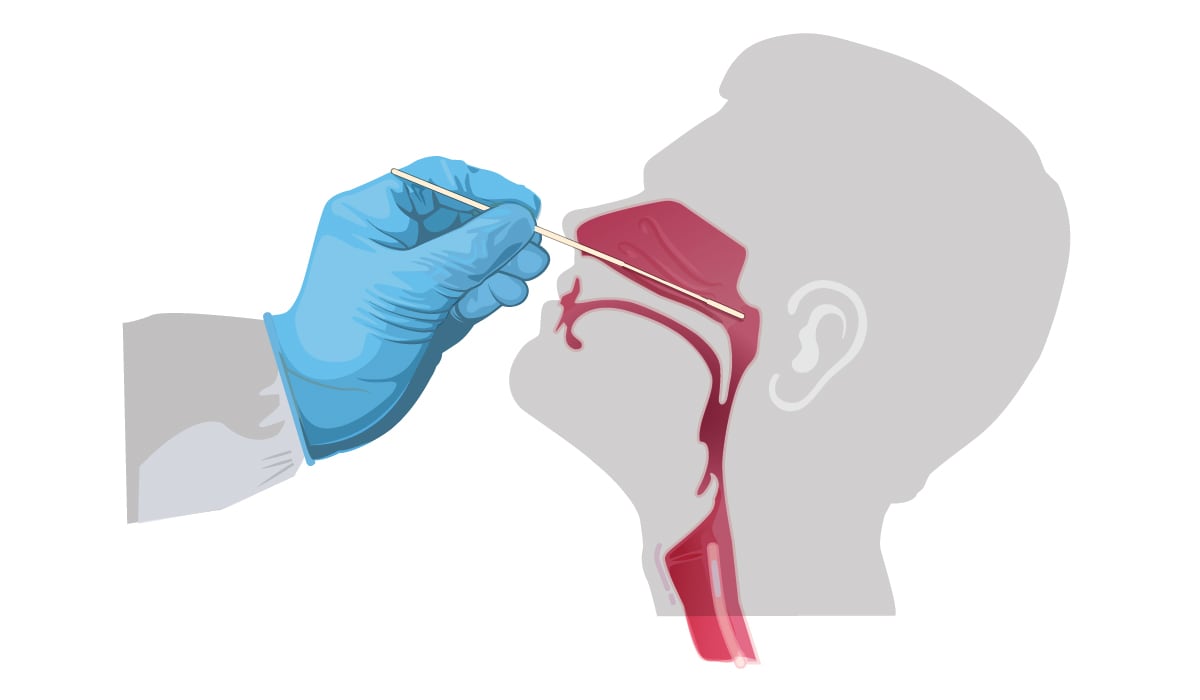
Instructions for collecting an NP specimen (performed by a trained healthcare provider):
- Tilt patient’s head back 70 degrees.
- Gently and slowly insert a mini-tip swab with a flexible shaft (wire or plastic) through the nostril parallel to the palate (not upwards) until resistance is encountered or the distance is equivalent to that from the ear to the nostril of the patient, indicating contact with the nasopharynx.
- Gently rub and roll the swab.
- Leave swab in place for several seconds to absorb secretions.
- Slowly remove swab while rotating it. Specimens can be collected from both sides using the same swab, but it is not necessary to collect specimens from both sides if the mini-tip is saturated with fluid from the first collection.
- If a deviated septum or blockage create difficulty in obtaining the specimen from one nostril, use the same swab to obtain the specimen from the other nostril.
- Place swab, tip first, into the transport tube provided.
Instructions for collecting an OP specimen (performed by a trained healthcare provider):
- Insert swab into the posterior pharynx and tonsillar areas.
- Rub swab over both tonsillar pillars and posterior oropharynx and avoid touching the tongue, teeth, and gums.
- Place swab, tip first, into the transport tube provided.
Nasal mid-turbinate (NMT) specimen (performed by a healthcare provider or the patient after reviewing and following collection instructions):
- Use a tapered swab.
- Tilt patient’s head back 70 degrees.
- While gently rotating the swab, insert swab less than 1 inch (about 2 cm) into nostril parallel to the palate (not upwards) until resistance is met at turbinates.
- Rotate the swab several times against nasal wall and repeat in other nostril using the same swab.
- Place swab, tip first, into the transport tube provided.
Visual guides
- For healthcare providers, see the Nasal Mid-Turbinate (NMT) Specimen Collection Steps [16 MB, 2 pages]
- For patients and consumers, see the How to Collect a Nasal Mid-Turbinate Specimen for COVID-19 Testing infographic [4 MB, 2 pages].
Anterior nasal specimen (performed by a healthcare provider or the patient after reviewing and following the collection instructions):
- Insert the entire collection tip of the swab provided (usually ½ to ¾ of an inch, or 1 to 1.5 cm) inside the nostril.
- Firmly sample the nasal wall by rotating the swab in a circular path against the nasal wall at least 4 times.
- Take approximately 15 seconds to collect the specimen. Be sure to collect any nasal drainage that may be present on the swab.
- Repeat in the other nostril using the same swab.
- Place swab, tip first, into the transport tube provided.
Nasopharyngeal wash/aspirate or nasal wash/aspirate (performed by a trained healthcare provider)
- Attach catheter to suction apparatus.
- Tilt patient's head back 70 degrees.
- Instill 1 mL-1.5 mL of non-bacteriostatic saline (pH 7.0) into one nostril.
- Insert the tubing into the nostril parallel to the palate (not upwards). Catheter should reach depth equal to distance from nostrils to outer opening of ear.
- Begin gentle suction/aspiration and remove catheter while rotating it gently.
- Place specimen in a sterile viral transport media tube.
For an additional visual guide, see the Nasopharyngeal/Nasal Aspirate or Nasopharyngeal/Nasal Wash sections in the Influenza Specimen Collection infographic.
For all other specimen types not described above refer to the manufacturer’s instructions. Contact the manufacturer if there are questions on collection.
B. Lower respiratory tract
Bronchoalveolar lavage, tracheal aspirate, pleural fluid, lung biopsy (generally performed by a physician in the hospital setting)
- Collect 2-3 mL into a sterile, leak-proof, screw-cap sputum collection cup or sterile dry container.
- Due to the increased technical skill and equipment needs, collection of specimens other than sputum from the lower respiratory tract may be limited to patients presenting with more severe disease, including people admitted to the hospital and/or fatal cases.
Sputum (collected under the guidance of a trained healthcare professional)
- For patients who develop a productive cough, sputum can be collected and tested when available for SARS-CoV-2. However, the induction of sputum is not recommended. Educate the patient about the difference between sputum (deep cough) and oral secretions (saliva/spit). Have the patient rinse the mouth with water and then expectorate deep cough sputum directly into a sterile, leak-proof, screw-cap collection cup or sterile dry container.
Note: This is an aerosol-generating procedure and likely to generate higher concentrations of infectious respiratory aerosols. Aerosol-generating procedures potentially put healthcare providers and others at an increased risk for pathogen exposure and infection. Healthcare providers should maintain proper infection control, including standard precautions, and wear an N95 or equivalent or higher-level respirator, eye protection, gloves, and a gown, when collecting specimens.
Assessing Validity of Specimens Obtained Through Self-Collection
Self-collection of specimens, both unsupervised and supervised by a medical professional, is currently available for specific tests authorized by the FDA.
Laboratories should confirm the specimen has been obtained correctly and from the individual that is being tested. Generally, Clinical Laboratory Improvement Amendments (CLIA) require laboratories to ensure positive specimen identification and optimum integrity of a patient's specimen using at least two separate (distinct) or unique identifiers, such as patient's name or another unique identifier. Other information that must be provided to the laboratory when requesting a test includes the sex and age or date of birth of the patient; the test(s) to be performed; the specimen source; the date and, if appropriate, the time of specimen collection.
Handling Bulk-Packaged Sterile Swabs Properly for Upper Respiratory Specimen Collection
Sterile swabs for upper respiratory specimen collection may be packaged in one of two ways:
- Individually wrapped (preferred when possible)
- Bulk packaged
When individually wrapped swabs are not available, bulk-packaged swabs may be used for specimen collection; however, care must be exercised to avoid SARS-CoV-2 contamination of any of the swabs in the bulk-packaged container.
- Before engaging with patients and while wearing a clean set of protective gloves, distribute individual swabs from the bulk container into individual sterile disposable plastic bags.
- If bulk-packaged swabs cannot be individually packaged:
- Use only fresh, clean gloves to retrieve a single new swab from the bulk container.
- Close the bulk swab container after each swab removal and leave it closed when not in use to avoid accidental contamination.
- Store opened packages in a closed, airtight container to minimize contamination.
- Keep all used swabs away from the bulk swab container to avoid contamination.
- Use only fresh, clean gloves to retrieve a single new swab from the bulk container.
- As with all swabs, only grasp the swab by the distal end of the swab, using gloved hands only.
- When patients are self-collecting swabs under clinical supervision:
- Hand a swab to the patient only while wearing a clean set of protective gloves.
- The patient can then self-swab and place the swab in transport media or sterile transport device and seal.
- If the patient needs assistance, you can help the patient place the swab into transport media or a transport device and seal it.
- Hand a swab to the patient only while wearing a clean set of protective gloves.
Storing and Shipping Respiratory Specimens
Shipping Specimens to CDC
If necessary, and with advance approval, specimens may be shipped to CDC if repeated testing results remain inconclusive or if other unusual results are obtained. Please contact CDC at respvirus@cdc.gov prior to submitting specimens to confirm.
Additional information, including the specimen submission form and shipping address, can be found at Submitting Specimens to CDC.
Pneumatic Tube Transport
CDC recommends that each laboratory perform a risk assessment before using the pneumatic tube system to transport suspected or confirmed SARS-CoV-2 specimens. Each facility should conduct a site- and activity-specific risk assessment of the procedures performed, identifying the hazards involved in the process, the competency level of the personnel performing the methods, and the laboratory facility. An institution's biosafety professional, laboratory management, scientific/clinical, and safety staff should be involved in conducting the risk assessment process to determine the appropriate specimen transport practices to implement at the facility.
Facilities should ensure that all personnel who transport specimens via pneumatic tubes are trained in safe handling practices, specimen management, and spill decontamination procedures.
For additional information about performing a risk assessment, refer to the Biological Risk Assessment: General Considerations for Laboratories and the Biosafety in Microbiological and Biomedical Laboratories (BMBL) 6th Edition.
Additional Resources
- How to Report COVID-19 Laboratory Data
- Guidance for SARS-CoV-2 Point-of-Care Testing
- Guidance – Proposed Use of Point-of-Care (POC) Testing Platforms for SARS-CoV-2 (COVID-19)
- Information for Clinicians on Influenza Virus Testing
- Information on Collection of Respiratory Specimens for Influenza Virus Testing
- FAQs on Testing for SARS-CoV-2