About
Summary
When first approved, the Advisory Committee on Immunization Practices (ACIP) recommended the hepatitis B vaccine for persons aged ≥19 years at risk, or seeking protection from, hepatitis B virus infection.1 Starting in 1991, all persons aged <19 years were recommended to receive hepatitis B vaccines, including routine recommendations for infants.1 In 2022, the ACIP expanded the recommendation for universal hepatitis B vaccination of infants and children to include all persons aged 19–59 years.2 Removing the risk factor assessment previously specified to determine vaccination eligibility among adults could increase vaccination uptake and prevent new hepatitis B cases.1
Hepatitis B vaccination coverage among persons in the U.S. aged ≥32 years as of 2023, who were born before the universal childhood vaccination recommendations issued in 1991, was assessed using the 2016, 2018, 2021, and 2023 National Health Interview Survey (NHIS) data.3 Knowledge of hepatitis B vaccination eligibility and self-reported receipt of provider recommendation was assessed in 2023 among a subset of persons aged 32–59 years with an in-depth survey using the NORC at the University of Chicago AmeriSpeak® probability-based household panel.
Based on NHIS data, hepatitis B vaccination coverage among adults born before 1991 was 32.5% in 2023, a 2.1 percentage point increase from 2021 but lower than coverage in 2018 (33.8%). In summary, there has been no change in coverage since 2018 among the cohort newly covered by the universal vaccination recommendation, persons aged 19–59 years without known risk factors for hepatitis B.
Analysis of AmeriSpeak® data show that fewer than half (43.1%) of persons aged 32–59 years believed they were eligible to receive hepatitis B vaccine, and even fewer (30.0%) reported ever receiving a provider recommendation for hepatitis B vaccination.
Despite the expansion of the recommendation for hepatitis B vaccination, coverage remains low, and most eligible adults are unaware of the need for vaccination. Increased provider recommendations for vaccination and improvement in adult hepatitis B vaccination uptake could reduce the burden of hepatitis B nationally.
Methods
Hepatitis B vaccination data were collected through the NHIS, a continuous, cross-sectional national household survey of the noninstitutionalized U.S. civilian population conducted by the U.S. Census Bureau for CDC's National Center for Health Statistics.3 The objectives of the NHIS are to monitor the health of the U.S. population and provide estimates of health indicators, health care use and access, and health-related behaviors.4 The NHIS data includes non-institutionalized persons aged ≥19 years with interviews conducted during January 2023–December 2023. Data from survey years 2016, 2018, and 2021 were included in addition to 2023 data to assess trends. Data on hepatitis B vaccine uptake are not collected every year because the NHIS survey questions are rotated every 2-3 years. Questions about receipt of vaccinations recommended for adults are asked of one randomly selected adult within each family in the household. For hepatitis B vaccination, respondents were asked if they had ever received the hepatitis B vaccine. Data were restricted to adults born before the universal hepatitis B vaccination recommendation for infants in 1991; persons aged ≥32 years in 2023. The final sample adult core response rate was 47.0% for the 2023 NHIS, and the analytic sample for hepatitis B vaccination was 22,282 persons aged ≥32 years.
Data related to knowledge of eligibility for hepatitis B vaccination and receipt of a provider recommendation for vaccination were not collected through the NHIS but were obtained in a separate survey of persons aged ≥18 years used to assess knowledge, attitudes, behaviors, and beliefs related to COVID-19, influenza, and other routine adult vaccines. This survey was conducted on behalf of CDC by NORC at the University of Chicago using AmeriSpeak®, a probability-based panel that uses address-based sampling methodology and is designed to be representative of the US household population. Panel members can participate online or by telephone interview. The survey was fielded August 11–25, 2023. After excluding ineligible respondents and incomplete responses, there were 3,038 total respondents in the analysis dataset (weighted cumulative response rateA = 3.9%). All respondents aged ≥18 years were asked "Which of the following vaccines do you believe are recommended for someone your age with your health history?" and "Has a health care provider ever recommended that you get the following vaccines?" with "hepatitis B" included in a list of vaccines each respondent would be eligible for based on age and health conditions. Respondents aged 32–59 years (n=1,468) were included in the analysis.
Weighted data were used to produce national estimates. For hepatitis B adult vaccination coverage estimates, the weighted proportion of respondents who reported receiving hepatitis B vaccination was calculated.
Point estimates and 95% confidence intervals (CIs) were calculated using SUDAAN software (Research Triangle Institute, Research Triangle Park, NC, version 11.0.1) to account for the complex sample design for NHIS data and R version 4.4.0 for AmeriSpeak® data. Differences were measured as the simple difference between 2016 and 2018, 2018 and 2021, and 2021 and 2023 for hepatitis B vaccination coverage. T-tests were used for comparisons between data years and for comparisons of each level of each respondent characteristic to a chosen referent level (e.g., for race and ethnicity, White was the reference group). Statistical significance was defined as P < .05. Estimates from NHIS and AmeriSpeak® data with small sample size (n<30) are suppressed; for NHIS, estimates with large relative standard errors (standard error/estimate >0.3) are also suppressed.
Results
- Hepatitis B vaccination coverage in 2023 was 32.5% among all persons aged ≥32 years.
- Overall, and in each age group, vaccination coverage was higher among adults with risk factorsB for hepatitis B than among those without.
- Coverage by specific risk factors is shown in Table 1.
- Among all persons aged ≥32 years and persons 32–59 years, coverage increased during 2021–2023 among those with risk factors (by 2.9 and 2.7 percentage points, respectively) but not among those without risk factors.
- Among all persons aged ≥32 years, coverage among White adults (32.2%) was higher than Black (29.2%) and Hispanic (28.9%) but lower than Asian (46.3%) and Other (43.8%) adults.
- Among persons aged 32–59 years, White adults had higher coverage (41.3%) compared with Black (33.6%) and Hispanic (31.3%) but lower than Asian (49.4%) adults.
Table 1. Estimated proportion of persons aged ≥32 years (born before 1991) who received hepatitis B vaccination, by age group, increased-risk status, and race and ethnicity — National Health Interview Survey, United States, 2023
| Vaccination, age group, increased-risk status, and race/ethnicity | Sample size | % | 95% CI | Simple difference from 2021 (at least 1 dose, compared with 2023) |
|---|---|---|---|---|
| Hepatitis B vaccination (at least 1 dose), ever§ | ||||
| ≥32 years¶ | ||||
| Total | 22,282 | 32.5 | (31.7-33.3) | 2.1** |
| White | 15,291 | 32.2 | (31.4-33.1) | 1.9** |
| Black | 2,431 | 29.2 | (27.0-31.6)†† | 2.7 |
| Hispanic | 2,928 | 28.9 | (27.0-30.8)†† | 0.4 |
| Asian | 1,148 | 46.3 | (42.5-50.1)†† | 3.9 |
| Other | 484 | 43.8 | (37.8-50.0)†† | 7.1 |
| With risk factors§§ | 9,477 | 41.7 | (40.5-43.0)¶¶ | 2.9** |
|
International travel***
|
8,572 | 41.9 | (40.6-43.3) | 2.6** |
|
History of hepatitis
|
538 | 42.9 | (38.1-47.9) | 9.3** |
|
Living with someone with hepatitis
|
874 | 44.7 | (40.9-48.6) | 2.6 |
| Without risk factors | 12,719 | 25.2 | (24.2-26.1) | 1.0 |
| 32–59 years††† | ||||
| Total | 10,995 | 39.1 | (38.0-40.2) | 2.3** |
| White | 6,610 | 41.3 | (40.0-42.7) | 2.9** |
| Black | 1,303 | 33.6 | (30.5-36.9)†† | 2.5 |
| Hispanic | 2,010 | 31.3 | (29.0-33.6)†† | -0.3 |
| Asian | 772 | 49.4 | (45.1-53.6)†† | 2.3 |
| Other | 300 | 48.4 | (41.3-55.4) | 7.0 |
| With risk factors§§ | 5,390 | 47.3 | (45.7-49.0)¶¶ | 2.7** |
|
International travel
|
5,059 | 47.3 | (45.6-49.0) | 2.4** |
|
History of hepatitis
|
168 | 57.0 | (48.2-65.3) | 15.7** |
|
Living with someone with hepatitis
|
437 | 50.6 | (45.2-56.0) | 3.2 |
| Without risk factors | 5,565 | 31.4 | (30.0-32.8) | 1.2 |
| With diabetes, overall | 821 | 37.5 | (33.8-41.2) | 3.1 |
| ≥60 years | ||||
| Total | 11,287 | 22.9 | (22.0-23.8) | 2.4** |
| With risk factors§§ | 4,087 | 31.4 | (29.8-33.0)¶¶ | 3.3** |
|
International travel
|
3,513 | 31.3 | (29.6-33.0) | 3.0** |
|
History of hepatitis
|
370 | 33.4 | (27.8-39.5) | 5.5 |
|
Living with someone with hepatitis
|
437 | 35.8 | (31.1-40.8) | 1.2 |
| Without risk factors | 7,154 | 17.7 | (16.7-18.8) | 1.8** |
| With diabetes, overall | 2,084 | 25.6 | (23.3-28.0) | 5.9** |
Abbreviations: CI = confidence interval
* For hepatitis B vaccination, data were collected on selected respondent characteristics that increase the risk for infection or progressive chronic liver disease (having diabetes, travel to countries where hepatitis B is endemic, living with someone with hepatitis, and history of hepatitis).
† In this report, persons identified as White, Black, Asian, or Other race are non-Hispanic. Persons identified as Hispanic might be of any race. "Other" includes American Indian/Alaska Native, Native Hawaiian, Pacific Islander, or any other race and persons who identified multiple races. The five racial/ethnic categories are mutually exclusive.
§ Respondents were asked if they had ever received the hepatitis B vaccine.
¶ Born before 1991. Includes persons aged ≥30 years surveyed in 2021 and persons aged ≥32 years surveyed in 2023.
** P < .05 by t-test for comparisons between 2023 and 2021 within each level of each characteristic. Hepatitis B vaccination was not assessed in the 2022 NHIS.
†† P < .05 by t–test for comparisons with White as the reference.
§§ Risk factors for hepatitis B virus infection included international travel, history of hepatitis, and living with someone with hepatitis.
¶¶ P < .05 by t–test for comparisons between adults with and without risk factors.
*** Had traveled outside the United States to countries other than countries in Europe, Japan, Australia, New Zealand, or Canada since 1995.
††† Persons aged 30-59 years in 2021 (born before 1991) and persons aged 32-59 years in 2023.
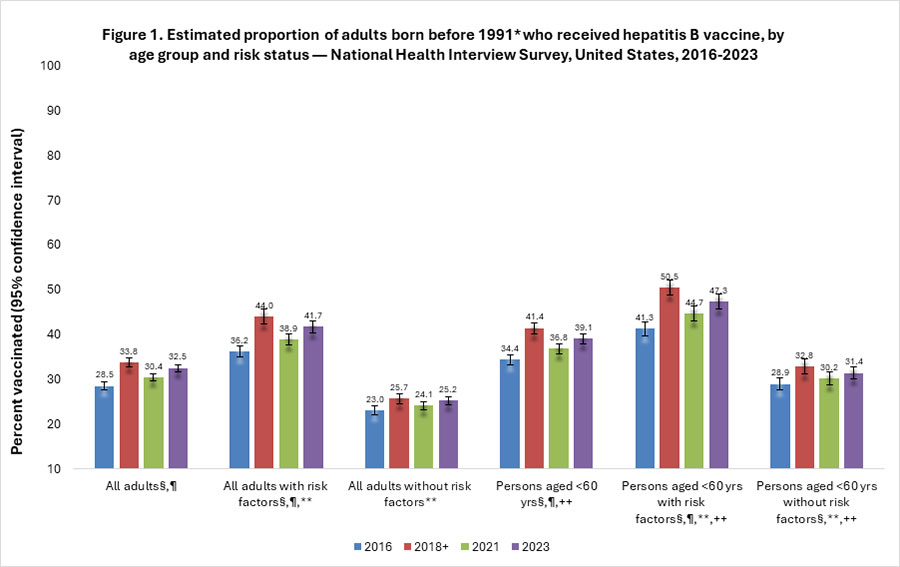
- Estimates of hepatitis B coverage for 2016, 2018, 2021, and 2023 by age group and risk status are shown in Figure 1.
- Coverage increased from 2016 to 2018 among all adults born before 1991 and in each age and risk group.
- In most age and risk groups, coverage decreased between 2018 and 2021 and then increased in 2023, but coverage in 2023 remained below 2018 levels.
- During 2023, the year after recommendation of universal hepatitis B vaccination, coverage did not increase among all persons without risk factors born before 1991, nor persons aged <60 years without risk factors.
Figure 1. Estimated proportion of adults born before 1991 who received hepatitis B vaccine, by age group and risk status — National Health Interview Survey, United States, 2016–2023
- Among persons aged 32–59 years, 43.1% believed hepatitis B vaccination is recommended for someone their age and with their health history.
- The following groups were less likely to report knowledge of eligibility:
- Those living in the South (compared with the West)
- Those who did not report receiving a provider recommendation
- Among persons aged 32–59 years, 30.0% reported a provider had ever recommended hepatitis B vaccination.
- Receipt of a provider recommendation varied by demographic factors.
Table 2. Estimated percentage of persons aged 32–59 years (born before 1991) who believe hepatitis B vaccination is recommended for them and who were recommended a hepatitis B vaccine by a health care provider, by demographic subgroup, Adult Vaccine Hesitancy In-Depth Survey, August 11-24, 2023
| Believe that hepatitis B vaccine is recommended for someone their age and with their health history | Receipt of hepatitis B vaccine recommendation by their health care provider | ||||
|---|---|---|---|---|---|
| Demographic group | Sample size | % | (95% CI) | % | (95% CI) |
| Persons aged 32–59 years | |||||
| Persons 32–59 years | 1,468 | 43.1 | (39.0-47.4) | 30.0 | (26.8-33.5) |
| Chronic health condition | |||||
| With diabetes* | 180 | 36.6 | (27.0-47.4) | 27.0 | (20.1-35.2) |
| With chronic liver disease | 42 | 44.6 | (25.4-65.6) | 42.3 | (25.5-61.1) |
| Race and ethnicity | |||||
| White, non-Hispanic | 872 | 43.8 | (38.4-49.4) | 30.2 | (26.3-34.5)† |
| Black, non-Hispanic* | 177 | 37.9 | (28.0-48.8) | 21.0 | (14.5-29.4) |
| Hispanic | 280 | 42.3 | (33.5-51.6) | 31.6 | (25.2-38.7)† |
| Other, non-Hispanic | 139 | 45.1 | (33.1-57.6) | 35.4 | (25.0-47.4)† |
| Educational status | |||||
| High school diploma or less* | 270 | 40.9 | (33.0-49.4) | 24.9 | (19.1-31.7) |
| Some college, no degree | 567 | 42.5 | (36.4-48.9) | 32.5 | (27.9-37.5) |
| College degree | 358 | 40.9 | (33.9-48.4) | 28.2 | (22.1-35.1) |
| More than college degree | 273 | 49.8 | (42.6-56.9) | 36.3 | (29.8-43.4)† |
| Income | |||||
| Below $25,000 | 219 | 36.3 | (28.6-44.8) | 24.5 | (18.0-32.4)† |
| $25,000-$49,999 | 259 | 44.8 | (34.9-55.2) | 26.3 | (19.4-34.6) |
| $50,000-$74,999 | 283 | 40.5 | (32.1-49.3) | 29.1 | (22.7-36.6) |
| Above $75,000* | 707 | 45.6 | (39.8-51.5) | 33.3 | (29.2-37.7) |
| Urbanicity | |||||
| Rural* | 223 | 42.9 | (33.3-53.1) | 21.1 | (14.1-30.3) |
| Suburban | 655 | 40.3 | (33.2-48.0) | 30.9 | (25.6-36.8) |
| Urban | 590 | 47.1 | (41.0-53.4) | 32.4 | (27.0-38.4)† |
| Region | |||||
| Northeast | 203 | 39.9 | (27.7-53.6) | 32.9 | (22.8-45.0) |
| Midwest | 384 | 48.0 | (38.4-57.7) | 29.5 | (22.2-38.0) |
| South* | 480 | 38.2 | (31.6-45.2) | 27.0 | (21.7-33.0) |
| West | 401 | 48.6 | (42.7-54.6)† | 33.0 | (27.6-38.8) |
| Insurance status | |||||
| Insured* | 1,301 | 43.6 | (39.1-48.2) | 32.2 | (28.8-35.9) |
| Uninsured | 165 | 38.4 | (28.0-50.0) | 12.9 | (7.3-21.8)† |
| Provider recommended vaccine | |||||
| Received vaccine recommendation* | 458 | 65.0 | (57.2-72.1) | ||
| Did not receive vaccine recommendation | 1,007 | 32.6 | (28.4-37.1)† | ||
| Saw provider within last year | |||||
| Saw provider within last year* | 1,025 | 43.3 | (38.3-48.4) | 32.6 | (28.9-36.5) |
| Did not see provider within last year | 441 | 43.1 | (36.1-50.4) | 23.7 | (18.9-29.1)† |
| Has personal provider | |||||
| Has personal provider* | 1,278 | 43.6 | (39.2-48.2) | 32.5 | (28.8-36.4) |
| Does not have personal provider | 186 | 39.2 | (26.1-54.1) | 13.2 | (8.1-20.7)† |
*Reference category.
†Significant difference to reference group (P < .05 by t-test).
Discussion
NHIS data from 2023 indicate that many adults in the United States remain unprotected against hepatitis B.
Prior to 2022, hepatitis B vaccination was a risk-based recommendation. Hepatitis B vaccination coverage decreased between 2018 and 2021, likely due to reduced travel during the COVID-19 pandemic, and possibly due to reduced routine visits to clinics and health care facilities. In 2022, hepatitis B vaccination was universally recommended for persons <60 years of age. Coverage did increase slightly in 2023 after the universal recommendation, but that could be due to resumed travel and health care visits following the pandemic; however, coverage did not increase to pre-pandemic levels. Among all persons aged 19–59 years without risk factors for hepatitis B, the group newly covered by the 2022 universal vaccination recommendation, there was no change in coverage since 2018.
Data in this report suggest most adults are not aware they are eligible for vaccination. Receipt of a provider recommendation was associated with awareness of eligibility for vaccination. However, few adults reported ever receiving a provider recommendation for hepatitis B vaccination, including those who had visited a provider since the universal recommendation was published. The Standards for Adult Immunization Practice recommend that providers assess vaccination status at every patient visit, offer needed vaccines or refer patients to other vaccination sites if vaccines are not available, and use evidence-based interventions such as provider reminder systems and standing orders to improve vaccination coverage.56
Limitations
The estimates in this report are subject to several limitations. First, all data rely on respondent self-report and were not validated with medical records, and therefore may be subject to recall bias. Adults might not be able to recall hepatitis B vaccinations received as children. While this analysis was restricted to adults born before the recommendation for universal infant vaccination with hepatitis B vaccine in 1991, adults born before 1991 could have still been vaccinated as part of catch-up vaccination programs for children. Data from the National Immunization Survey-Teen show that hepatitis B vaccination coverage was 77% among adolescents aged 17 years in 2006, who would be age 34 years in 2023, and 80% for adolescents aged 15 years in 2006, who would be age 32 years in 2023.7 Second, the NHIS response rate was 47.0% in 2023. Nonresponse bias can result if respondents and non-respondents differ in their vaccination status and if survey weighting does not fully correct for this. Third, the NHIS does not collect data on all risk factors for hepatitis B, such as sexual behaviors and injection drug use. Also, while the ACIP recommendations specify that risk factors for hepatitis B include hepatitis C infection and being a household contact of someone with hepatitis B infection, the NHIS questions simply ask about history of hepatitis and living with someone with hepatitis, they do not specify if it is hepatitis B or hepatitis C. Finally, the NHIS and AmeriSpeak® samples exclude persons in the military and those residing in institutions, which might result in underestimation or overestimation of adult vaccination coverage levels.
Authors
Anup Srivastav, B.V.Sc.&A.H., MPVM, PhD1,2; Mei-Chuan Hung, MPH, PhD1,2; Peng-jun Lu, MD, PhD1; Kayla Calhoun, MS1; Susanne Schorpp, PhD1,3; Min Kim, MD4; Carla L. Black, PhD1
1 Immunization Services Division, National Center for Immunization and Respiratory Diseases, CDC
2 Eagle Health Analytics, Inc, Atlanta, GA
3 Goldbelt Professional Services, LLC, Chesapeake, VA
4 Division of Viral Hepatitis, National Center for HIV, Viral Hepatitis, STD, and TB Prevention, CDC
- Weighted Cumulative Response Rate: The overall survey response rate that accounts for survey response in all phases, including panel recruitment, panel retention, and survey completion. This overall rate is weighted to account for the sample design and differential inclusion probabilities of sample members in all sampling stages.
- Risk factors for hepatitis B virus infection included international travel, history of hepatitis, and living with someone with hepatitis.
- Schillie S, Vellozzi C, Reingold A, et al. Prevention of hepatitis B virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep 2018;67:1–31.
- Weng MK, Doshani, M, Khan MA, et al. Universal hepatitis B vaccination in adults aged 19–59 Years: Updated recommendations of the Advisory Committee on Immunization Practices — United States, 2022; MMWR Morb Mortal Wkly Rep 2022;71(13):477–483.
- National Center for Health Statistics. Survey description, National Health Interview Survey, 2022. Hyattsville, Maryland. 2022. Available at: https://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/NHIS/2022/srvydesc-508.pdf
- National Center for Health Statistics. Public-use data file and documentation. Available at: https://www.cdc.gov/nchs/nhis/about/index.html
- CDC. Standards for adult immunization practice. Available at: https://www.cdc.gov/vaccines-adults/hcp/imz-standards/index.html
- Community Preventive Services Task Force. The Guide to Community Preventive Services: what works to promote health? Available at: http://www.thecommunityguide.org/index.html.
- CDC. National vaccination coverage among adolescents aged 13-17 years--United States, 2006. MMWR Morb Mortal Wkly Rep. 2007;56(34):885–888.