Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Global Routine Vaccination Coverage, 2011
In 1974, the World Health Organization (WHO) established the Expanded Programme on Immunization (EPI) to ensure all children had access to routinely recommended vaccines. Initially, those vaccines were limited to bacille Calmette-Guérin vaccine (BCG), diphtheria-tetanus-pertussis vaccine (DTP), oral poliovirus vaccine, and measles-containing vaccine (MCV). Global coverage with the third dose of DTP (DTP3) increased from <5% in 1974 to 79% by 2005. However, one fifth of the world's children, especially those in low-income countries, still were not fully vaccinated during the first year of life with the four traditional EPI vaccines (1). In 2005, WHO and the United Nations Children's Fund (UNICEF) developed the Global Immunization Vision and Strategy (GIVS) to improve national immunization programs and decrease vaccine-preventable disease–associated morbidity and mortality (2). A goal was to reach a sustained national DTP3 coverage of 90% in all countries. This report summarizes global routine vaccination coverage during 2011. An estimated 83% of infants worldwide received at least 3 doses of DTP in 2011, similar to coverage in 2009 (82%) and 2010 (85%). Among 194 WHO member states, 130 (67%) achieved ≥90% national DTP3 coverage. More than half of all incompletely vaccinated children (i.e., those who did not receive DTP3) lived in one of three countries: India (32%), Nigeria (14%), and Indonesia (7%). Strengthening routine immunization services, especially in countries with the greatest number of undervaccinated children, should be a global priority to help achieve the fourth Millennium Development Goal of reducing mortality among children aged <5 years by two thirds from 1990 to 2015.
Vaccination coverage is calculated as the percentage of those in the target age group who received a dose of a recommended vaccine by a given age. DTP3 coverage by age 12 months is a key indicator of immunization program performance, but coverage with other vaccines, such as the third dose of polio vaccine (Polio3) or first dose of measles-containing vaccine (MCV1), also are indicators. Administrative coverage estimates are derived by dividing number of vaccine doses administered to children in the target age group by the estimated target population. These are reported annually to WHO and UNICEF by 194 WHO member states through the Joint Reporting Form (3). More precise estimates of vaccination coverage can be obtained from coverage surveys of a representative sample of households to identify children in the target age group. Dates of receipt of vaccine doses are copied from the child's vaccination card. If the card is not available, a caregiver is asked to recall whether the child received a particular vaccine dose. WHO and UNICEF derive national estimates of vaccination coverage through an annual country-by-country review of all available data, which can lead to revision of past coverage estimates (4). These estimates are updated and published annually on the WHO website (5).
Estimated global DTP3 coverage among children aged <12 months in 2011 was 83%, ranging from 71% in the African Region to 96% in the Western Pacific Region, and representing 106.8 million vaccinated children (Table). Estimated global coverage for BCG, Polio3, and MCV1 was 88%, 84%, and 84%, respectively. During 2011, 130 (67%) countries achieved ≥90% national DTP3 coverage, and 46 (24%) achieved the GIVS goal of ≥80% DTP3 coverage in every district or equivalent administrative unit. DTP3 coverage was 80%–89% in 32 (17%) countries, 70%–79% in 13 (7%) countries, and <70% in 19 (10%) countries.
Among the 22.4 million children who did not receive 3 DTP doses during the first year of life, 11.8 million (53%) lived in three countries, India (32%), Nigeria (14%), and Indonesia (7%), and 16.2 million (72%) lived in 10 countries (Figure). Nearly 14 million (62%) of these children did not receive the first dose of DTP, whereas 8.4 million (38%) started, but did not complete the 3-dose DTP series.
Beyond the traditional four EPI vaccines, several newer vaccines are increasingly utilized by national immunization programs. By the end of 2011, hepatitis B vaccine had been introduced into routine childhood vaccination schedules in 180 (93%) countries; 94 (52%) countries recommended the first dose within 24 hours of birth to prevent perinatal transmission. Worldwide coverage (including countries that have not yet introduced the vaccine) with 3 doses of hepatitis B vaccine was 75% and ranged from 56% in the South-East Asia Region to 91% in the Western Pacific Region (Table). Coverage with 3 doses of Haemophilus influenzae type b vaccine, which had been introduced into 177 (91%) countries by 2011, was 43% globally, ranging from 11% (South-East Asia Region) to 90% (Americas Region). By 2011, rotavirus vaccine had been introduced in 31 (16%) countries, and pneumococcal conjugate vaccine (PCV) in 73 (39%) countries. Coverage with completed rotavirus vaccination series was 9% globally, but reached 66% in the Americas Region. Coverage with 3 doses of PCV was 12% globally and was highest (43%) in the Americas Region.
Reported by
Dept of Immunization, Vaccines, and Biologicals, World Health Organization, Geneva, Switzerland. United Nations Children's Fund, New York, New York. Global Immunization Div, Center for Global Health, CDC. Corresponding contributor: Samir V. Sodha, ssodha@cdc.gov, 404-639-8287.
Editorial Note
In 2011, nearly 107 million infants (83%) worldwide received at least 3 doses of DTP vaccine; however, approximately 22.4 million failed to receive 3 doses, leaving large numbers of children susceptible to vaccine-preventable diseases and death. Two thirds of countries achieved the GIVS target of 90% national DTP3 coverage; however, high national coverage might mask suboptimal coverage at lower administrative levels. Only 24% of countries achieved the GIVS goal of >80% DTP3 coverage in every district.
Administrative coverage estimates are convenient and timely, but might overestimate or underestimate coverage if inaccuracies occur in the numerator (number of doses administered) or denominator (populations based on census data). Although coverage surveys are not dependent on knowing target population size or on other administrative data sources, they are costly, and because they are retrospective, they are not timely. However, coverage surveys are useful for validating administrative data and for monitoring coverage at different administrative levels, to aid in identifying areas of low coverage. WHO recommends that countries conduct regular vaccination coverage surveys to validate reported administrative coverage (6). A WHO advisory committee recommends validation of vaccination coverage estimates, ideally using multiple external data sources such as serosurveys and morbidity and mortality data (6).
Among all incompletely vaccinated children worldwide, 14 million (62%) had not received the first DTP dose. Nearly 8.4 million received at least 1 DTP dose, but dropped out before completing the 3-dose series. Factors associated with undervaccination might be different from those associated with nonvaccination (7). For example, immunization system issues are reported more commonly with undervaccination, whereas access to services, parental attitudes, knowledge, and practices appear to play a greater role among children who have not received any vaccination. For improvements in global vaccination coverage to occur, multifaceted and tailored strategies will be required by countries to address factors contributing to incomplete infant vaccination, particularly in countries with the largest numbers of unvaccinated children.
More than half of incompletely vaccinated children live in three countries (India, Nigeria, and Indonesia). Focusing routine immunization efforts in countries with the highest number of unvaccinated children might substantially reduce the number of susceptible children worldwide and limit the occurrence and spread of vaccine-preventable disease outbreaks. In May 2012, as part of the Decade of Vaccines launched in 2010, a global vaccine action plan was endorsed by all WHO member states at the World Health Assembly (8). Meeting routine vaccination coverage targets in every region, country, and community worldwide is a major goal of this plan.
References
- Keja K, Chan C, Hayden G, Henderson RH. Expanded programme on immunization. World Health Stat Q 1988;41:59–63.
- World Health Organization, United Nations Children's Fund. Global immunization vision and strategy 2006–2015. Geneva, Switzerland: World Health Organization; 2005. Available at http://www.who.int/vaccines-documents/docspdf05/givs_final_en.pdf. Accessed October 26, 2012.
- CDC. Global routine vaccination coverage, 2010. MMWR 2011;60:1520–2.
- Burton A, Monasch R, Lautenbach B, et al. WHO and UNICEF estimates of national infant immunization coverage: methods and processes. Bull World Health Organ 2009;87:535–41.
- World Health Organization/United Nations Children's Fund. WHO/UNICEF coverage estimates. Available at http://www.who.int/entity/immunization_monitoring/data/coverage_estimates_series.xls. Accessed October 26, 2012.
- World Health Organization. Report on the WHO quantitative immunization and vaccines related research (QUIVER): advisory committee meeting, Geneva, 4–6 October 2011. Geneva, Switzerland: World Health Organization; 2012. Available at http://whqlibdoc.who.int/hq/2012/who_ivb_12.03_eng.pdf. Accessed October 26, 2012.
- Rainey J, Watkins M, Ryman T, Sandhu P, Bo A, Banerjee K. Reasons related to non-vaccination and under-vaccination of children in low and middle income countries: findings from a systematic review of the published literature, 1999–2009. Vaccine 2011;29:8215–21.
- Decade of Vaccines Collaboration. Global vaccine action plan. Geneva, Switzerland: World Health Assembly; 2012. Available at http://www.dovcollaboration.org/action-plan. Accessed October 29, 2012.
What is already known on this topic?
Substantial progress has been made in reducing vaccine-preventable morbidity and mortality since establishment of the global Expanded Programme on Immunization in 1974. However, millions of children, especially those in less developed countries, still are not being reached by the program.
What is added by this report?
During 2011, estimated global coverage with the third dose of diphtheria-tetanus-pertussis vaccine (DTP) was 83%. Three countries (India, Nigeria, and Indonesia) accounted for 53% of the 22.4 million children who had not received 3 doses of DTP during the first year of life. Global coverage with other recommended vaccines was 88% for bacille Calmette-Guérin vaccine, 84% for the third dose of poliovirus vaccine, 84% for the first dose of measles-containing vaccine, 75% for the third dose of hepatitis B vaccine, and 43% for the third dose of Haemophilus influenzae type b vaccine. Among all incompletely vaccinated children, 62% had never received the first dose of DTP vaccine.
What are the implications for public health practice?
Although progress continues to be made, many children, especially those in less developed countries, remain at risk for vaccine-preventable diseases. Strategies to improve vaccination coverage might differ for those children who have never been vaccinated, compared with those who have started but not completed the immunization series.
FIGURE. Estimated number of children who, during the first year of life, did not receive the first dose of diphtheria-tetanus-pertussis vaccine (DTP1) or dropped out before completing the 3-dose series (DTP3), among the 10 countries with the largest numbers of incompletely vaccinated children, and the percentage of all incompletely vaccinated children worldwide represented by the 10 countries, 2011
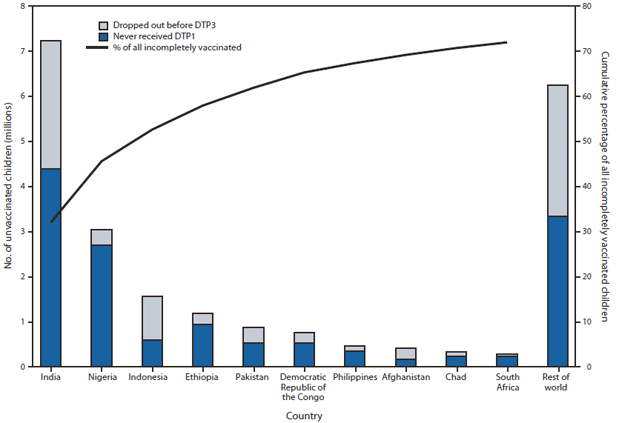
Alternate Text: The figure above shows the estimated number of children who, during the first year of life, did not receive the first dose of diphtheria-tetanus-pertussis vaccine (DTP1) or dropped out before completing the 3-dose series (DTP3), among the 10 countries with the largest numbers of incompletely vaccinated children, and the percentage of all incompletely vaccinated children worldwide represented by the 10 countries during 2011. Among the 22.4 million children who did not receive 3 DTP doses during the first year of life, 11.8 million (53%) lived in three countries, India (32%), Nigeria (14%), and Indonesia (7%), and 16.2 million (72%) lived in 10 countries.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
