|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
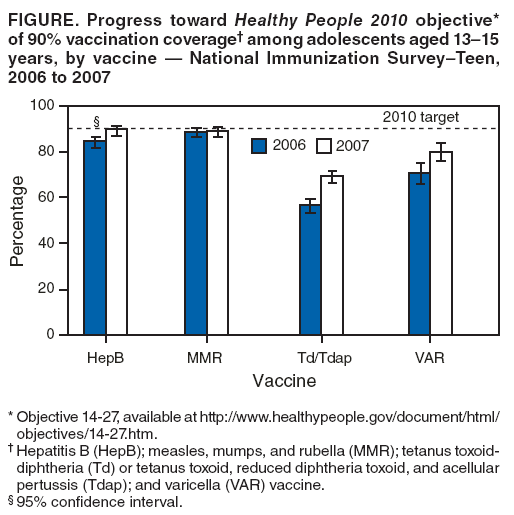
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Vaccination Coverage Among Adolescents Aged 13--17 Years --- United States, 2007Three new vaccines have been recommended for adolescents by the Advisory Committee for Immunization Practices (ACIP) since 2005: meningococcal conjugate vaccine (MCV4; 1 dose), tetanus, diphtheria, acellular pertussis vaccine (Tdap; 1 dose), and quadrivalent human papillomavirus vaccine (HPV4; 3 doses)* (1). ACIP also recommends that adolescents should receive recommended vaccinations that were missed during childhood (1). Since 2006, CDC has conducted the National Immunization Survey--Teen (NIS--Teen) to estimate vaccination coverage from a national sample of adolescents aged 13--17 years. This report describes the findings from NIS--Teen 2007, which indicated substantial increases in receipt of new adolescent vaccinations compared with 2006, including Tdap (from 10.8% to 30.4%) and MCV4 (from 11.7% to 32.4%), and increases in coverage with childhood vaccinations, including measles, mumps, and rubella (MMR), hepatitis B (HepB), and varicella (VAR) (among those without disease history). An assessment of HPV4 coverage, which is reported for the first time, showed that 25.1% of adolescent females initiated the vaccine series (>1 dose) in 2007. To improve vaccination coverage among adolescents, health-care providers should take advantage of every health-care visit as an opportunity to evaluate vaccination status and administer vaccines when needed. NIS--Teen collects vaccination information on age-eligible adolescents aged 13--17 years using a random-digit--dialing sample of telephone numbers of households. After parent/guardian respondents grant permission, surveys are mailed to the adolescents' vaccination providers to obtain vaccination histories (2). During the fourth quarter of 2007, among households identified by telephone, 81.5% were screened for an age-eligible adolescent.† Among the 9.5% in which an age-eligible adolescent lived, 83.3% (5,474) completed the household interview. Provider-reported vaccination records were obtained from 2,947 adolescents, representing 53.8% of adolescents with completed household interviews. Statistical analyses were conducted using chi-square and t-tests. Differences were considered statistically significant at p<0.05. Among adolescents aged 13--17 years, vaccination coverage with >1 dose of either tetanus and diphtheria toxoids vaccine (Td) or Tdap after age 10 years was 72.3%, a significant increase from the 60.1% coverage rate measured in 2006 (p<0.05) (Table). Coverage with 1 dose of Tdap increased from 2006 to 2007 (10.8% to 30.4%, p<0.05). Tdap coverage was significantly higher among adolescents aged 13--14 years than among those aged 15--17 years. Vaccination coverage with MCV4 was 32.4% in 2007, an increase from 11.7% in 2006 (p<0.05) (Table). No significant differences were observed among age groups. For HPV4 coverage, 25.1% of adolescent females had initiated the vaccination series (>1 dose) in 2007. No significant differences were observed among age groups (Table). Among HPV4 recipients, an estimated 32.3% (95% confidence interval [CI] = 26.5--38.7) had received 1 dose, 44.2% (CI = 37.8--50.8) had received 2 doses, and 23.5% (CI = 18.2--29.9) had received 3 doses by the interview date. Vaccination coverage with >3 doses of HepB was 87.6%, an increase from 81.3% in 2006 (p<0.05). Coverage with >2 doses of MMR was 88.9%, an increase of 2.0 percentage points compared with 2006 (Table). Significantly fewer adolescents aged 13--17 years had a reported history of varicella disease in 2007 compared with 2006 (Table). Among adolescents without a history of varicella disease, 75.7% had received >1 dose of VAR (a significant increase from 2006) and 18.8% had received >2 doses. Most adolescents (91.7%) were protected by at least 1 dose of VAR or had already had the disease. Measured against the Healthy People 2010 targets of 90% coverage (3), vaccination coverage for adolescents aged 13--15 years was 89.5% (CI = 87.3--91.3) for >3 doses of HepB, 89.0% (CI = 86.8--90.8) for >2 doses of MMR, 69.3% (CI = 66.5--72.0) for >1 dose of Td or Tdap booster, and 80.2% (CI = 76.1--83.7) for >1 dose of VAR among those without disease history. From 2006 to 2007, coverage increased 5.2 percentage points for >3 doses of HepB, 0.5 percentage points for >2 doses of MMR, 12.6 percentage points for >1 dose of Td or Tdap booster, and 9.5 percentage points for >1 dose of VAR among those without disease history (Figure). Reported by: N Jain, MD, S Stokley, MPH, D Yankey, MA, Immunization Svc Div, National Center for Immunization and Respiratory Diseases, CDC. Editorial Note:This is the second report of national adolescent vaccination coverage estimates based on provider-reported vaccination histories from the NIS--Teen (4). Comparisons with NIS--Teen 2006 results show higher coverage rates in 2007 for all vaccines, including an increase of approximately 20 percentage points for the newly recommended vaccines Tdap and MCV4. Vaccination coverage for HepB, MMR, and VAR also increased. This is the first year HPV4 coverage is being reported. The survey showed that, within 1 year after ACIP recommendations were made, approximately one in four adolescent females had initiated the vaccination series. MMR and HepB coverage levels approached the Healthy People 2010 national objective of 90% coverage. In 2007, more adolescents aged 13--14 years than those aged 15--17 years had received Tdap, rather than Td, a finding that likely reflects provider implementation of the 2006 Tdap recommendation (1). However, some younger adolescents still received Td; further study is needed to assess this finding. Older adolescents likely received Td because they were vaccinated before Tdap became available in 2005. These adolescents should now receive Tdap. Although ACIP recommends a 5-year interval between Td and Tdap, the interval can be shorter in circumstances where pertussis is circulating in the community or the risk for pertussis is high (5). This report provides the first coverage estimates for HPV4 since the ACIP recommendations were published in March 2007. Routine vaccination with HPV4 is recommended for females at age 11--12 years (1). Approximately 25% of females aged 13--17 years had initiated the HPV4 series, with no observed differences among age groups. This finding is of particular interest because studies conducted before vaccine licensure suggested that providers preferred to vaccinate older adolescent females (6). Only a quarter of HPV4 vaccination recipients had completed the 3-dose series. However, because at least 6 months is required to complete the series, some respondents who received the first dose might not have had sufficient time to complete the series by the survey interview date. Vaccine series completion will be monitored in future surveys, and the results will be used to refine strategies to promote completion of the series. As of 2007, HepB and MMR coverage among adolescents aged 13--15 years was at or near the Healthy People 2010 national targets of 90% (3). Adolescents aged 13--14 years in this survey were most likely vaccinated during early childhood, in compliance with recommendations for routine infant HepB vaccination made in 1991. According to the 1996 NIS, HepB coverage was 82% among children aged 19--35 months, corresponding to those adolescents aged 13--14 years in the NIS--Teen in 2007 (7). Coverage among older adolescents reflects implementation of recommendations made in 1999 for HepB vaccination of older children and adolescents. Although coverage among younger adolescents approached 90%, approximately 15% of older adolescents remain unprotected against hepatitis B virus infection. In 2005, ACIP recommended 2 doses of VAR for outbreak control. In 2006, ACIP expanded the 2-dose recommendation to cover persons aged >13 years who previously have not had varicella disease. This recommendation was made to further decrease varicella disease and its complications in the United States. High coverage of 1 dose of VAR has been achieved, especially among adolescents aged 13--14 years. However, coverage with 2 doses of VAR was low (18.8%) among all adolescents. For the past 10 years, professional organizations have recommended a preteen health-care visit at age 11--12 years for delivery of preventive services, including vaccinations (8). The adolescent vaccination schedule consists of both new vaccinations recommended specifically during adolescence and vaccinations recommended during early childhood that might have been missed. Optimally, adolescent vaccines should be delivered during the age 11--12 year health-care visit. Vaccinations not received at that time should be administered at the earliest opportunity. Because adolescents make few preventive health-care visits and might not visit their primary care provider routinely (8), each health-care encounter becomes an opportunity to review vaccination records and administer recommended vaccinations. Strategies to improve vaccination coverage include simultaneously administering needed vaccinations at the same visit and setting up systems to remind parents when vaccines for their adolescent are due or have been missed (9). The findings in this report are subject to at least three limitations. First, NIS--Teen is a telephone survey and some bias might remain after adjustments for nonresponse and for noninclusion of households without landline telephones. However, data from the 2006 National Health Interview Survey show that this bias is minimal; only 7.5% of adolescents were reported living in cellular-only households and 2.1% were reported having no telephone service (10). Second, NIS--Teen uses provider-reported vaccination histories, and the generalizability of the survey depends on the assumption that coverage among adolescents for whom adequate provider data were not available is similar to coverage among adolescents for whom adequate provider data were available, after controlling for factors associated with vaccine coverage. If this assumption is not correct, an underestimation or overestimation of vaccination coverage might have resulted. Finally, some provider-reported vaccination histories also might not have included all vaccinations received (e.g., vaccinations given in nontraditional settings such as emergency departments), which also might have resulted in underestimated coverage. Vaccination coverage among adolescents will continue to be monitored annually. In 2008, NIS--Teen is collecting state and local data that will provide a larger sample size adequate for examining vaccination coverage by race/ethnicity, socioeconomic status, and geographic area. References
* Protects against HPV types 6, 11, 16, and 18. † NIS--Teen 2007 was conducted during the fourth quarter 2007 only; eligible participants were born during October 7, 1988 through February 7, 1994. Similarly, NIS--Teen 2006 was conducted during the fourth quarter 2006. Table
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 10/9/2008 |
|||||||||
|