|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
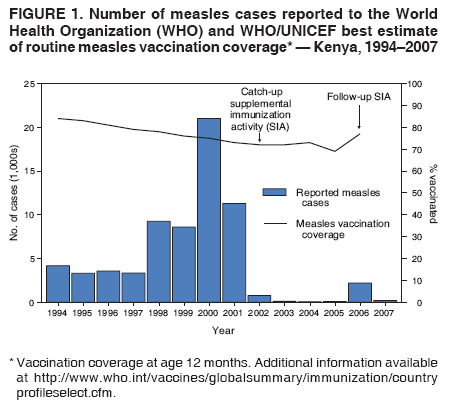
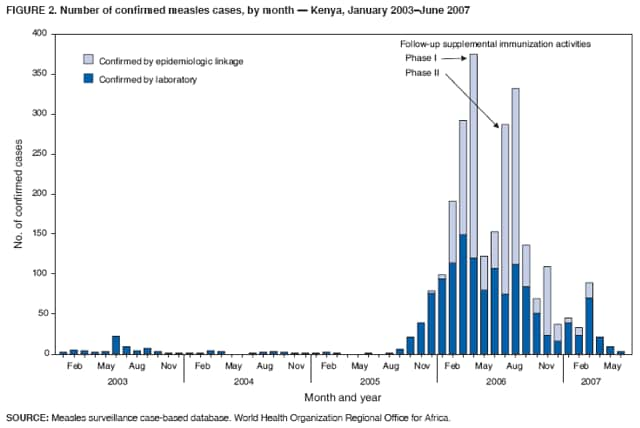
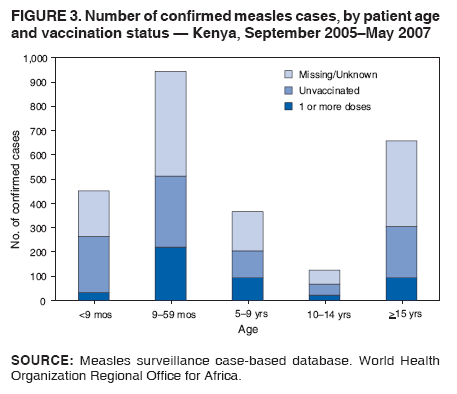
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress in Measles Control --- Kenya 2002--2007In 2000, countries represented by the World Health Organization (WHO) Regional Office for Africa established a goal to reduce, by the end of 2005, measles mortality to 50% of the 506,000 deaths from measles estimated in 1999 (1). Strategies adopted included strengthening routine vaccination, providing a second opportunity for measles vaccination through supplemental immunization activities (SIAs), monitoring disease trends, and improving measles case management. In Kenya, an east African country with a population estimated at 33.4 million in 2005, the Kenya Expanded Programme on Immunization (KEPI) in the Ministry of Health began implementing these strategies in 2002 with a wide age range catch-up SIA* and reduced the number of reported measles cases by >99%, from 11,304 in 2001 to 20 in 2004. A follow-up SIA, initially scheduled for July 2005, was postponed to 2006 to include concurrent distribution of long-lasting insecticide-treated bednets (LLINs).† This report documents progress made in reducing measles morbidity and mortality in Kenya and describes the consequences of a large measles outbreak, beginning in September 2005, on the integrated measles follow-up SIA. Immunization ActivitiesKEPI was established within the Kenya Ministry of Health in 1980, with the goal of immunizing all children in the country against six vaccine-preventable diseases.§ National coverage with 1 dose of measles vaccine (provided at age 9 months) increased in the early 1990s to 84% of children aged 12 months but decreased to 72% in 2002 (Figure 1). To accelerate measles control, goals were established in 2002 to achieve and maintain national average measles vaccination coverage at 90%, with every district expected to attain a coverage of >85%. Since then, reported national measles vaccination coverage increased to 77% in 2006 (Figure 1), and the proportion of districts with coverage >85% increased from 10% in 2002 (eight of 77 districts) to 35% in 2006 (27 of 78 districts).¶ To provide a second opportunity for measles vaccination, a nationwide measles catch-up SIA was conducted in June 2002, targeting children aged 9 months--14 years; approximately 13 million children were vaccinated, 98% of the estimated target population. A multistage cluster survey provided a similar estimate of national measles SIA coverage at 94%, with seven of nine provinces achieving coverage >90%. The two exceptions were North East Province at 84% and Coast Province at 90%. Measles SurveillanceAfter the 2002 measles catch-up SIA, Kenya implemented a system of case-based surveillance for measles within the existing surveillance network for acute flaccid paralysis. In this system, for each suspected measles patient who visits a health facility, a measles case report form is completed, and a blood specimen is taken for measles immunoglobulin M testing at the national measles laboratory. In an outbreak, defined as five or more cases reported from the same health area in a month, specimens are collected from five cases. If three or more test positive, the outbreak is confirmed as measles, untested cases are confirmed by epidemiologic linkage, and specimen collection stops after throat swabs are collected for viral genotyping. In 2003, a total of 1,791 suspected measles cases were reported through this case-based surveillance system, including 59 cases that were confirmed by laboratory or epidemiologic linkage. In 2004, a total of 1,968 suspected cases were reported, including 20 that were confirmed; in 2005, a total of 1,061 suspected cases were reported, including 151 that were confirmed. During 2003--2005, more than 99% of suspected cases were reported with a blood specimen, and the proportion of districts reporting at least one suspected measles case increased from 69% in 2004 to 99% in 2005.** Measles Outbreak and Follow-up SIAA follow-up measles SIA had been planned for July 2005, approximately 36 months after the initial catch-up SIA in June 2002, an interval between SIAs recommended by the African Regional Measles Technical Advisory Group (2). However, to expedite meeting the 2005 World Health Assembly target of 80% of children aged <5 years sleeping under an insecticide-treated bednet, the Kenya Ministry of Health and the Inter-Agency Coordinating Committee decided to integrate distribution of LLINs with the measles follow-up SIA. Raising additional funds for procurement and distribution of the LLINs required postponement of the SIA, initially to July 2006. In September 2005, a cluster of laboratory-confirmed measles cases was reported from a predominantly Somali immigrant community in Nairobi. During September 2005--May 2007, this outbreak grew to a total of 2,544 confirmed measles cases reported from 71 (91%) of the 78 districts, with peak monthly totals of 375 and 332 confirmed cases reported in April and August 2006, respectively (Figure 2). Viruses were isolated from specimens collected from approximately 80 persons and identified as genotype B3, with one additional virus from Rift Valley Province identified as D4. Of the 2,544 confirmed outbreak cases, 944 (37%) were in persons aged 9--59 months, 491 (19%) were in persons aged 5--14 years, and 658 (26%) were in persons aged >15 years. A history of measles vaccination was provided by 466 (18%) of the patients, including 220 (23%) of the 944 children aged 9--59 months and 95 (26%) of the 366 children aged 5--9 years. Vaccination status was unknown for 1,192 persons (47%) (Figure 3). During the outbreak, 24 measles deaths were documented; 17 of the decedents were children aged <5 years, and nine had a history of measles vaccination. In response to this outbreak, the planned follow-up SIA was moved forward from July to April 2006. Because adequate funds were not available to support a nationwide measles campaign in April and the full shipment of LLINs purchased for the SIA had not arrived, the SIA was divided into two phases. Phase I, conducted during April 29--May 5, covered the 16 districts most affected by measles outbreaks and most at risk for poliovirus importation from neighboring Somalia and Ethiopia (3). All the districts administered measles vaccination to children aged 9--59 months, vitamin A to children aged 6--59 months, and monovalent type 1 oral polio vaccine (mOPV1) to children aged 0--59 months. Each intervention reached more children than expected, based on population estimates; 670,016 received measles vaccine (120% of the 558,699 targeted), 785,180 received mOPV1 (119% of the 663,949 targeted), and 717,829 received vitamin A (120% of the 597,794 targeted). Phase II was conducted during July 8--12 in the 62 remaining districts. Overall, 4,590,225 children received measles vaccine (110% of the 4,180,330 targeted), and 4,716,471 received vitamin A (105% of the 4,486,266 targeted). Four districts with an estimated combined population of 181,434 (4% of the total) did not achieve 90% reported coverage with measles vaccine. Six districts also provided mOPV1 to 490,974 children (99.6% of the 492,813 targeted). LLINs were distributed to children aged <5 years in one district in April from preexisting stock and in 21 districts in July after the shipment of LLINs had arrived, reaching 1,741,005 children (104% of the estimated target population of 1,761,582). In September 2006, an additional 2 million LLINs were distributed in the remaining 23 malaria-endemic districts in Kenya. These SIAs were conducted with the support of the Measles Initiative and other partners.†† Reported by: T Kamau, MBBS, I Mugoya, MBChB, Kenya Expanded Programme on Immunization; M Duale, MD, Kenya Country Office, World Health Organization; M Eshetu, MD, Intercountry Support Team for Eastern and Southern Africa, World Health Organization, Nairobi, Kenya. BG Masresha, MD, Measles Program, Regional Office for Africa, World Health Organization, Brazzaville, Congo. P Strebel, MBChB, A Dabbagh, PhD, Dept of Immunization, Vaccines, and Biologicals, World Health Organization, Geneva, Switzerland. RT Perry, MD, T Hyde, MD, Global Immunization Div, National Center for Immunization and Respiratory Diseases, CDC. Editorial Note:Implementation of the WHO Regional Office for Africa strategies for measles mortality reduction achieved in 2004 the goal of reducing deaths caused by measles by half, both regionally and globally, from 1999 to 2005 (4). In Kenya, accelerated measles-control activities resulted in a >99% decrease in measles cases to an incidence of approximately six to 29 cases per 1 million population during the 36 months after the catch-up SIA of June 2002. Achieving high levels of vaccination coverage during that SIA, even though routine coverage was <80%, likely led to the rapid reduction in measles. In multiple countries, integrating high-priority health interventions with vaccination campaigns has attracted political support, allowed for pooling of resources, and increased community participation (5--7). Achieving high coverage with insecticide-treated bednets is a key strategy for reducing the burden of malaria. In Kenya, delaying the measles follow-up SIA by 1 year enabled distribution of LLINs to >90% of children aged <5 years in the target districts. Kenya, therefore, joins the ranks of countries that have rapidly increased coverage with insecticide-treated bednets by integrating bednet distribution with measles SIAs (5--7). However, Kenya's experience also highlights a disadvantage of delaying a follow-up SIA beyond the recommended interval. This delay likely resulted in a nationwide measles outbreak in 2005 that ultimately produced approximately 2,500 laboratory-confirmed cases and 24 deaths. Surveillance data indicate that the heaviest burden of disease was in children born after the 2002 catch-up SIA, who would have received a second opportunity for measles vaccination during the follow-up SIA. With <80% routine coverage since 1997 and the delay in the follow-up SIA, population immunity was low enough in Kenya to sustain a large outbreak after a measles importation. Successful control of measles in Kenya will depend on continued improvement of routine vaccination services; conducting regular, periodic, and high-quality follow-up SIAs; improving measles case management; and monitoring success by using case-based surveillance with laboratory confirmation. The intervals between SIAs must be based not only on disease epidemiology and SIA coverage but also on estimated routine coverage (2). In addition, despite the documented advantages of integrating measles SIAs with other life-saving interventions, in some countries, consideration should be given to the risks of delaying measles SIAs to gain the benefits from the other interventions. References
* The WHO Regional Office for Africa recommends an initial, nationwide catch-up SIA targeting all children aged 9 months--14 years and periodic nationwide follow-up SIAs targeting all children born since the last SIA. † LLINs are impregnated with an insecticide that lasts the life of the net. Conventional insecticide-treated bednets require periodic retreatment with insecticide to maintain effectiveness. § KEPI target diseases are tuberculosis, diphtheria, tetanus, pertussis, poliomyelitis, and measles. ¶ In 2003, the number of districts in Kenya was increased from 77 to 78. ** WHO Regional Office for Africa performance indicators for quality measles surveillance include collection of blood specimens from >80% of persons with suspected measles (to assess specificity) and reporting of at least one suspected measles case with a patient blood specimen from >80% of districts (to assess sensitivity). †† Founded in 2001, the Measles Initiative is a partnership formed to reduce measles mortality and is led by the American Red Cross, the United Nations Foundation, CDC, WHO, UNICEF, and the Canadian International Development Agency. The initiative has supported implementation of high-quality measles SIAs since 2000 in approximately 42 African countries. Additional information is available at http://www.measlesinitiative.org. Additional partners supporting the LLIN distribution included the Kenyan Office of the President, Ministry of Education, and Ministry of Gender, Sports, Culture, and Social Services; the Kenyan Red Cross; Rotary International; the Church of Jesus Christ of Latter-Day Saints; the United Kingdom Department for International Development; and numerous Kenyan nongovernmental organizations.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 9/19/2007 |
|||||||||
|