|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Poliomyelitis Eradication --- Pakistan and Afghanistan, January 2000--April 2002
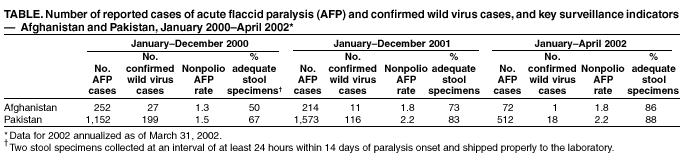
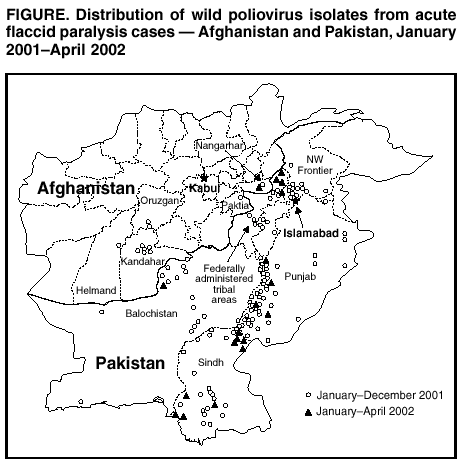
Since 1988, when the World Health Assembly resolved to eradicate poliomyelitis worldwide, the estimated global incidence of polio has decreased 99% (1). Pakistan began polio eradication activities in 1994 and Afghanistan in 1997 (2). Although polio remains endemic in the two countries, both the incidence and the geographic distribution of poliovirus have been reduced substantially. This report summarizes progress toward eradicating polio in Pakistan and Afghanistan during January 2000--April 2002. Both countries aim to stop transmission of poliovirus by the end of 2002; however, the unstable security situation in the region might threaten this success. Routine VaccinationDuring 2000--2001 in Pakistan, reported routine coverage of infants with 3 doses of oral poliovirus vaccine (OPV3) ranged from 33% in Balochistan province to 82% in Punjab. In Afghanistan, reported national routine OPV3 coverage increased from 35% in 1999 to 45% in 2001; coverage rates in 2001 ranged from 15% in the Northeastern region to 83% in the Eastern region. Supplemental Immunization ActivitiesAt least two rounds of National Immunization Days (NIDs)* have been conducted annually in Pakistan since 1994 (3). During 1999, vaccination activities were intensified by adding a house-to-house vaccination strategy and extra rounds of NIDs. Four rounds of NIDs were conducted during 2000 and five during 2001, and an additional subnational immunization day (SNID)† was conducted in August 2001. During 2002, one SNID round was conducted in January, and two rounds of NIDs were conducted in March and April. Two additional SNID rounds will be conducted in June and July, and full NIDs are planned for September and October. Surveillance and genetic sequencing data are being used to target polio-virus reservoir districts (i.e., districts in which persistent year-round indigenous transmission occurs, particularly during the low transmission season [January--March]). Following subnational campaigns during 1994--1996 that included OPV and other antigens, NIDs for polio began in Afghanistan in April and May 1997; since then, at least two rounds of NIDs have been conducted annually (4). During 2000, efforts were intensified by adding a house-to-house vaccination strategy and increasing the number of rounds of NIDs. In the spring of 2001, a house-to-house vaccination strategy was used to reach 5.8 million children; in the spring of 1999, 4.0 million children were reached by using fixed vaccination posts. Supplemental immunization activities (SIAs) have been coordinated with Afghanistan's neighbors, particularly Pakistan and Iran. During January--August 2001, three rounds of NIDs, a mop-up vaccination campaign in Kandahar and three neighboring districts, and a SNID round in high-risk provinces and districts were conducted. In September and November 2001, NIDs were conducted despite the absence of international support staff caused by armed conflict in the region. Acute Flaccid Paralysis SurveillanceThe quality of acute flaccid paralysis (AFP) surveillance is evaluated by two key WHO-established indicators: sensitivity of reporting (target: nonpolio AFP rate of >1 case per 100,000 children aged <15 years) and completeness of specimen collection (target: two adequate stool specimens§ from >80% of all persons with AFP). Since 2001, AFP surveillance in Pakistan has met these indicators. During 2000--2001, the nonpolio AFP rate increased from 1.5 per 100,000 children aged <15 years to 2.2, and the rate for adequate stool collection increased from 67% to 83% (Table). During January--April 2002, rates remained above targets, with an annualized nonpolio AFP rate of 2.2 and an adequate stool collection rate of 88%. The nonpolio enterovirus (NPEV) isolation rate (target: >10%), a marker for laboratory performance and the integrity of the reverse cold chain for specimens, was 13% in 2000 and 19% in 2001. Since Afghanistan's AFP surveillance system began in 1997, surveillance indicators have improved steadily. During 2000, the nonpolio AFP rate was 1.3, and the adequate stool collection rate was 50%; during 2001, the rates were 1.8 and 73%, respectively. In January 2001, the country switched from clinical to virologic classification of polio cases. During September--December 2001, a period marked by armed conflict, 42 AFP cases were identified (27 [64%] with adequate stool samples). AFP surveillance in the Southern region, which reported nine of the 11 polio cases in 2001, was affected more than other regions by lack of security and displacement of staff. Since January 2002, a total of 72 AFP cases has been reported nationally, with adequate specimens collected from 62 (86%) cases. The NPEV isolation rate was 19% in 2000, 16% in 2001, and 11% during January--April 2002. The WHO-accredited Regional Reference Poliovirus Laboratory in Islamabad performs virologic testing of stool specimens from both Afghanistan and Pakistan. During 2001, laboratory results were reported within 28 days of specimen receipt for 81% of the 1,584 AFP cases in Pakistan and for 72% of the 215 AFP cases in Afghanistan (target: >80%). Incidence of PolioDuring 2000--2001, the number of polio cases confirmed virologically declined 42% in Pakistan, from 199 in 59 districts to 116 in 39 districts; during January--April 2002, a total of 18 cases has been confirmed virologically (Figure). Of the 116 cases in 2001, a total of 69 was caused by polio-virus type 1 (P1), 46 by poliovirus type 3 (P3), and one by a mixture of P1 and P3. Epidemiologic data from polio cases in 2001 indicated several high-risk groups, including Afghan refugees and children whose parents are uneducated. During 2000 in Afghanistan, 27 polio cases that were confirmed virologically were reported from 22 districts; during 2001, a total of 11 cases was reported from seven districts. During January--August 2001, nine cases of wild poliovirus were reported, of which seven were from Kandahar and three neighboring districts, and two were from a district in a neighboring province. During the same period in 2000, a total of 21 polio cases was reported. No polio cases have been reported for the Northern, Northeastern, Central, and Western regions since late 2000. Each of the 11 cases (one P3 and 10 P1) reported in 2001 came from regions that border Pakistan. As of April 2002, one case of polio (P3) was confirmed in the Eastern region, with onset in February. One case has been reported in the Southern region of Afghanistan with onset in early May 2002, indicating that transmission is ongoing in that region. Reported by: National Institutes of Health; Country Office of the World Health Organization; United Nations Children's Fund, Islamabad, Pakistan. Ministry of Public Health; Country Office of the World Health Organization; United Nations Children's Fund, Kabul, Afghanistan. Regional Office for the Eastern Mediterranean Region, World Health Organization, Cairo, Egypt. Dept of Vaccines and Biologicals, World Health Organization, Geneva, Switzerland. Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Global Immunization Div, National Immunization Program, CDC. Editorial Note:Pakistan and Afghanistan constitute a single epidemiologic block representing one of the three remaining major global reservoirs for poliovirus transmission (the other two being northern India and Nigeria). Improvements in the quality of SIAs and AFP surveillance since January 2000 have brought both countries closer to interrupting poliovirus transmission. Although armed conflict in Afghanistan has posed many challenges to surveillance and vaccination activities, data from January--April 2002 indicate that progress toward eradication has resumed. The improved quality of SIAs and the addition of targeted SNID rounds in Afghanistan before September 2001 appear to have prevented a widespread resurgence of poliovirus in the country during the recent conflict. Despite continuing military and political instability, public health staff in Afghanistan and Pakistan succeeded in implementing NIDs in late September and November and continued essential surveillance activities. The AFP surveillance system in Pakistan provides reliable data on which to base programmatic decisions. AFP surveillance quality in Afghanistan appears to be recovering from a decline during the recent conflict. Rapid restoration of the system in the remaining regions bordering Pakistan where polio is endemic is a top program priority. Both countries will conduct intense SIAs targeting high-risk populations during the summer of 2002 followed by NIDs in September and October. Mop-up vaccination activities to terminate the final chains of transmission will be implemented in 2003 in response to any isolation of wild poliovirus. Vaccination and surveillance activities are coordinated closely between the two countries and include synchronization of SIAs, establishment of border vaccination posts, and regular exchange of data. A number of risks might threaten the interruption of virus transmission by the end of 2002, including armed conflict and deterioration of security throughout the region, sudden large population movements that might spread the virus to areas where it is now absent, persistence of virus transmission in reservoirs shared between the two countries, failure to reach high- risk groups in SIAs, shortfall in human and financial resources, increasing complacency, and inability to balance competing priorities. In Afghanistan, the new interim administration is committed to polio eradication, and in Pakistan, political commitment from the newly formed district governments to the federal government is high. Close collaboration between local governments and their global partners¶ has been critical in sustaining eradication activities in both countries and will continue to be essential to achieve polio eradication. References
* Nationwide mass campaigns over a short period (days to weeks) in which 2 doses of OPV are administered to all children (usually aged <5 years), regardless of vaccination history, with an interval of 4--6 weeks between doses. † Same procedure as NIDs but in a smaller geographic area. § Two stool specimens collected at an interval of at least 24 hours within 14 days of paralysis onset and shipped properly to the laboratory. ¶Polio eradication efforts in Pakistan and Afghanistan are supported by the governments of both countries, Japan, the United Kingdom, and the Netherlands; the Bill and Melinda Gates Foundation, the United Nations Foundation; the United Nations Children's Fund (UNICEF); the International Committee of the Red Cross; the International Federation of Red Cross and Red Crescent Societies; Rotary International; the U.S. Agency for International Development; WHO; and CDC.
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 6/20/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 6/20/2002