|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
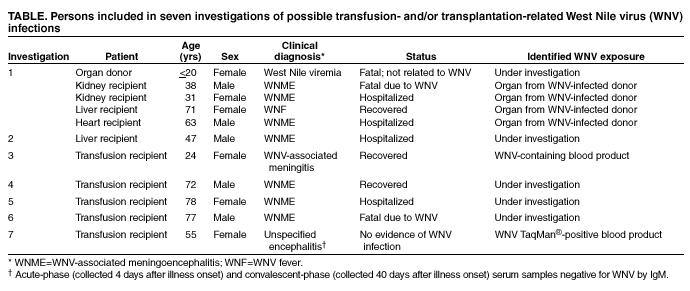
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update: Investigations of West Nile Virus Infections in Recipients of Organ Transplantation and Blood TransfusionAn investigation involving CDC, the Food and Drug Administration (FDA), the Health Resources and Services Administration (HRSA), the Georgia Division of Public Health, and the Florida Department of Health identified West Nile virus (WNV)--associated illnesses in four recipients of organs from the same donor (1,2). Although the transplanted organs were the source of infection for the four organ recipients, the source of the organ donor's infection remains unknown; an investigation of the numerous transfusions received by the organ donor is ongoing. Since the report of these cases, CDC has been informed of other patients with suspected WNV-associated meningoencephalitis (WNME) after receiving blood products within 4 weeks of illness onset. One of these patients also received an organ transplant. All of these patients resided in areas with epidemic and epizootic WNV activity; investigations are ongoing to determine whether transfusion or transplantation was the source of WNV transmission. This report summarizes two investigations of recipients of organs and blood products, four investigations of transfusion recipients, and one investigation of a WNV-seronegative person with fever and encephalopathy who received a potentially contaminated unit of blood. Investigation 1. On August 1, four organs were recovered from an organ donor and were transplanted into four persons (1,2). WNME was confirmed in three recipients and WNV fever in one recipient (Table). Illness began 7--17 days after transplantation. Although a sample of the donor's plasma collected at the time of the organ recovery was positive for WNV by kinetic quantitative PCR assay (TaqMan®), the source of the organ donor's infection is unknown. During treatment for injuries, which eventually were fatal, the organ donor received blood products from 63 unique donors. Donor follow-up has been initiated by the blood collection agency. Of 41 donors for whom retention segments* were available, 22 tested negative for WNV by TaqMan® and serology, and 19 tested negative for WNV by TaqMan®; serology testing on these 19 segments is in progress. In addition to the organ donor, 35 other persons received components derived from these 63 donors; follow-up of these recipients is pending. Untransfused components are being returned to the blood collection agency. One has tested negative for WNV by TaqMan®; testing on the others is under way. Investigation 2. A man aged 47 years received a liver transplant on August 14 and during the next 7 days received 39 units of blood products. After discharge on August 24, he was readmitted to the hospital on September 3 with fever and subsequently developed encephalopathy. A lumbar puncture revealed elevated protein, a lymphocytic pleocytosis, and WNV IgM antibody; the patient recovered and was discharged. Before organ recovery, the donor received two units of albumin and one unit of fresh frozen plasma (FFP). In addition to the liver, two kidneys were recovered and were transplanted into one recipient, whose clinical status is being investigated. Investigation 3. During July 27--28, a woman aged 24 years received 18 units of blood products (12 units of packed red blood cells [PRBC] and six units of FFP) because of postpartum hemorrhage. On August 1, she was discharged. The patient developed worsening headache and fever and 22 days later was readmitted to the hospital with meningitis. A lumbar puncture revealed a lymphocytic pleocytosis; serum and CSF samples were positive for WNV by IgM. Retention segments were available from 15 of the 18 donations administered in July; three (20%) were positive for WNV by TaqMan®. Of three components derived from a donation associated with these positive segments, one unit of FFP was retrieved, tested, and found to be positive for WNV by TaqMan®; viable WNV also was isolated from this plasma. The donor of this blood component sought medical care 4 days after donation because of fever, chills, and headache; follow-up WNV-antibody testing of this donor is in progress. Investigation 4. A man aged 72 years with a history of myelodysplasia and frequent blood transfusions received four units of PRBC during July 18--August 7. The patient was admitted on August 8 with generalized weakness and fever. A serum sample obtained 2 days later was positive for WNV by IgM. No retention segments were available. Of five components derived from these four donations, four units of FFP were retrieved, and testing is in progress. One unit of platelets was transfused into another recipient, and follow-up is pending. Investigation 5. On July 17, a woman aged 78 years received two units of PRBC 1 day after a surgical amputation. Three days after receiving the transfusions, she developed fever, altered mental status, and seizures. Acute- and convalescent-phase serum samples and CSF were positive for WNV by IgM. Retention segments associated with both units of PRBC were negative for WNV by TaqMan® and by IgM. Follow-up of the two donors and a patient who received platelets from one of these donors is in progress. Investigation 6. During July 26--August 23, a man aged 77 years who required frequent blood transfusions for myelodysplasia received eight units of blood products (four units of PRBC and four units of single-donor platelets). On August 23, the patient developed fever and headache. Serum and CSF samples were positive for WNV-specific IgM. The patient had progressive encephalopathy and died. Four retention segments were available for four of the eight donations; all were negative for WNV by TaqMan®. Follow-up is ongoing for three patients who received platelets from three of the eight donors. In addition, four units of plasma have been withdrawn and are being tested. Investigation 7. On July 26, a woman aged 55 years received three units of PRBC after an orthopedic procedure. The following day, she developed fever and encephalopathy. Serum samples collected on the fourth and 40th days after illness onset were negative for WNV by IgM. Retention segments were available from all donations; two were negative for WNV by TaqMan®. One was positive for WNV by TaqMan® but negative for WNV-specific IgM; serum collected from the donor 69 days after donation was positive for WNV-specific IgM, reflecting WNV seroconversion. The donor denied fever, headache, or other symptoms during the 3 weeks before or after the donation. A patient undergoing cardiac surgery received a unit of FFP from this donation. A serum sample collected from this patient was negative for WNV by IgM. Follow-up serum samples are being collected for the index case and for the recipient of the FFP. Reported by: L Shireley, MPH, K Kruger, T Miller, MPH, D Johnson, MS, North Dakota Dept of Health. S Lance-Parker, DVM, Georgia Dept of Human Resources, Div of Public Health. R Ratard, MD, Louisiana Office of Public Health. M Currier, MD, Mississippi State Dept of Health. MG Stobierski, DVM, L Scott, D Johnson, MD, G Stoltman, PhD, Michigan Dept of Community Health. S Wiersma, MD, M Trepka, MD, C Blackmore, PhD, Florida Dept of Health. M Chamberland, MD, S Zaki, MD, J Guarner, MD, W Shieh, MD, C Goldsmith, MS, J Sejvar, MD, P Rollins, PhD, Div of Viral and Rickettsial Diseases; M Kuehnert, MD, D Jernigan, MD, Div of Healthcare Quality Promotion; L Chapman, MD, Div of AIDS, STD, and TB Laboratory Research; L Petersen, MD, A Marfin, MD, G Campbell, MD, R Lanciotti, PhD, J Roehrig, PhD, Div of Vector-Borne Infectious Diseases, National Center for Infectious Diseases; A Winquist, MD, Div of Applied Public Health Training, Epidemiology Program Office; D Withum, Div of HIV/AIDS Prevention, National Center for HIV, STD, and TB Prevention; M Iwamoto, MD, T Harrington, MD, M Haddad, MSN, A Vicari, DVM, J Montgomery, MD, EIS officers, CDC. Editorial Note:CDC, FDA, HRSA, blood collection agencies, and state and local health departments continue to investigate possible transmission of WNV through blood transfusion or organ transplantation. The initial investigation demonstrated transmission from a WNV-viremic organ donor to four recipients of those organs. In another investigation (Investigation 3), the isolation of live WNV from a unit of FFP indicates that the virus can survive in some blood components and probably can be transmitted by transfusion. Although this case is highly suspicious for transfusion-associated transmission, this patient lived in an area where WNV was active, and the exact means of WNV acquisition cannot be determined. In contrast, the preliminary results of another case investigation (Investigation 7) indicate that not all recipients of potentially WNV-contaminated units (i.e., those that are positive for WNV by TaqMan®) will become infected with WNV. The Public Health Service (PHS) recommends several precautionary measures to reduce the possible risk for WNV transmission by organ transplantation or blood transfusion. Patients with WNV infection who have received blood transfusions or organs within 4 weeks preceding symptom onset should be reported to CDC through local public health authorities to initiate an investigation. Serum or tissue samples should be retained for later studies. In addition, patients with WNV infection who have onset of symptoms within 1 week of blood or organ donation should be reported. Prompt reporting of these persons will facilitate withdrawal of potentially infected blood components. HRSA has alerted organ transplant organizations about the potential for transplantation-associated WNV infection.
Tests for WNV suitable for routine blood donor screening are not available. However, FDA is working with public and private partners to facilitate development of such tests to ensure their availability if screening is necessary. FDA is developing additional guidance for blood centers to enhance reporting of post-donation illnesses suggestive of WNV infection and to determine when retrieval of recent blood collections from these donors is warranted. Approximately 4.5 million persons receive blood or blood products annually. Although persons needing blood transfusions or organ transplants should be aware of the risk for WNV infection, the benefits of receiving needed transfusions or transplants outweigh the potential risk for WNV infection. In addition, blood donation poses no risk to the donor for acquiring WNV, and PHS encourages blood donation. References
* Blood samples from tubing that had been attached to the original donor collection bag.
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
Page converted: 9/19/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 9/19/2002