 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Poliomyelitis Eradication During Armed Conflict -- Somalia and Southern Sudan, January 1998-June 1999In 1988, the Regional Committee of the World Health Organization (WHO) for the Eastern Mediterranean Region* adopted a resolution to eliminate poliomyelitis from the region by 2000 (1). Somalia and parts of southern Sudan have persons living in areas where there is ongoing armed conflict and poor infrastructure (e.g., health-care facilities, schools, roads, and power plants). Under these conditions, conducting National Immunization Days** (NIDs) and acute flaccid paralysis (AFP) surveillance is difficult. This report summarizes NIDs in Somalia during 1997 and 1998 and in southern Sudan*** during 1998 and 1999 and establishment of AFP surveillance in northern Somalia and southern Sudan. SOMALIA Health-Care Delivery and Routine Vaccination Coverage Health-care services to the estimated 5.8 millions persons residing in Somalia are delivered through national and international nongovernmental organizations (NGOs), supported by United Nations Children's Fund (UNICEF), WHO, and other United Nations (UN) agencies. Somalia is divided into four zones: south, central, northeast, and northwest. At the end of 1996 and in early 1997, in the northeast and northwest zones, routine vaccination coverage with three doses of oral poliovirus vaccine (OPV) among children aged 12-23 months was 27% and 28%, respectively. Estimated coverage was lower in the southern and central zones (UNICEF, unpublished data, 1999). National Immunization Days In 1997, the first Subnational Immunization Days**** (SNIDs) were conducted in the two northern zones of Somalia. The first and second round of SNIDs reached an estimated 330,000 children aged 0-59 months. In 1998, the first round of NIDs covering the entire country was planned. Partnerships were developed between local and international NGOs and Somali nationals, who were then trained to conduct NIDs in all areas of the country. This was the first nationwide activity carried out by Somali communities since civil war began in 1991. In August and September 1998, southern Somalia held its first NIDs, followed by northern Somalia in November and December. Three thousand Somali workers administered OPV throughout Somalia and reached almost all settlements. AFP Surveillance In April 1998, AFP surveillance began in northern Somalia at 65 reporting sites selected for regular surveillance through active case detection visits. By February 1999, AFP surveillance had expanded to 117 sites. During May 1998-May 1999, 32 AFP cases were reported (Table 1); of these, 10 (31%) were confirmed***** as polio (Figure 1). The nonpolio AFP rate for both northern zones was 2.3 per 100,000 children aged less than 15 years. Adequate****** stool specimens were collected from all 10 case-patients. Eighty-six percent of case-patients had a 60-day follow-up examination. AFP surveillance is planned to begin in the southern and central zones in late 1999. SOUTHERN SUDAN Health-Care Delivery and Routine Vaccination Coverage The regions of Bahr El Ghazal, Equatoria, and Upper Nile have experienced continuous armed conflict since 1984. Health-care services to the estimated 5.4 million persons affected are implemented through the southern sector of Operation Lifeline Sudan (OLS)*******, with the Sudanese government also providing services in some areas. Many persons do not have access to any health-care services. Reported routine vaccination coverage with three doses of OPV was less than 20%, although specific coverage statistics are not available for most areas (Operation Lifeline Sudan, southern sector, unpublished data, 1999). National Immunization Days In 1998, the first round of NIDs that included all of southern Sudan began in February. The second round took place in March in Equatoria and Upper Nile. NIDs occurred 1 month later in Bahr El Ghazal. The 1999 NIDs were held in February (first round) and March (second round). Eighty-three Sudanese workers who were recruited and trained to assist in NIDs coordinated with local leaders and NGOs to develop a plan of action. Vaccine vial monitors (VVMs) were used to confirm that OPV remained potent in remote areas. Five thousand Sudanese volunteers administered OPV to persons in every county and district served by OLS. AFP Surveillance UNICEF, WHO, NGOs, and local staff selected 25 sentinel sites for AFP surveillance throughout Bahr El Ghazal, Equatoria, and Upper Nile. Sites were chosen on the basis of a functioning health-care facility, a large catchment population, a health NGO, and reliable access by air or road. In November 1998, AFP surveillance began at 19 (76%) of the 25 selected sites. Implementation in the remaining sites is ongoing. During November 1998-April 1999, 17 AFP cases were reported (Table 1); eight (47%) were confirmed as polio (Figure 1)--one by isolation of wild virus from a stool specimen and seven by clinical classification. Of the remaining nine cases, two were classified as nonpolio, and classification of seven cases is pending. Pending cases are classified as nonpolio (2), resulting in an annualized AFP nonpolio rate of 0.67 per 100,000 children aged less than 15 years. Adequate stool specimens were collected for three (18%) case-patients. Wild poliovirus type 3 was isolated from a stool specimen from a patient in Mapel, Wau County, and vaccine virus was isolated from the two other stool specimens. Forty-one percent of all case-patients had a 60-day follow-up examination. Reported by: Operation Lifeline Sudan, southern sector; United Nations Children's Fund Country Program for Somalia, Nairobi, Kenya. Offices of the World Health Organization for the Eastern Mediterranean; Offices of the United Nations Children Fund for East and Southern Africa Region. United Nations Children's Fund, New York. Vaccines and Other Biologicals Dept, World Health Organization, Geneva, Switzerland. Respiratory and Enteric Viruses Br, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Vaccine Preventable Disease Eradication Div, National Immunization Program, CDC. Editorial Note:At the end of 1998, poliovirus was suspected or known to circulate in 10 countries in civil conflict********, eight of which are on the African continent. Recognizing that these countries are essential to reaching the polio eradication goal, the UN is advocating for days of tranquility during vaccination activities. In addition, the findings in this report demonstrate that even in the absence of formally negotiated cease-fires, polio eradication activities can be conducted effectively. In both Somalia and southern Sudan, the following factors made achieving high coverage during NIDs possible: 1) strong partnerships between UN agencies, NGOs, and local leaders and communities; 2) involvement of Sudanese and Somali nationals in administering vaccine and widespread campaign coverage, compared with health activities limited to selected areas or agencies; and 3) commitment of funds and other resources necessary to overcome existing infrastructure limitations. In Somalia, extensive social mobilization efforts were conducted by district and local leaders to develop a plan of action for vaccination campaigns. In southern Sudan, coordination with the Sudanese government and with Sudanese workers, local leaders, and NGOs to plan and implement NIDs also were effective. Use of VVMs minimized dependence on freezing capacity and maximized the mobility of vaccination teams. In southern Sudan, the experience gained during NIDs of how to reach successfully those persons who were not reached previously by routine vaccination presents an opportunity for the Expanded Program on Immunization (EPI) to develop other strategies. In addition, resources (e.g., vaccine carriers, cold boxes, freezers, bicycles, and vehicles) left with the routine EPI programs also can help to improve routine coverage. AFP surveillance was implemented in northern Somalia and southern Sudan, and these data are being used to target supplementary vaccination strategies. The late presentation of cases to sentinel sites in southern Sudan presented a challenge, and expansion beyond existing sentinel sites is needed. Establishing AFP surveillance in southern and central Somalia is a priority. Progress toward polio eradication in countries with civil unrest, insecurity, and low routine coverage with OPV is critical for the success of the global polio eradication initiative. Reaching almost all areas and settlements in Somalia and southern Sudan during NIDs and the ability of newly established AFP surveillance systems to successfully detect and investigate AFP cases demonstrate that global polio eradication is achievable, even in adverse circumstances. These findings should encourage other countries to implement the key programs that will lead to global polio eradication. References
* Member countries are Djibouti, Egypt, Libya, Morocco, Somalia, Sudan, and Tunisia in northern and eastern Africa; the Arab Gulf states of Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, United Arab Emirates, and Yemen; Iraq, Jordan, Lebanon, Syria, and the Palestinian people in the Middle East; Afghanistan, Iran, and Pakistan in Asia; and Cyprus. ** Nationwide mass campaigns over a short period (days to weeks) in which two doses of OPV are administered to all children in the target age group (usually aged less than 5 years), regardless of previous vaccination history, with and interval of 4-6 weeks between doses. *** NIDs in Somalia and southern Sudan were implemented with the cooperation of local health authorities and the government of Sudan, and supported by national and international nongovernment organizations, Rotary International, the United Nations Foundation, the United Nations Children's Fund (UNICEF), the UNICEF national committees of the United States and the United Kingdom, WHO, and CDC. **** Focal mass campaigns in high-risk areas over a short period (days to weeks) in which two doses of OPV are administered to all children in the target age group, regardless of vaccination history, with an interval of 4-6 weeks between doses. ***** A confirmed case of polio is defined as AFP and at least one of the following: 1) laboratory-confirmed wild poliovirus infection, 2) residual paralysis at 60 days, 3) death, or 4) no follow-up investigation at 60 days. ****** Two stool specimens collected at an interval of at least 24 hours within 14 days of onset of paralysis. ******* OLS is a consortium led by UNICEF that includes several UN agencies and more than 40 nongovernmental agencies. ******** Afghanistan, Angola, Democratic Republic of the Congo, Eritrea, Ethiopia, Liberia, Sierra Leone, Somalia, Sudan, and Tajikistan. Table 1 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 1. Number of children aged 0-59 months*, number receiving oral poliovirus
vaccine (OPV) during National Immunization Days+ (NIDs), number of reported cases
of acute flaccid paralysis (AFP), and nonpolio AFP rate& -- southern Sudan and
northern Somalia, 1998-1999
=====================================================================================================================
AFP Surveillance
----------------------------------
National Immunization Days % persons
No. ------------------------------------------------ with AFP
children 1998 1999 No. with
aged --------------------- ------------------------- reported Nonpolio adequate@
Country/Region <5 years Round 1 Round 2 Round 1 Round 2 AFP cases AFP rate specimens
-------------------------------------------------------------------------------------------------------------------
Somalia
Northwest 247,320 217,666 212,616 Planned for 14 1.4 38
Northeast 168,104 120,572 124,831 November/ 18 3.6 22
December
1999
Central 931,245 873,378 989,716 Planned for NA NA NA
South 176,462 190,081 206,192 August/ NA NA NA
September
1999
Total 1,523,131 1,401,697 1,533,355 NA NA NA
Southern Sudan**
Bahr El Ghazal 378,668 330,899 315,023 441,610 484,922 10 0.6 20
Upper Nile 284,183 207,857 244,723 362,861 394,914 4 1.1 25
Equatoria 261,546 177,438 218,224 196,660 260,816 3 0.6 0
Total 924,397 716,194 777,970 1,001,131 1,140,652 17 0.7 18
------------------------------------------------------------------------------------------------------------------
* Population denominator data varied widely depending on the source and cannot be used to calculate
coverage or total population. The numbers shown were used for planning purposes only and do not
reflect an endorsement of any estimate.
+ Nationwide mass campaigns over a short period (days to weeks), in which two doses of OPV are
administered to all children in the target age group (usually aged <5 years), regardless of previous
vaccination history, with an interval of 4-6 weeks between doses.
& Per 100,000 children aged <15 years.
@ Two stool specimens collected 24 hours apart and <14 days after the onset of paralysis.
** Does not include areas covered by the government of Sudan.
=====================================================================================================================
Return to top. Figure 1 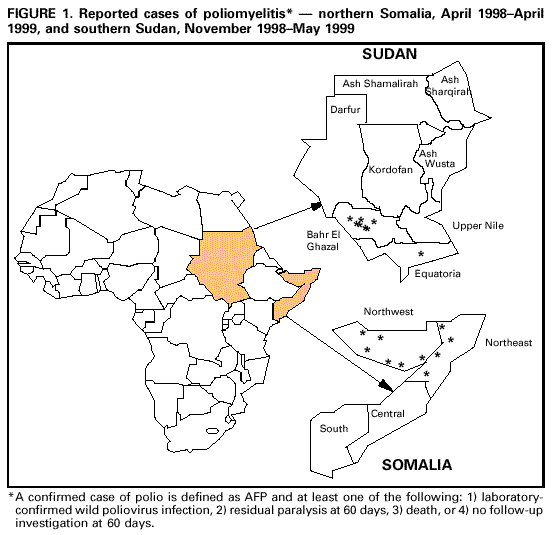 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 7/29/99 |
|||||||||
This page last reviewed 5/2/01
|