Funding

Public Health Emergencies
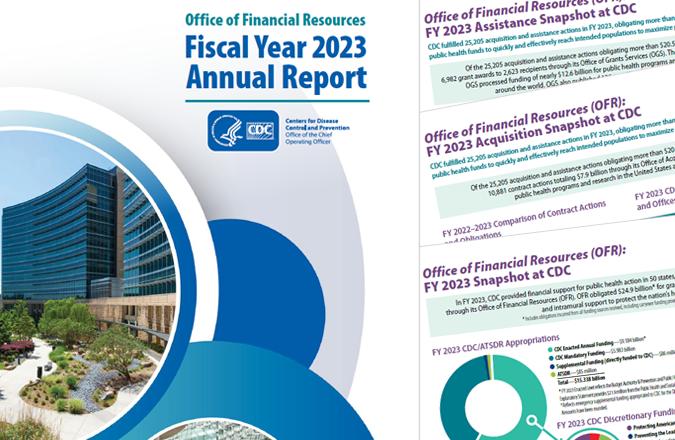
Office of Financial Resources Fiscal Year 2023 Annual Report and Snapshots
Calculating Your Next Move?
Consider a role with the CDC's Office of Financial Resources (OFR)

Understanding the Difference: Acquisition and Assistance

CDC and Small Business

CDC Grant Funding Eligibility

CDC's Budget Request
The Centers for Disease Control and Prevention’s (CDC) Office of Financial Resources (OFR) aids in achieving CDC’s mission by quickly and effectively allocating funds to where they are needed. In its Pledge to the American People, CDC commits to being a diligent steward of the funds entrusted to the Agency. OFR ensures this pledge remains intact. To learn more about OFR, please review our Fiscal Year 2023 Annual Report, OFR Snapshot, Acquisition Snapshot, and Assistance Snapshot.
What's New - Funding
- FY 2024 CDC Operating Plan5/15/2024 10:30:00 AM
- FY 2025 CDC/ATSDR Congressional Justifications3/11/2024 1:56:00 PM
- FY 2025 Budget Overview Factsheet3/11/2024 1:30:00 PM
- Update to PMS Login Process 2/15/2024 4:00:00 PM
- CDC OFR FY 2023 Acquisition Snapshot1/30/2024 11:09:00 AM
- OFR Fiscal Year 2023 Annual Report and Snapshots1/30/2024 10:52:00 AM
- CDC Office of Financial Resources FY 2022 OFR Snapshot1/26/2023 12:12:00 PM
- FY 2022 Report on CDC-Hosted Scientific Meetings12/20/2022 8:05:00 AM
- FY 2022 CDC Conference Reports12/20/2022 8:01:00 AM
- FY 2022 Report on Non-CDC-Hosted Scientific Meetings12/16/2022 7:47:00 AM
Budget

View CDC’s financial goals, objectives, and data analysis in budget requests for each fiscal year.
Contracts

CDC uses contracts to purchase goods and services for the use and benefit of the agency.

