Reasons for Emergency Room Use Among U.S. Children: National Health Interview Survey, 2012
- Key findings
- Children with Medicaid coverage were more likely to have at least one ER visit in the past year, compared with the uninsured and those with private coverage.
- For three in four children with an ER visit in the past 12 months, the most recent visit was at night or on a weekend, regardless of health insurance coverage status.
- Children with Medicaid were less likely than children with private insurance to visit the ER for reasons reflecting the seriousness of the medical problem.
- Among those visiting the ER for reasons reflecting the seriousness of the medical problem, the most common reason was that only a hospital could help.
- Among children whose most recent ER visit was for reasons other than those reflecting the seriousness of the medical problem, the most common reason was because their doctor’s office was not open.
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 160, July 2014
PDF Version (430 KB)
Renee M. Gindi, Ph.D., and Lindsey I. Jones, M.P.H.
Key findings
Data from the National Health Interview Survey, 2012
- In 2012, children with Medicaid coverage were more likely than uninsured children and those with private coverage to have visited the emergency room (ER) at least once in the past year.
- About 75% of children’s most recent visits to an ER in the past 12 months took place at night or on a weekend, regardless of health insurance coverage status.
- The seriousness of the medical problem was less likely to be the reason that children with Medicaid visited the ER at their most recent visit compared with children with private insurance.
- Among children whose most recent visit to the ER was for reasons other than the seriousness of the medical problem, the majority visited the ER because the doctor’s office was not open.
Emergency rooms (ERs) are intended to provide care for acute and life-threatening medical conditions for people of all ages, but use is highest among older adults and young children (1). In 2012, 18% of children aged 0–17 years visited the ER at least once in the past year (2). Rising health care costs make it important to understand the reasons that families with children seek ER care, rather than less expensive office-based or outpatient care (3). Families visiting the ER at night or on weekends may have different characteristics or reasons for using the ER than those who visit during the day (4). Previous research among adults found that the majority visited the ER because “only a hospital could help,” or the “doctor’s office [was] not open” (5). This report provides comparable statistics on reasons for children’s ER use.
Keywords: health care utilization, health insurance
Children with Medicaid coverage were more likely to have at least one ER visit in the past year, compared with the uninsured and those with private coverage.
Figure 1. Children aged 0–17 years with at least one emergency room visit in the past 12 months, by health insurance coverage status: United States, 2012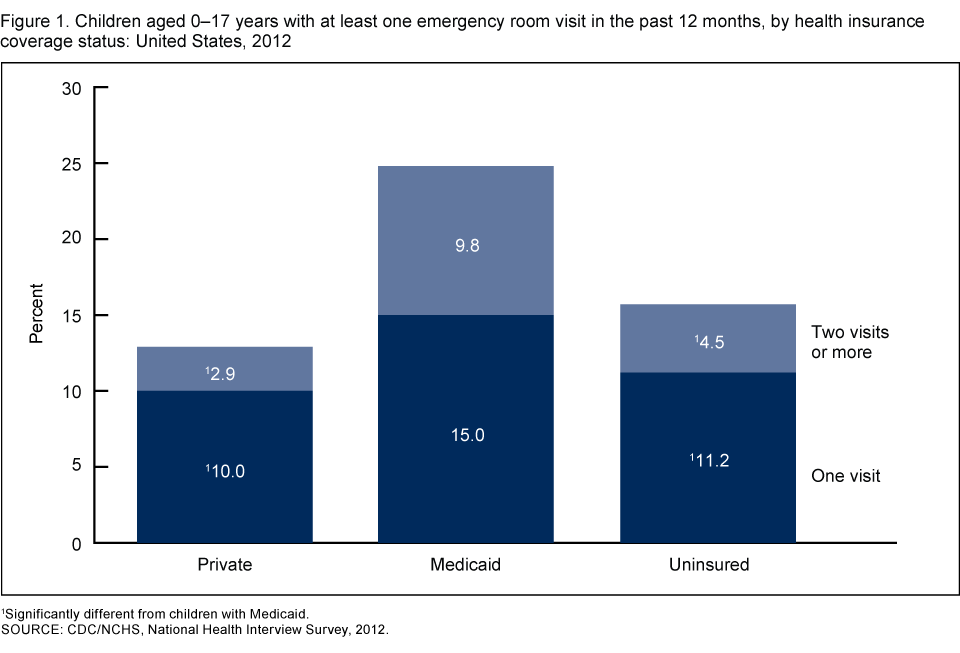
1Significantly different from children with Medicaid.
SOURCE: CDC/NCHS, National Health Interview Survey, 2012.
In 2012, almost one in four children aged 0–17 with Medicaid coverage visited the ER at least once in the past 12 months (24.8%) (Figure 1). This was significantly higher than the percentage of uninsured children (15.7%) and the percentage of children with private insurance (12.9%) who visited the ER at least once in the past 12 months. This relationship was seen for both those visiting the ER only once and those visiting two times or more in the past 12 months.
For three in four children with an ER visit in the past 12 months, the most recent visit was at night or on a weekend, regardless of health insurance coverage status.
Among children with at least one ER visit in the past 12 months, almost 75% of the most recent ER visits were at night or on a weekend (Figure 2). This percentage was similar for children with private insurance (71.4%), Medicaid (75.4%), and those who were uninsured (75.0%).
Figure 2. Timing of most recent emergency room visit among children aged 0–17 years with an emergency room visit in the past 12 months, by health insurance coverage status: United States, 2012

SOURCE: CDC/NCHS, National Health Interview Survey, 2012.
Children with Medicaid were less likely than children with private insurance to visit the ER for reasons reflecting the seriousness of the medical problem.
Among privately insured children with at least one ER visit in the past 12 months, 67.9% of most recent ER visits were for a reason reflecting the seriousness of the medical problem, compared with 60.6% of children with Medicaid and 59.0% of uninsured children (Figure 3). Children with Medicaid (32.9%) who had at least one ER visit in the past 12 months were more likely than those with private insurance (26.4%) to visit most recently for a reason other than those reflecting the seriousness of the medical problem. No reasons were selected for a smaller percentage of most recent ER visits (6.5%).
Figure 3. Selected reasons for most recent emergency room visit among children aged 0–17 years with an emergency room visit in the past 12 months, by health insurance coverage status: United States, 2012
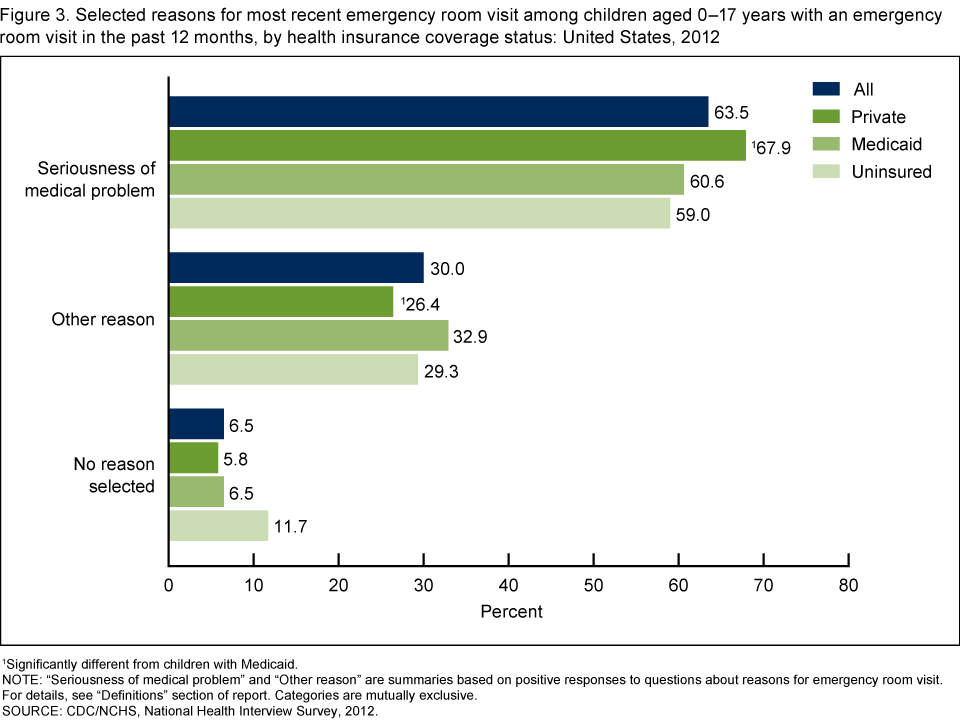
1Significantly different from children with Medicaid.
NOTE: “Seriousness of medical problem” and “Other reason” are summaries based on positive responses to questions about reasons for emergency room visit. For details, see “Definitions” section of report. Categories are mutually exclusive.
SOURCE: CDC/NCHS, National Health Interview Survey, 2012.
Among those visiting the ER for reasons reflecting the seriousness of the medical problem, the most common reason was that only a hospital could help.
“Only a hospital could help” (79.1%) and “the problem was too serious for a doctor’s office” (62.0%) were the most common reasons for the most recent ER visit related to the seriousness of the medical problem among children aged 0–17 who had an ER visit reflecting the seriousness of the medical problem in the past 12 months (Figure 4). Of children who visited the ER for a reason reflecting the seriousness of the medical problem, privately insured children were the most likely to visit the ER because a health provider said to go (43.4%), compared with children with Medicaid (36.3%) and uninsured children (19.5%). Less than 10% of children’s most recent ER visits related to the seriousness of the medical problem were because the child arrived at the ER by ambulance.
Figure 4. Selected reasons for most recent emergency room visit among children aged 0–17 years who had an emergency room visit in the past 12 months for a reason reflecting the seriousness of the medical problem, by health insurance coverage status: United States, 2012

1Significantly different from uninsured children.
* Estimate has a relative standard error greater than 30% and less than or equal to 50% and is considered unreliable. Estimate should be used with caution.
NOTE: “Seriousness of medical problem” is a summary based on positive responses to any of the related detailed reasons included in this figure. Respondents could select more than one reason.
SOURCE: CDC/NCHS, National Health Interview Survey, 2012.
Among children whose most recent ER visit was for reasons other than those reflecting the seriousness of the medical problem, the most common reason was because their doctor’s office was not open.
Among children aged 0–17 whose most recent visit to the ER in the past 12 months was for a reason other than the seriousness of the medical problem, there were no significant differences in reasons by insurance type (Figure 5). The most common reason for the most recent ER visit was that the “doctor’s office [was] not open” (86.0%).
Figure 5. Selected reasons for most recent emergency room visit among children aged 0–17 years whose emergency room visit in the past 12 months was for a reason other than the seriousness of the medical problem, by health insurance coverage status: United States, 2012
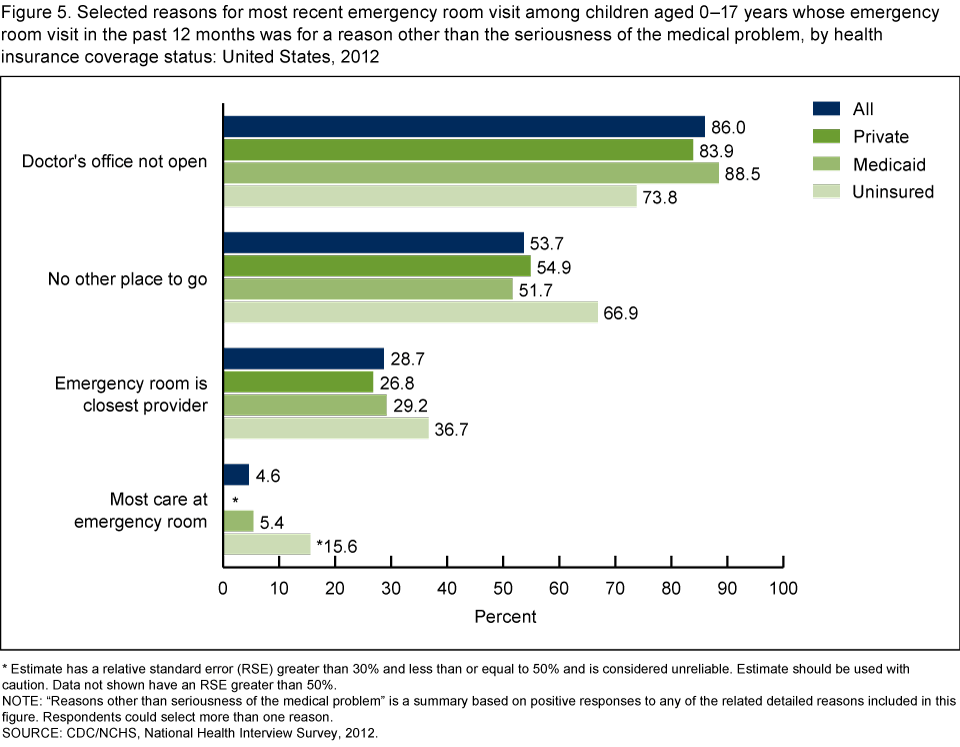
* Estimate has a relative standard error (RSE) greater than 30% and less than or equal to 50% and is considered unreliable. Estimate should be used with caution. Data not shown have an RSE greater than 50%.
NOTE: “Reasons other than seriousness of the medical problem” is a summary based on positive responses to any of the related detailed reasons included in this figure. Respondents could select more than one reason.
SOURCE: CDC/NCHS, National Health Interview Survey, 2012.
Summary
During 2012, children with Medicaid were more likely to have had at least one ER visit compared with children with private insurance or uninsured children. Approximately 75% of children’s most recent ER visits were at night or on the weekend, and this percentage was similar regardless of health insurance coverage status. Approximately two-thirds of children’s most recent visits to the ER were due to reasons that reflected the seriousness of the medical problem, and this differed by health insurance coverage status. Children with Medicaid were less likely to visit the ER because of reasons reflecting the seriousness of the medical problem and more likely to visit for other reasons. Similar to adults aged 18–64, common reasons for children’s most recent ER visits were because “only a hospital could help” and the “doctor’s office [was] not open” (5). Some reasons for ER visits (e.g., “no other place to go” and “doctor’s office [was] not open”) may depend on whether a child has a regular source of care, an association seen previously among adults (5). Recent changes to children’s health insurance coverage make it important to monitor the rates, timing, and reasons for ER use by health insurance coverage status.
Definitions
Emergency room visit: Based on the response provided to the question “During the past 12 months, how many times has [sample child] gone to a hospital emergency room about [his/her] health? (This includes emergency room visits that resulted in a hospital admission.)”
Health insurance coverage: The “private insurance coverage” category includes children who had any comprehensive private insurance plan (including health maintenance and preferred provider organizations). These plans include those obtained through an employer, purchased directly, or purchased through local or community programs. Private coverage excludes plans that pay for only one type of service, such as accidents or dental care. The “Medicaid” category includes children without private insurance who reported Medicaid, Children’s Health Insurance Program (CHIP), and other state-sponsored health plans. Children were defined as uninsured if they did not have any private insurance, Medicare, Medicaid, CHIP, state-sponsored or other government-sponsored health plan, or military plan at the time of interview. Children also were defined as uninsured if they had only Indian Health Service coverage or had only a private plan that paid for one type of service, such as accidents or dental care.
Reasons for last emergency room visit: Respondents who indicated that the sample child had visited the emergency room at least once in the past 12 months were then asked, “Tell me which of these apply to [sample child’s] last emergency room visit? ‘you didn’t have another place to go,’ ‘your doctor’s office or clinic was not open,’ ‘your health provider advised you to go,’ ‘the problem was too serious for the doctor’s office or clinic,’ ‘only a hospital could help you,’ ‘the emergency room is your closest provider,’ ‘you get most of your care at the emergency room,’ ‘you arrived by ambulance or other emergency vehicle.’” Respondents could select more than one reason, and reasons were not mutually exclusive. Three mutually exclusive categories of reasons for last ER visit were developed: children who went to the ER due to reasons reflecting the seriousness of medical problem, those who went for reasons other than the seriousness of the medical problem, and those who did not select any of the reasons listed.
“Seriousness of medical problem” is a summary based on positive responses to any of the following: “your health provider advised you to go,” “the problem was too serious for the doctor’s office or clinic,” “only a hospital could help you,” or “you arrived by ambulance or other emergency vehicle.” Among children who did not attend the ER for a reason reflecting the seriousness of the medical problem, “Other reason” is a summary based on positive responses to any of the following: “you didn’t have another place to go,” “your doctor’s office or clinic was not open,” “the emergency room is your closest provider,” or “you get most of your care at the emergency room.”
Timing of last emergency room visit: Based on the response provided to the question “Thinking about [sample child’s] most recent emergency room visit, did [he/she] go to the emergency room either at night or on the weekend?”
Data source and methods
The National Health Interview Survey (NHIS) is a multipurpose health survey conducted continuously throughout the year by the Centers for Disease Control and Prevention’s (CDC) National Center for Health Statistics (NCHS). Interviews are conducted in respondents’ homes, but follow-ups to complete interviews may be conducted over the telephone. A sample child is randomly selected from each family in NHIS, and information about the sample child is obtained from an adult residing in the household who is knowledgeable about the child’s health (usually the parent). Questions about children’s ER use are from the Sample Child Core and Supplemental components of the survey. Questions about health insurance are from the Family Core component. Information was collected for 13,275 children.
Survey design and weighting procedures are described in more detail elsewhere (6). To account for the complex sample design of NHIS, point estimates and significance tests (using p < 0.05) were calculated using SUDAAN software, version 11.0.0 (RTI International, Research Triangle Park, N.C.). The Taylor series linearization method was chosen for variance estimation. All estimates shown in this report meet the NCHS standard of reliability (relative standard error less than or equal to 30%) unless otherwise noted. For further information about NHIS, including the questionnaire, visit the NHIS website.
About the authors
Renee M. Gindi and Lindsey I. Jones are with CDC’s National Center for Health Statistics, Division of Health Interview Statistics.
References
- National Center for Health Statistics. Health, United States, 2012: With special feature on emergency care. Hyattsville, MD. 2013.
- Bloom B, Jones LI, Freeman G. Summary health statistics for U.S. children: National Health Interview Survey, 2012. National Center for Health Statistics. Vital Health Stat 10(258). 2013.
- Machlin SR. Expenses for a hospital emergency room visit, 2003. Rockville, MD: Agency for Healthcare Research and Quality. 2006.
- Pachter LM, Ludwig S, Groves A. Night people: Utilization of a pediatric emergency department during the late night. Pediatr Emerg Care 7(1):12–4. 1991.
- Gindi RM, Cohen RA, Kirzinger WK. Emergency room use among adults aged 18–64: Early release of estimates from the National Health Interview Survey, January–June 2011. National Center for Health Statistics. 2012.
- Parsons VL, Moriarity CL, Jonas K, et al. Design and estimation for the National Health Interview Survey, 2006–2015. National Center for Health Statistics. Vital Health Stat 2(165). 2014.
Suggested citation
Gindi RM, Jones LI. Reasons for emergency room use among U.S. children: National Health Interview Survey, 2012. NCHS data brief, no 160. Hyattsville, MD: National Center for Health Statistics. 2014.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Charles J. Rothwell, M.S., M.B.A., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health Interview Statistics
Jane F. Gentlemen, Ph.D., Director