Asthma Prevalence, Health Care Use and Mortality: United States, 2002
Please note this E-stat has been updated with 2003-2005 data, see the following report for more information:
Asthma is a chronic respiratory disease characterized by episodes or attacks of inflammation and narrowing of small airways in response to asthma “triggers.” Asthma attacks can vary from mild to life-threatening and involve shortness of breath, cough, wheezing, chest pain or tightness, or a combination of these symptoms. Many factors can trigger an asthma attack, including allergens, infections, exercise, abrupt changes in the weather, or exposure to airway irritants, such as tobacco smoke.
The burden from asthma in the United States has increased over the past 2 decades. Trends from 1980 to 1999 are presented in the CDC Asthma Surveillance Survey. This fact sheet presents the most recent national data on asthma gathered by the National Center for Health Statistics. Estimates for race/ethnicity and gender are age adjusted to the 2000 population standard to allow comparison of rates between groups.
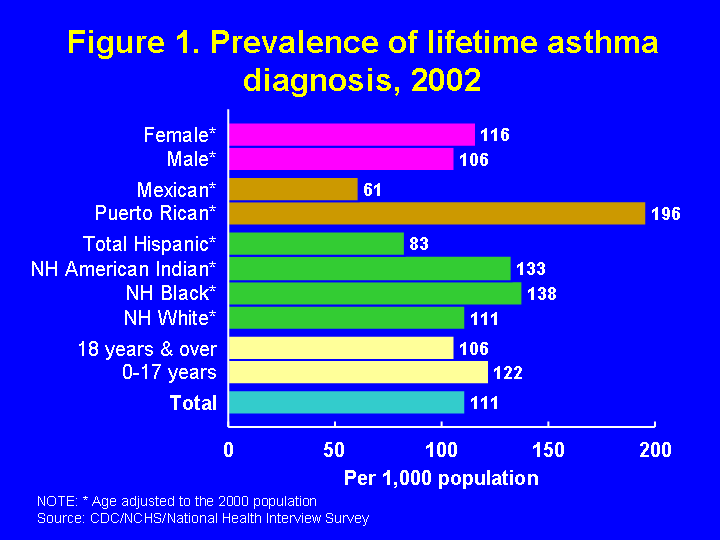
Prevalence, 2002: Lifetime asthma diagnosis, current asthma, and asthma attack prevalence
Respondents in the National Health Interview Survey are asked if they were ever told by a health professional that they had asthma. In 2002, 30.8 million people (111 people per 1,000) had ever been diagnosed with asthma during their lifetime (Figure 1). Among adults, 106 per 1,000 had a lifetime asthma diagnosis (21.9 million) compared to 122 per 1,000 children 0-17 years (8.9 million). Among all racial and ethnic groups, Puerto Ricans have the highest rate of lifetime asthma (196 per 1,000) and Mexicans the lowest (61 per 1,000). Grouping all Hispanics together masks this difference. Puerto Ricans were almost 80% more likely, and non-Hispanic blacks and American Indians were about 25% more likely to have ever been diagnosed with asthma than non-Hispanic whites. Females were about 7% more likely than males to ever have been diagnosed with asthma, but among children 0-17 years of age, males were more likely to have an asthma diagnosis, 139 per 1,000 versus 104 per 1,000 for females.
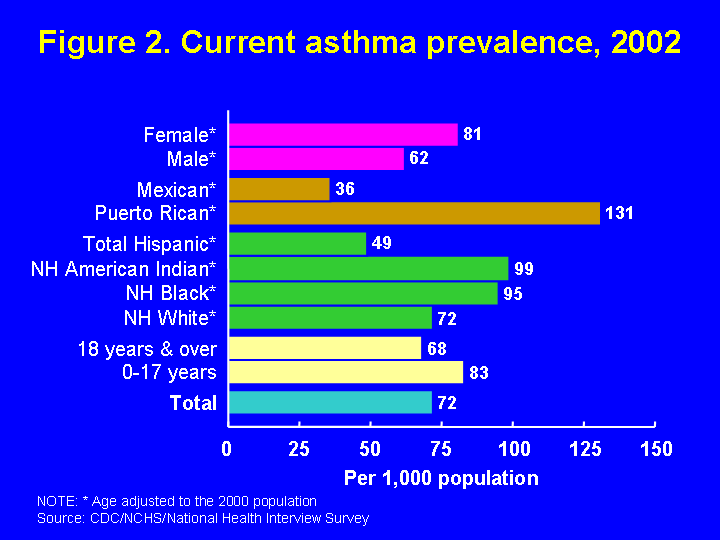
Estimates of current asthma prevalence include people who have been diagnosed with asthma by a health professional and who still have asthma. In 2002, 72 people per 1,000 or 20 million people, currently had asthma (Figure 2). Rates decreased with age; 83 per 1,000 children 0-17 years (6.1 million children) had asthma compared to 68 per 1,000 adults 18 years and over (14 million adults). When race/ethnicity is considered, Puerto Ricans had current asthma prevalence 80% higher than non-Hispanic whites, and non-Hispanic blacks and American Indians had current asthma prevalence 30% higher than non-Hispanic whites. The overall estimate for Hispanics masks the high prevalence among Puerto Ricans. Females had a 30% higher prevalence compared to males. However, this pattern was reversed among children. The current asthma prevalence rate for boys aged 0-17 years (94 per 1,000) was 30% higher than the rate among girls (71 per 1,000).
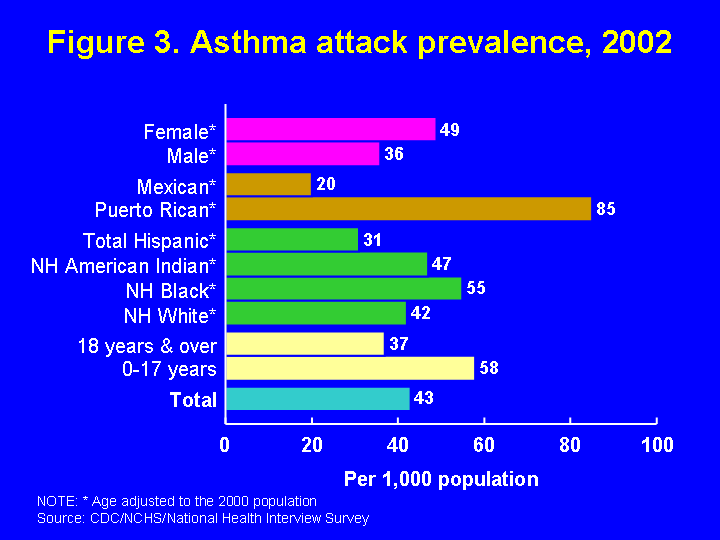
Asthma attack prevalence, or the number of people who had at least one asthma attack in the previous year, is a crude indicator of how many people have uncontrolled asthma and are at risk for a poor outcome, such as hospitalization. In 2002, 43 people per 1,000 (12 million people) had experienced an asthma attack in the previous year (Figure 3). That is, about 60% of the people who had asthma at the time of the survey had an asthma attack in the previous year. Asthma attack prevalence also decreased with age, 58 per 1,000 children 0-17 years (4.2 million children) had an asthma attack in the previous year compared to 37 per 1,000 adults aged 18 years and over (7.7 million adults). Puerto Ricans had the highest asthma attack prevalence, 100% higher than non-Hispanic whites while Non-Hispanic blacks had an asthma attack prevalence about 30% higher and American Indians about 10% higher than non-Hispanic whites. Mexicans had the lowest asthma attack prevalence. Females had about 35% higher prevalence than males. This pattern was reversed among children. The asthma attack prevalence rate for boys aged 0-17 years (68 per 1,000) was 45% higher than the rate among girls (47 per 1,000).
Missed school and work days, 2002
Asthma attacks interfere with daily activities, including attending school and going to work. Among those who reported at least one asthma attack in the previous year:
- Children 5-17 years of age missed 14.7 million school days due to asthma
- Adults 18 years of age and over who were currently employed missed 11.8 million work days due to asthma
Source: National Health Interview Survey, National Center for Health Statistics, CDC
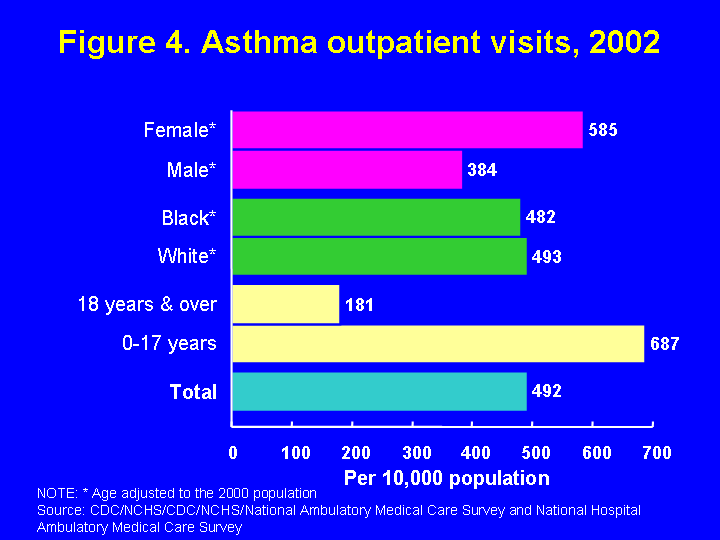
Health Care Use, 2002
Health care use for asthma includes outpatient visits to doctors’ offices and hospital outpatient departments, visits to hospital emergency departments (EDs), and hospitalizations. Information about Hispanic ethnicity is not consistently available in national health care utilization data, and therefore is not presented. In 2002, there were 13.9 million outpatient asthma visits to private physician offices and hospital outpatient departments, or 492 per 10,000 people (Figure 4). Children aged 0-17 years had 5 million visits and an outpatient visit rate of 687 per 10,000 and adults 18 years and older had a rate of 181 per 10,000. In contrast to other asthma measures shown here, blacks had an outpatient visit rate about the same as whites. Females had a 50% higher outpatient visit rate compared to males.
There were 1.9 million visits to EDs for asthma in 2002, or 67 per 10,000 people (Figure 5). Children aged 0-17 years had over 727,000 ED visits, a rate of 100 per 10,000. The ED visit rate was highest among children aged 0-4 years at 162 per 10,000. Adults 18 years and over had 24 ED visits per 10,000. The ED visit rate for blacks was 380% higher than that for whites, and for females, about 6% higher than for males.

There were 484,000 asthma hospitalizations in 2002, or 17 per 10,000 people (Figure 6). Among children 0-17 years, there were 196,000 hospitalizations (27 per 10,000). Hospitalizations were highest among children 0-4 years, 59 hospitalizations per 10,000. The asthma hospitalization rate for blacks was 225% higher than for whites. Females had a hospitalization rate about 35% higher than males.

Mortality
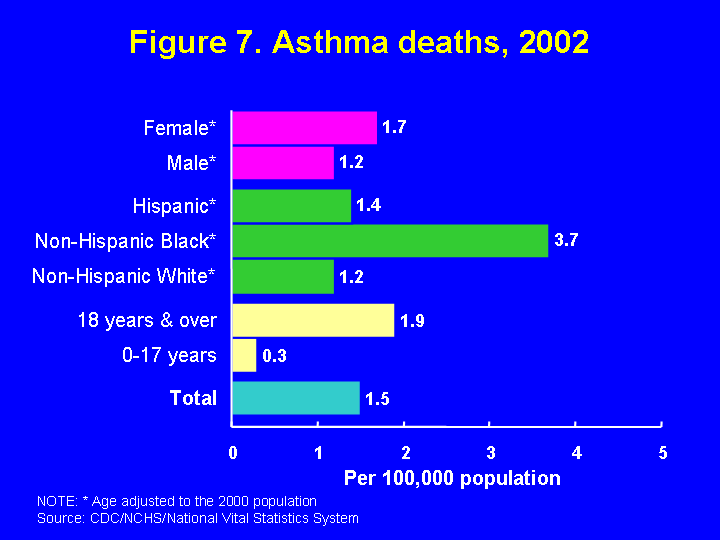
In 2002, 4,261 people died from asthma, or 1.5 per 100,000 people (Figure 7). Among children, asthma deaths are rare. In 2002, 187 children aged 0-17 years died from asthma, or 0.3 deaths per 100,000 children compared to 1.9 deaths per 100,000 adults aged 18 and over. Non-Hispanic blacks were the most likely to die from asthma, and had an asthma death rate over 200% higher than non-Hispanic whites and 160% higher than Hispanics. National estimates for Hispanic subgroups, such as Puerto Ricans and Mexicans, are not available. Females had an asthma death rate about 40% higher than males.
Data Sources
- Prevalence: National Health Interview Survey, NCHS, CDC
- Outpatient visits, emergency room visits: National Ambulatory Medical Care Survey and National Hospital Ambulatory Medical Care Survey, NCHS, CDC
- Hospitalizations: National Hospital Discharge Survey, NCHS, CDC
- Mortality: Mortality component of the National Vital Statistics System, NCHS, CDC
- U.S. Population to calculate health care utilization and mortality death rates: noninstitutionalized civilian population (ambulatory care rates), civilian population (hospitalization rates), and residential population (mortality rates): U.S. Bureau of the Census (revised February 20, 2004)
Sources of information
Data on asthma:
- State-level asthma data
- Surveillance for Asthma — United States, 1980–1999, Centers for Disease Control and Prevention
- Measuring Childhood Asthma Prevalence Before and After the 1997 Redesign of the National Health Interview Survey — United States, Centers for Disease Control and Prevention
- National Heart, Lung, and Blood Institute Morbidity and Mortality Chartbook
Economic and social costs:
- Weiss KB, Sullivan SD. The health economics of asthma and rhinitis. I. Assessing the economic impact. J Allergy Clin Immunol 2001;107:3-8.
Asthma management/medical professional and patient education:
- CDC’s Asthma Information
- National Asthma Education and Prevention Program Expert Panel Report 2: Guidelines for the Diagnosis and Management of Asthma
- What is Asthma?
- Action Against Asthma: A Strategic Plan for the Department of Health and Human Services
- About asthma management, American Lung Association