Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Public Health Strategies for Preventing and Controlling
Overweight and Obesity in School and Worksite Settings
A Report on Recommendations of the Task Force on Community
Preventive Services
Prepared by
David L. Katz, MD1,2
Meghan O'Connell, MPH1
Ming-Chin Yeh, PhD1,3
Haq Nawaz, MD1
Valentine Njike, MD1
Laurie M. Anderson, PhD4*
Stella Cory, MD5*
William Dietz, MD, PhD6*
1Yale Prevention Research Center, New Haven, Connecticut
2Yale University School of Medicine, New Haven, Connecticut
3Hunter College, City University of New York, New York, New York
4Division of Scientific Communications, National Center for Health Marketing, CDC
5Career Development Division, Office of Workforce and Career Development, CDC
6Division of Nutrition and Physical Activity, National Center for Chronic Disease Prevention and Health
Promotion, CDC
The material in this report originated in the National Center for Chronic Disease Prevention and Health Promotion, Janet Collins, PhD, Director; and
the Division of Nutrition and Physical Activity, William Dietz, MD, PhD, Director.
Corresponding preparer: Laurie M. Anderson, PhD, Health Scientist, Scientific Information and Dissemination Branch, CDC/NCHM/DSC,
4770 Buford Highway, MS K-95, Atlanta, GA 30341; Telephone: 360-236-4274; Fax: 360-236-4245; E-mail:
laa1@cdc.gov.
Summary
Reducing morbidity and mortality related to overweight and obesity is a public health priority. Various interventions
in school and worksite settings aim to maintain or achieve healthy weight. To identify effective strategies for weight control
that can be implemented in these settings, the Task Force on Community Preventive Services (Task Force) has conducted
systematic reviews of the evidence on nutrition, physical activity, combinations of these interventions, and other behavioral
interventions (e.g., cognitive techniques such as self-awareness and cue recognition).
Task Force recommendations are based on evidence of effectiveness, which is defined in this report as achieving a
mean weight loss of >4 pounds, measured
>6 months after initiation of the intervention program. The Task Force
recommends multicomponent interventions that include nutrition and physical activity (including strategies such as providing
nutrition education or dietary prescription, physical activity prescription or group activity, and behavioral skills development
and training) to control overweight and obesity among adults in worksite settings. The Task Force determined that
insufficient evidence existed to determine the effectiveness of combination nutrition and physical activity interventions to prevent or
reduce overweight and obesity in school settings because of the limited number of qualifying studies reporting
noncomparable outcomes. This report describes the methods used in these systematic reviews; provides additional information regarding
these recommendations; and cites sources for full reviews containing details regarding applicability, other benefits and
harms, barriers to implementation, research gaps, and economic data (when available) regarding interventions.
Background
On the basis of conservative estimates, 65% of adults are overweight or obese
(1), a relative increase of 61% during
1991--2000 (2). Despite a conservative definition of overweight in children based on the 95th percentile for age- and
sex-adjusted body mass index (BMI), a measure intended to be more specific than sensitive,
>16% of children aged 6--19 years in the
U.S. population are considered overweight
(1--3). Overall, the prevalence of childhood overweight has tripled over the previous
2 decades (4), and the prevalence of overweight among certain ethnic minority groups is even higher. Approximately 22%
of Mexican American children aged 6--19 years are overweight, and for non-Hispanic black children aged 6--19
years,
approximately 21% are overweight (3).A study of a limitednumber of American Indian children indicated that 30%
were overweight (5).
Obesity is associated with increased risk for cardiovascular disease; diabetes;
certainforms of cancer, depression, discrimination and weight-related bias; and various other physical, psychological, and social morbidities
(6--9). A linear relation was reported between BMI and mortality risk based on an observational cohort of approximately 1 million
persons followed for 14 years (10). In the Nurses' Health Study, a linear relation was reported between BMI and mortality risk
among women; the lowest risk for all-cause mortality occurred among women with a BMI 15% below average with stable weight
over time (11). An analysis of National Health and Nutrition Examination Survey (NHANES) data
(12) indicated that, relative to being normal weight (BMI 18.5 to <25.0), being obese (BMI
>30.0) resulted in excess deaths in the United States in
2000, primarily among persons with a BMI
>35.0. The same analysis reported excess deaths among underweight (BMI
<18.5) persons, but overweight (BMI 25.0 to <30.0) was not associated with excess mortality
(12).
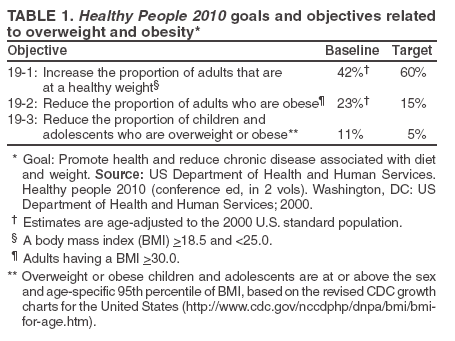
Healthy People 2010 objectives pertinent to overweight and obesity prevention and control have been documented
(Table 1) (13). Interventions in school and worksite settings to reduce overweight and obesity might affect multiple objectives.
School and worksite settings are both locations where children or adults spend substantial time, and these settings
provide ample opportunities for nutrition and physical activity interventions. A substantial proportion of daily calories are
consumed in these settings, and both sites frequently have existing facilities that can support regular physical activity among students
and employees, potentially reducing obesity and overweight in addition to providing other benefits.
School sites offer multiple advantages for implementation of efforts to prevent and control overweight by
affording continuous and intensive contact with the majority of children and adolescents in the United States
(14). School programs can capitalize on existing (although often constrained)
resources and tools to develop student knowledge, attitudes, and
skills essential for healthy lifestyles. School curricula, personnel, policy interventions, and changes in the physical
environment (e.g., making healthier choices available in cafeterias and vending machines) have the potential to promote healthful
dietary practices and regular physical activity
(15). Guide to Community Preventive Services (Community
Guide) recommendations for increasing physical activity include
recommendations applicable to schools (16).
Worksites provide access to 65% of the population aged
>16 years (17), which makes them ideal settings to
implement strategies for reducing the prevalence and burden of overweight and obesity. Similar
toschools, worksites allow access to employees in a controlled environment through
existing channels of communication and social support
networks. Opportunities for environmental and policy change to foster healthy dietary practices and increase activity
(18) are readily available. For example, worksites can provide easier access to stairwells than to elevators and adopt policies that
provide employees with exercise breaks during working hours. The incentive for ongoing support of weight maintenance and
other health promoting activities in worksites is substantial, given that such programs might translate into cost savings for
employers (19,20).
Introduction
The Task Force on Community Preventive Services (Task Force) leads work on the
Community Guide, a resource that includes multiple systematic reviews, each focusing on a public health topic.
Community Guide development is supported by the U.S. Department of Health and Human Services (DHHS) in collaboration with public and private partners.
Although CDC provides staff support to the Task Force for development of the
Community Guide, the recommendations presented
in this report were developed by the Task Force and are not necessarily the recommendations of DHHS or CDC.
This report is one in the series of systematic reviews developed for the
Community Guide; it provides an overview of
the process used by the Task Force to select and review evidence and summarizes recommendations regarding interventions
to prevent or control overweight and obesity. This report provides guidance to state and local health departments, state and
local education agencies and school systems, government policymakers, employers, and others interested in or responsible
for reducing the prevalence of overweight and obesity. A full report on the recommendations (including discussions
of applicability; additional benefits; potential harms; existing barriers to implementation; costs, cost benefit, and
cost effectiveness of the interventions; and remaining research questions) and additional information concerning the
review findings are scheduled for publication on the
Community Guide website
(http://www.thecommunityguide.org).The report
will include interventions in community and health-care system settings and those in school and worksite settings.
The review of the evidence on effectiveness of community approaches to reducing overweight and obesity in school
and worksite settings complements reviews by the U.S. Preventive Services Task Force and the
Guide to Clinical Preventive Services (Clinical
Guide). The Clinical Guide provides information on 1) screening and interventions for childhood
overweight (21), 2) effectiveness of routine counseling to
promote physical activity in primary care settings
(22), 3) behavioral counseling to promote a healthy diet
(23), and 4) screening and counseling of adults for obesity and overweight
(24). Detailed information regarding the
Clinical Guide is available (http://www.ahrq.gov). Both the
Clinical Guide and the Community
Guide present evidence on effectiveness for options for weight control across primary care and community settings.
Additional information regarding the Task Force and the
Community Guide and links to published reports
are available (http://www.thecommunityguide.org).
Methods
The methods used by the Community Guide for conducting systematic reviews and linking evidence to
recommendations have been described (25). As with each review, a multidisciplinary systematic review development team (review team),
with support from a consultation team,†
conducts a review consisting of the following steps:
developing a conceptual approach to organize, group, and select the interventions;
systematically searching for and retrieving evidence;
assessing the quality of and summarizing the strength of evidence of effectiveness;
assessing cost and cost-effectiveness data (when available) for recommended interventions;
identifying issues of applicability and barriers to implementation (when available) for recommended interventions;
summarizing information regarding other benefits or harms potentially resulting from the intervention; and
identifying and summarizing research gaps.
For each setting in which a review of interventions to
prevent overweight and obesity was completed, the review
team developed an analytic framework to indicate the relation of interventions to relevant intermediate outcomes (e.g.,
knowledge, attitudes, and beliefs), diet- and physical activity-related behaviors, and the relations between improvements in
dietary consumption and physical activity and weight
control. In this review, the review team considered only
weight-related variables as recommendation outcome measures, indicating intermediate outcomes (e.g., change in diet or physical activity levels) in
the analytic framework for their explicative value. In the school setting, determination of a meaningful weight change in studies
of children was assessed based on the intervention goal and study population characteristics on a study-by-study basis.
Among adults in worksite settings, a 4-pound minimum weight loss standard was used as a measure of success, based on
expert consensus and supporting studies indicating that modest weight loss is associated with improvements in lipid profiles
(26), metabolic syndrome (27), and hypertension
(28) and might be of particular benefit to persons with visceral overweight
or obesity (i.e., deposition of fat in vital organs, especially the liver).
To be considered for inclusion in the reviews of effectiveness, studies had to include multiple characteristics.
Description of a primary intervention with participants recruited or enrolled from the school (including preschool)
or worksite setting.
Publication in English during 1966--2001.
Interventions related to diet, physical activity, or combinations thereof, with sufficient detail to meet
Community Guide standards.
Common weight-related measures as outcomes (e.g., BMI, body weight, and anthropometric measures).
Control measurement between or within groups (either with baseline and follow-up [before and after] measurements
or by using control groups).
Subjects followed for at least 6 months from the beginning of the intervention to assess weight loss maintenance (Box).
To identify additional studies, manual searches were performed of reference lists from identified reports, extant
systematic reviews (certain reviews available through the Cochrane Library), review reports, and reports written by researchers in
the field.
Each candidate study was evaluated by two independent reviewers by using a standardized abstraction form and
was assessed for suitability of study design and threats to validity. Study designs were characterized as greatest, moderate, or
least
suitable, based on the number of quality limitations, and study execution was characterized as good, fair, or limited, based
on the number of threats to validity (29).
Effect sizes for each outcome of interest were obtained from all studies meeting the minimum quality criteria
(qualifying studies). Net effects were derived, when appropriate, by calculating the difference between the changes observed in
the intervention and comparison groups relative to the respective baseline levels. Individual effect sizes were calculated as
follows:
For studies with before-and-after measurements of weight in intervention and concurrent comparison groups,
effect size = Δ I -- Δ C
For studies with post measurements of weight only in
intervention and comparison groups, effect size = Ipost -- Cpost,
where Ipost = intervention group post measurement and
Cpost = the control group post measurement.
For studies with before-and-after measurements of weight, with no comparison group, effect size = Ipost -- Ipre,
where Ipost = the intervention group post measurement and
Ipre = the intervention group baseline measure.
Where study outcomes were reported in comparable metrics (e.g., BMI or weight in pounds), effect sizes were plotted
on graphs and pooled effects were calculated. Pooled
effect size = Σ(individual effect size*n)/N, where n = sample size
of individual study and N = sum of n of all individual studies included in the analysis.
The Task Force uses systematic reviews to evaluate the evidence of intervention effectiveness and makes
recommendations based on the findings of the reviews. The strength of each recommendation is based on the evidence of effectiveness (i.e.,
an intervention is recommended on the basis of either
strong or sufficient evidence of effectiveness)
(25). Other types of evidence can also affect a recommendation. For
example, harms resulting from an intervention that outweigh benefits might lead to
a recommendation that the intervention not be used, even if it is effective in improving certain outcomes.
A finding of insufficient evidence to determine effectiveness means that the review team was not able to determine
whether the intervention was effective. This finding is critical to identify areas of uncertainty and continuing research needs.
In contrast, sufficient or strong evidence of ineffectiveness
would lead to a recommendation against use of the intervention.
Results
The Task Force findings in this report were based on the systematic review and evaluation of qualifying studies, all of
which had good or fair quality of execution. In the worksite studies, effectiveness was defined as achievement of a mean weight loss
of >4 pounds across studies (pooled effect size) measured at
>6 months into the intervention
program. Among growing children in school settings, no single standard for meaningful weight loss exists because a successful intervention might be one
that prevents weight gain, allowing children to normalize their BMI by growing into their weight (i.e., getting taller
without adding weight). Therefore, determination of a meaningful weight change in studies of children was assessed in relation to
the intervention goal and study population characteristics on a study-by-study basis.
Interventions for Preventing and Controlling Overweight and Obesity in
School Settings
From the initial search for interventions in the school setting, 44 studies were considered
(30--73); of these studies, six did not meet inclusion criteria
(31,46,47,52,67,71). The remaining 38 candidate studies were retained for full review; of
these studies, 28
(30,33--43,45,49,51,54,56,58--60,62,64,66,68--70,72,73
) were excluded on the basis of methodologic limitations.
The remaining 10 studies were considered qualifying studies and form the basis of the Task Force findings
reported (32,44,48,50,53,55,57,61,63,65).
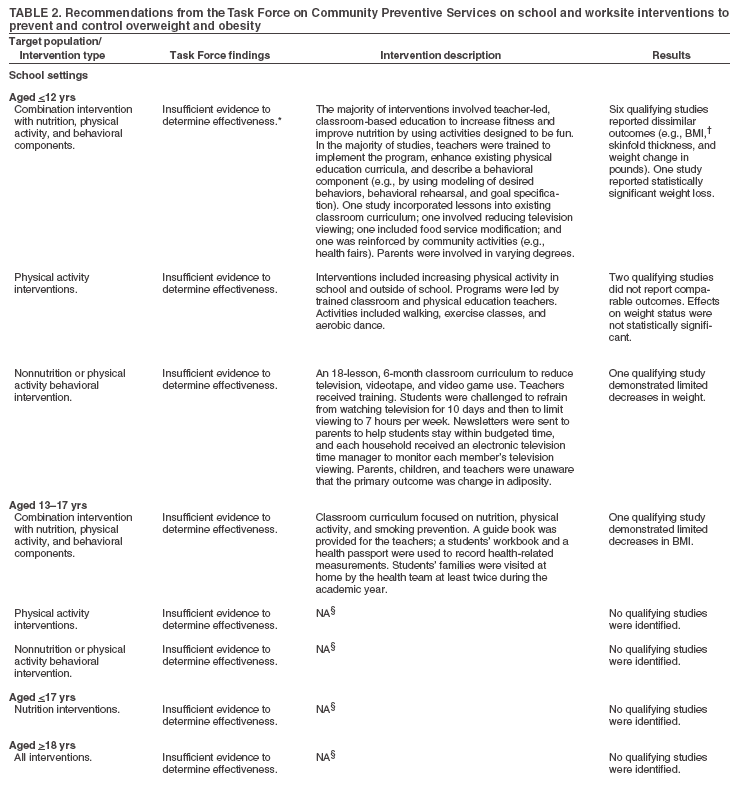
The Task Force determined that insufficient evidence
existed to determine the effectiveness of all reviewed
interventions in school settings among children and adolescents: combinations of nutrition and physical
activity, physical activity interventions alone, nutrition interventions alone, and behavioral interventions with or without a nutrition or physical activity focus.
The most frequent reasons for insufficient evidence were that no studies or only a limited number of studies with
comparable outcomes were identified (Table 2). No studies of interventions conducted among college students were identified (Table 2).
Interventions for Preventing and Controlling Overweight and Obesity in
Worksite Settings
From the initial search, 35 studies of interventions in the worksite setting were considered
(74--108); four studies did not meet inclusion criteria
(79,80,91,99); and the remaining 31 candidate studies were retained for full review. Of these
studies, 11 were excluded because of quality limitations
(75,76,78,82,86,93,94,96,104,105,107); the remaining 20 were
considered qualifying studies (74,77,81,83--85,87--90,92,95,97,98,100--103,106,108
).
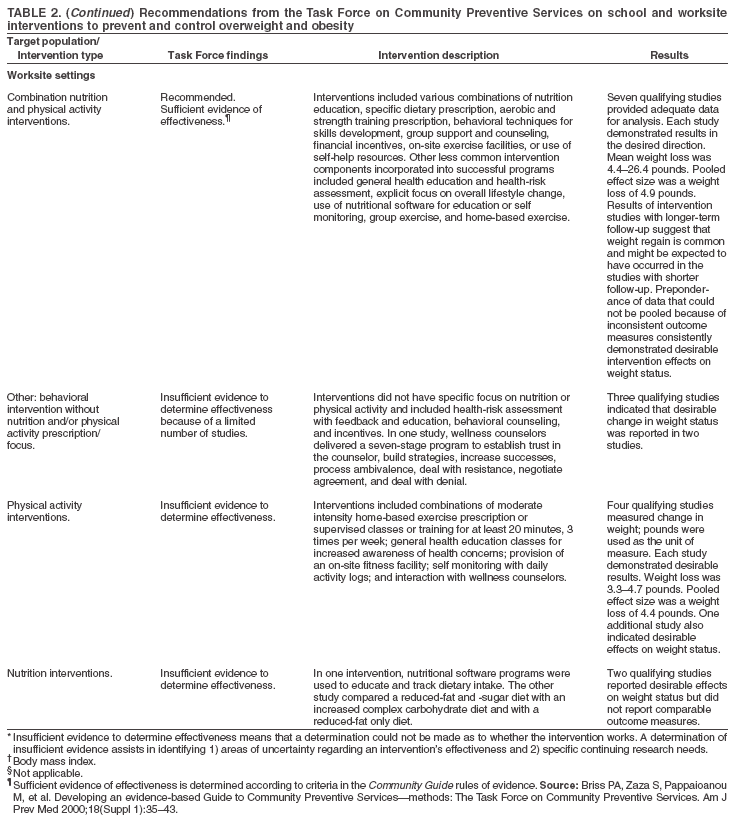
On the basis of sufficient evidence from seven studies
(74,81,85,95,101,106,108) with comparable outcomes, the
Task Force recommended worksite interventions in which nutrition and physical activity to control overweight or
obesity were combined. Frequently, employed intervention strategies were didactic nutrition education
(81,85,95,101, 106,108), aerobic or strength training exercise prescription
(74,81,85,95), training in behavioral techniques
(81,85,95,106,108), providing self-directed materials
(74,85,95), specific dietary prescription
(74), and group or supervised exercise
(101,106,108).
Two studies that met the quality criteria for a
Community Guide economic review provided cost-effectiveness analyses
of worksite interventions to prevent and control overweight and obesity
(80,109). On the basis of the findings of these
two studies, the cost is <$1 per employee per year to engage 1% of the population at risk in onsite programs for weight loss.
The Task Force determined that insufficient evidence
existed to determine the effectiveness of single-component
worksite interventions focused on nutrition, physical activity, or other behavioral intervention among adults. This determination
was made because of a limited number of studies with comparable outcomes (Table 2). Summary tables of studies in these
reviews are scheduled to be available on the Community
Guide website (http://www.thecommunityguide.org/obese) in 2006.
Conclusions and Use of Recommendations
Employing components of each category of intervention evaluated (physical activity, nutrition, combinations of the
two, and other behavioral interventions) might contribute to
reducing the prevalence of overweight and obesity and
subsequentobesity-related morbidity and mortality. Because the multiple components of the studies on which recommendations
have been based could not be evaluated separately, the effects of specific intervention components could not be
determined.
School-Based Interventions
In the literature search for the review of school-based interventions, an insufficient number of studies (according
to Community Guide rules of evidence) were identified that had methodologic quality on which to base recommendations.
The literature used for this review included studies initiated before the age- and sex-adjusted BMI standards for children
(currently the gold standard) were established in the late 1990s. In addition, in these qualifying studies, various outcome measures
were used; therefore, comparisons across studies were hampered.
Barriers to school-based overweight and obesity intervention research pose formidable challenges. The stigma attached
to overweight makes the assessment of weight among children a difficult concern for school officials and parents and
raises ethical concerns regarding the potential stigmatization of
children.
When planning future interventions aimed at weight control outcomes, considering interventions that produced modest
but positive changes in weight-related measures might be useful. These interventions are 1) including nutrition and
physical activity components in combination
(32,44,48,53,61,65,67); 2) allotting additional time to physical activity during
the school day (32,50,57); 3) including noncompetitive sports (e.g., dance)
(50); and 4) reducing sedentary activities,
especially television viewing (44,55).
Internet use and playing video games seem conceptually similar and worth addressing in future evaluations. Further
research regarding the value of college- and university-based interventions, involving parents in school-based interventions, and
the effect of school environmental and policy changes on weight-related outcomes are all warranted.
Worksite-Based Interventions
The Task Force recommends combination nutrition and physical activity programs. The literature supports an emphasis
on interventions combining instruction in healthier eating with a structured approach to increasing physical activity in
the worksite setting. Evidence of effectiveness of workplace efforts to control overweight and obesity
mightencourage employers to
provide such programs. Program cost-effectiveness data might also increase employer interest. Reviews of cost effectiveness
of these interventions to reduce overweight and obesity are available on the
Community Guide website (http://www.thecommunityguide.org/obese).
Studies of primary obesity prevention are lacking. Research needs to be conducted to determine the effect of
weight-related outcomes of worksite-based environmental change (e.g., making stairs more accessible and modifying the
nutritional environment by providing easy, ubiquitous access to affordable, healthful foods). Creative worksite interventions coupled
with other interventions (e.g., weight loss programs in community supermarkets or recreational facilities and providing
pedestrian or bicycling alternatives to driving) warrant study. Worksite interventions directed toward adolescents alone or in concert
with adults, in worksites where both can be targeted
(e.g., supermarkets and other retail outlets), also
warrant study.
The definition of effectiveness was based exclusively on achievement of weight loss; therefore,
certainstudies in the review might have resulted in positive change in other outcomes (e.g., dietary intake and exercise) not included in this report. A
4-pound minimum weight loss standard was used as a measure of success; however, evidence is lacking to determine
categorically how much weight loss over what period yields the greatest health benefit. Finally, given the frequency of weight rebound
after short-term weight loss, additional research is needed regarding the most effective means of maintaining initial success.
Certain effective strategies for preventing and controlling overweight and obesity over the short-term have been
identified for worksite settings; interventions in school-settings
require further evaluation. New data on interventions in
scientific literature since 2001 are scheduled to be included in periodic updates to these systematic reviews. Multiple
additional programmatic, policy, and research efforts are needed to control and reverse obesity trends and achieve the healthy
weight goals of Healthy People 2010
(13).
References
Flegal KM, Carroll MD, Ogden CL, Johnson CL. Prevalence and trends in obesity among U.S. adults, 1999--2000. JAMA 2002;288:1723--7.
Mokdad AH, Bowman BA, Ford ES, Vinicor F, Marks JS, Koplan JP. The continuing epidemics of obesity and diabetes in the United States.
JAMA 2001;286:1195--200.
Hedley AA, Ogden CL, Johnson CL, Carroll MD, Curtin LR, Flegal KM. Prevalence of overweight and obesity among US children,
adolescents, and adults, 1999--2002. JAMA 2004;291:2847--50.
Ogden CL, Carroll MD, Flegal KM. Epidemiologic trends in overweight and obesity. Endocrinol Metab Clin North Am 2003;32: 741--60,vii.
Caballero B, Himes JH, Lohman T, et al. Body composition and overweight prevalence in 1704 schoolchildren from 7 American
Indian communities. Am J Clin Nutr 2003;78:308--12.
Chambliss HO, Finley CE, Blair SN. Attitudes toward obese individuals among exercise science students. Med Sci Sports Exerc 2004;36:468--74.
Dixon JB, Dixon ME, O'Brien PE. Depression in association with severe obesity: changes with weight loss. Arch Intern Med 2003;163:2058--65.
Pi-Sunyer FX. Comorbidities of overweight and obesity: current
evidence and research issues. Med Sci Sports Exerc 1999;31 (Suppl 11):S602--8.
Puhl RM, Brownell KD. Psychosocial origins of obesity stigma:
toward changing a powerful and pervasive bias. Obes Rev 2003;4: 213--27.
Calle EE, Thun MJ, Petrelli JM, Rodriguez C, Heath CW Jr. Body-mass index and mortality in a prospective cohort of U.S. adults.
N Engl J Med 1999;341:1140--1.
Manson JE, Willett WC, Stampfer MJ, et al. Body weight and mortality among women. N Engl J Med 1995;333:677--85.
Flegal KM, Graubard BI, Williamson DF, Gail MH. Excess deaths associated with underweight, overweight, and obesity. JAMA 2005;293:1861--7.
US Department of Health and Human Services. Healthy people 2010
(conference ed, in 2 vols). Washington, DC: US Department of Health
and Human Services; 2000.
Baranowski T, Cullen KW, Niklas T, Thompson D, Baranowski J. School-based obesity prevention: a blueprint for taming the epidemic. Am
J Health Behav 2002;26:486--93.
Dietz WH, Gortmaker SL. Preventing obesity in children and adolescents. Annu Rev Public Health 2001;22:337--53.
Kahn EB, Ramsey LT, Brownson RC, et al. The effectiveness of interventions to increase physical activity: a systematic review. Am J Prev
Med 2002;22(Suppl 4):73--107.
Catlin TK, Simoes EJ, Brownson RC. Environmental and policy factors associated with overweight among adults in Missouri. Am J Health
Promot 2003;17:249--58.
Aldana SG. Financial impact of health promotion programs: a
comprehensive review of the literature. Am J Health Promot 2001;15:296--320.
Goetzel RZ, Jacobson BH, Aldana SG, Vardell K, Yee L. Health care costs of worksite health promotion participants and non-participants. J
Occup Environ Med 1998;40:341--6.
Whitlock EP, Williams SB, Gold R, Smith PR, Shipman SA. Screening and interventions for childhood overweight: a summary of evidence for
the US Preventive Services Task Force. Pediatrics 2005;116:e125--44.
US Preventive Services Task Force. Physical activity counseling. Rockville, MD: US Department of Health and Human Services, Agency
for Healthcare Research and Quality, US Preventive Services Task Force; 2002. Available at
http://www.ahrq.gov/clinic/uspstf/uspsphys.htm.
US Preventive Services Task Force. Healthy diet counseling. Rockville, MD: US Department of Health and Human Services, Agency for
Healthcare Research and Quality, US Preventive Services Task Force; 2003. Available at
http://www.ahrq.gov/clinic/uspstf/uspsdiet.htm.
US Preventive Services Task Force. Screening for obesity in adults. Rockville, MD: US Department of Health and Human Services, Agency
for Healthcare Research and Quality, US Preventive Services Task Force; 2003. Available at
http://www.ahrq.gov/clinic/3rduspstf/obesity/obeswh.pdf.
Briss PA, Zaza S, Pappaioanou M, et al. Developing an evidence-based Guide to Community Preventive Services---methods: The Task Force
on Community Preventive Services. Am J Prev Med 2000;18 (Suppl 1):35--43.
Dattilo AM, Kris-Etherton PM. Effects of weight reduction on blood
lipids and lipoproteins: a meta-analysis. Am J Clin Nutr 1992;56:320--8.
Bussetto L. Visceral obesity and the metabolic syndrome: effects of weight loss. Nutr Metab Cardiovasc Dis 2001;11:195--204.
Stevens VJ, Obarzanek E, Cook NR, et al. Long-term weight loss and changes in blood pressure: results of the Trials of Hypertension
Prevention, phase II. Ann Intern Med 2001;134:1--11.
Zaza S, Wright-De Aguero LK, Briss PA, et al. Data collection instrument and procedure for systematic reviews in the Guide to
Community Preventive Services. Task Force on Community Preventive Services. Am J Prev Med 2000;18(Suppl 1):44--74.
Angelico F, Del Ben M, Fabiani L, Pannozzo F, Urbanati GC, Ricci G. Management of childhood obesity through a school-based programme
of general health and nutrition education. Public Health 1991;105:393--8.
Balch P, Balch K. Establishing a campus-wide behavioral weight
reduction program through a university student health service: the use and
training of health service personnel as behavioral weight
therapists. J Am Coll Health Assoc 1976;25:148--52.
Burke V, Milligan RA, Thompson C, et al. A controlled trial of health promotion programs in 11-year-olds using physical activity "enrichment"
for higher risk children. J Pediatr 1998;132:840--8.
Bush PJ, Zuckerman AE, Theiss PK, Taggart VS, Horowitz C, Sheridan MJ. Cardiovascular risk factor prevention in black schoolchildren:
two-year results of the "Know Your Body" program. Am J Epidemiol 1989;129:466--82.
Bush PJ, Zuckerman AE, Taggart VS, Theiss PK, Peleg EO, Smith SA. Cardiovascular risk factor prevention in black school children: the
"Know Your Body" evaluation project. Health Educ Q 1989;16:215--27.
Christakis G, Sajecki S, Hillman RW, Miller E, Blumenthal S, Archer M. Effect of a combined nutrition education and physical fitness program
on the weight status of obese high school boys. Fed Proc 1966;25:15--9.
Davis S, Gomez Y, Lambert L, Skipper B. Primary prevention of
obesity in American Indian children. Ann N Y Acad Sci 1993;699: 167--80.
DeWolfe JA, Jack E. Weight control in adolescent girls: a comparison of the effectiveness of three approaches to follow-up. J Sch
Health 1984;54:347--9.
Donnelly JE, Jacobsen DJ, Whatley JE, et al. Nutrition and physical activity program to attenuate obesity and promote physical and
metabolic fitness in elementary school children. Obes Res 1996;4:229--43.
Dwyer T, Coonan WE, Leitch DR, Hetzel BS, Baghurst RA. An
investigation of the effects of daily physical activity on the health of primary
school students in South Australia. Int J Epidemiol 1983;12:308--13.
Epstein L, Masek B, Marshall W. A nutritionally based school
program for control of eating in obese children. Behav Ther 1978;9:766--78.
Flores R. Dance for health: improving fitness in African American and Hispanic adolescents. Public Health Rep 1995;110:189--93.
Foster GD, Wadden TA, Brownell KD. Peer-led program for the treatment and prevention of obesity in the schools. J Consult Clin
Psychol 1985;53:538--40.
Goldberg SJ, Allen HD, Friedman G, Meredith K, Tymrack M, Owen AY. Use of health education and attempted dietary change to
modify atherosclerotic risk factors: a controlled trial. Am J Clin Nutr 1980;33:1272--8.
Gortmaker SL, Peterson K, Wiecha J, et al. Reducing obesity via a school-based interdisciplinary intervention among youth: Planet Health.
Arch Pediatr Adolesc Med 1999;153:409--18.
Howard JK, Bindler RM, Synoground G, van Gemert FC. A cardiovascular risk reduction program for the classroom. J Sch Nurs 1996;12:4--11.
Killen JD, Telch MJ, Robinson TN, Maccoby N, Taylor CB, Farquhar JW. Cardiovascular disease risk reduction for tenth graders. A
multiple-factor school-based approach. JAMA 1988;260:1728--33.
Killen JD, Robinson TN, Telch MJ, et al. The Stanford Adolescent Heart Health Program. Health Educ Q 1989;16:263--83.
Lionis C, Kafatos A, Vlachonikolis J, Vakaki M, Tzortzi M, Petraki A. The effects of a health education intervention program among
Cretan adolescents. Prev Med 1991;20:685--99.
Luepker RV, Perry CL, McKinlay SM, et al. Outcomes of a field trial to improve children's dietary patterns and physical activity. The Child
and Adolescent Trial for Cardiovascular Health. CATCH collaborative group. JAMA 1996;275:768--76.
Mo-suwan L, Pongprapai S, Junjana C, Puetpaiboon A. Effects of a controlled trial of a school-based exercise program on the obesity
indexes of preschool children. Am J Clin Nutr 1998;68:1006--11.
Musgrave KO, Thornbury ME. Weight control program for university students conducted by nutrition seniors. J Am Diet Assoc 1976;68:462--6.
Nader PR, Sallis JF, Patterson TL, et al. A family approach to cardiovascular risk reduction: results from the San Diego Family Health Project.
Health Educ Q 1989;16:229--44.
Nader PR, Stone EJ, Lytle LA, et al. Three-year maintenance of
improved diet and physical activity: the CATCH cohort. Child and Adolescent
Trial for Cardiovascular Health. Arch Pediatr Adolesc Med 1999;153:695--704.
Resnicow K, Cohn L, Reinhardt J, et al. A three-year evaluation of the Know Your Body program in inner-city schoolchildren. Health Educ
Q 1992;19:463--80.
Robinson TN. Reducing children's television viewing to prevent
obesity: a randomized controlled trial. JAMA 1999;282:1561--7.
Rotatori AF, Switzky H. A successful behavioral weight-loss program for moderately-retarded teenagers. Int J Obes 1979;3:223--8.
Sallis JF, McKenzie TL, Alcaraz JE, Kolody B, Hovell MF, Nader PR. Project SPARK. Effects of physical education on adiposity in children. Ann
N Y Acad Sci 1993;699:127--36.
Sasaki J, Shindo M, Tanaka H, Ando M, Arakawa K. A long-term aerobic exercise program decreases the obesity index and increases the high
density lipoprotein cholesterol concentration in obese children. Int J Obes 1987;11:339--45.
Seltzer CC, Mayer J. An effective weight control program in a public school system. Am J Public Health Nations Health 1970;60:679--89.
Simonetti D'Arca A, Tarsitani G, Cairella M, et al. Prevention of
obesity in elementary and nursery school children. Public Health
1986;100:166--73.
Tamir D, Feurstein A, Brunner S, Halfon ST, Reshef A, Palti H. Primary prevention of cardiovascular diseases in childhood: changes in serum
total cholesterol, high density lipoprotein, and body mass index after 2 years of intervention in Jerusalem schoolchildren age 7--9 years. Prev
Med 1990;19:22--30.
Vandongen R, Jenner DA, Thompson C, et al. A controlled evaluation of a fitness and nutrition intervention program on cardiovascular health
in 10- to 12-year-old children. Prev Med 1995;24:9--22.
Walter HJ, Hofman A, Connelly PA, Barrett LT, Kost KL. Primary prevention of chronic disease in childhood: changes in risk factors
after one year of intervention. Am J Epidemiol 1985;122:772--81.
Walter HJ, Hofman A, Connelly PA, Barrett LT, Kost KL. Coronary heart disease prevention in childhood: one-year results of a
randomized intervention study. Am J Prev Med 1986;2:239--45.
Walter HJ, Hofman A, Vaughan RD, Wynder EL. Modification of risk factors for coronary heart disease. Five-year results of a
school-based intervention trial. N Engl J Med 1988;318:1093--100.
Walter HJ, Wynder EL. The development, implementation, evaluation, and future directions of a chronic disease prevention program for
children: the "Know Your Body" studies. Prev Med 1989;18:59--71.
Walter HJ. Primary prevention of chronic disease among children: the school-based "Know Your Body" intervention trials. Health Educ
Q 1989;16:201--14.
Webber LS, Osganian SK, Feldman HA, et al. Cardiovascular risk factors among children after a 2 1/2-year intervention---The CATCH Study.
Prev Med 1996;25:432--41.
Weber MD, Johnson CA, Carter S, et al. Project SMART parent program: preliminary results of a chronic disease risk reduction trail. Ann
Med 1989;21:231--3.
Williams CL, Arnold CB. Teaching children self-care for chronic disease prevention: obesity reduction and smoking prevention. Patient Couns Health Educ 1980;2:92--8.
Williams CL. Prevention and treatment of childhood obesity in a public school setting. Pediatr Ann 1984;13:482--90.
Wong ML, Koh D, Lee MH, Fong YY. Two-year follow-up of a behavioural weight control programme for adolescents in Singapore: predictors
of long-term weight loss. Ann Acad Med Singapore 1997;26:147--53.
Zakus G, Chin ML, Cooper H Jr, Makovsky E, Merrill C. Treating adolescent obesity: a pilot project in a school. J Sch Health 1981; 51:663--6.
Research Group of the Rome Project of Coronary Heart Disease Prevention. Eight-year follow-up results from the Rome Project of Coronary
Heart Disease Prevention: Research Group of the Rome Project of Coronary Heart Disease Prevention. Prev Med 1986;15:176--91.
Abrams DB, Follick MJ. Behavioral weight-loss intervention at the worksite: feasibility and maintenance. J Consult Clin Psychol 1983; 51:226--33.
Aldana SG, Jacobson BH, Harris CJ, Kelley PL. Mobile work site health promotion programs can reduce selected employee health risks. J
Occup Med 1993;35:922--8.
Aldana SG, Jacobson BH, Kelley PL, Quirk M. The effectiveness of a mobile worksite health promotion program in lowering employee health
risk. Am J Health Promot 1994;8:254--6.
Bjurstrom LA, Alexiou NG. A program of heart disease intervention
for public employees: a five year report. J Occup Med 1978;20:521--31.
Breslow L, Fielding J, Herrman AA, Wilbur CS. Worksite health promotion: its evolution and the Johnson & Johnson experience. Prev
Med 1990;19:13--21.
Brownell KD, Cohen RY, Stunkard AJ, Felix MR, Cooley NB. Weight loss competitions at the work site: impact on weight, morale and
cost-effectiveness. Am J Public Health 1984;74:1283--5.
Brownell KD, Stunkard AJ, McKeon PE. Weight reduction at the work site: a promise partially fulfilled. Am J Psychiatry 1985;142:47--52.
DeBacker G, Kornitzer M, Dramaix M, et al. Risk factor changes in the Belgian heart disease prevention project. Acta Cardiol Suppl
1979;23:377--84.
DeLucia JL, Kalodner CR, Horan JJ. The effect of two nutritional software programs used as adjuncts to the behavioral treatment of
obesity. J Subst Abuse 1998;1:203--8.
Drummond S, Kirk T. The effect of different types of dietary advice on body composition in a group of Scottish men. J Hum Nutr
Diet 1998;11:473--85.
Forster JL, Jeffery RW, Sullivan S, Snell MK. A work-site weight
control program using financial incentives collected through payroll deduction.
J Occup Med 1985;27:804--8.
Forster JL, Jeffery RW, Snell MK. One-year follow-up study to a worksite weight control program. Prev Med 1988;17:129--33.
Fukahori M, Aono H, Saito I, Ikebe T, Ozawa H. Program of exercise training as total health promotion plan and its evaluation. J Occup
Health 1999;41:76--82.
Furuki K, Honda S, Jahng D, Ikeda M, Okubo T. The effects of a health promotion program on body mass index. J Occup Health 1999;41:19--26.
Gomel M, Oldenburg B, Simpson JM, Owen N. Work-site cardiovascular risk reduction: a randomized trial of health risk assessment,
education, counseling, and incentives. Am J Public Health 1993; 83:1231--8.
Gregg W, Foote A, Erfurt JC, Heirich MA. Worksite follow-up and engagement strategies for initiating health risk behavior changes. Health Educ
Q 1990;17:455--78.
Harrell JS, Johnson LF, Griggs TR, et al. An occupation based physical activity intervention program: improving fitness and decreasing
obesity. AAOHN J 1996;44:377--84.
Heirich MA, Foote A, Erfurt JC, Konopka B. Work-site physical
fitness programs. Comparing the impact of different program designs
on cardiovascular risks. J Occup Med 1993;35:510--7.
Hoiberg A, Berard S, Watten RH, Caine C. Correlates of weight loss in treatment and at follow-up. Int J Obes 1984;8:457--65.
James LC, Folen RA, Page H, Noce M, Brown J, Britton C. The Tripler LE3AN Program: a two-year follow-up report. Mil Med
1999;164:389--95.
Jeffery RW, Forster JL, Snell MK. Promoting weight control at the worksite: A pilot program of self-motivation using payroll-based
incentives. Prev Med 1985;14:187--94.
Jeffery RW, Forster JL, Schmid TL. Worksite health promotion: feasibility testing of repeated weight control and smoking cessation classes. Am
J Health Promot 1989;3:11--6.
Jeffery RW, Forster JL, French SA, et al. The Healthy Worker Project: a work-site intervention for weight control and smoking cessation.
Am J Public Health 1993;83:395--401.
Juneau M, Rogers F, DeSantos V, et al. Effectiveness of
self-monitored, home-based, moderate-intensity exercise training in middle-aged men
and women. Am J Cardiol 1987;60:66--70.
Nelson DJ, Senneh L, Lefebvre RC, Loiselle L, McClements L, Carlton RA. A campaign strategy for weight loss at worksites. Health Educ
Res Theory Pract 1987;2:27--31.
Okada K. Effects of long-term corporate fitness program on
employees' health. J Nutr Sci Vitaminol (Tokyo) 1991;37(Suppl):S131--8.
Pavlou KN, Krey S, Steffee WP. Exercise as an adjunct to weight loss and maintenance in moderately obese subjects. Am J Clin
Nutr 1989;49(Suppl 5):1115--23.
Pritchard JE, Nowson CA, Ward JD. A worksite program for overweight middle-aged men achieves lesser weight loss with exercise than
with dietary change. J Am Diet Assoc 1997;97:37--42.
Rose G, Heller RF, Pedoe HT, Christie DG. Heart disease prevention project: a randomised controlled trial in industry. Br Med
J 1980;280(6216):747--51.
Rose G, Tunstall-Pedoe HD, Heller RF. UK heart disease prevention
project: incidence and mortality results. Lancet 1983;1(8333):1062--6.
Shi L. The impact of increasing intensity of health promotion intervention on risk reduction. Eval Health Prof 1992;15:3--25.
Stamler R, Stamler J, Gosch FC, McDonald AM. Primary prevention of hypertension---a randomized controlled trial. Ann Clin
Res 1984;16(Suppl 43):136--42.
Steinhardt MA, Bezner JR, Adams TB. Outcomes of a traditional weight control program and a nondiet alternative: a one-year
comparison. J Psychol 1999;133:495--513.
Trent LK, Stevens LT. Evaluation of the Navy's obesity treatment
program. Mil Med 1995;160:326--30.
Erfurt JC, Foote A, Heirich MA. The cost-effectiveness of work-site wellness programs for hypertension control, weight loss,
and smoking cessation. J Occup Med 1991;33:962--70.
* Points of view are those of the contributors and the Task Force on Community Preventive Services and do not necessarily reflect those of CDC.
† The review team directs the review, in conjunction with a group of consultants. For these reviews, the members of the review team were David L. Katz,
MD, Meghan O'Connell, MPH, Ming-Chin Yeh, PhD, Haq Nawaz, MD, Yale Prevention Research Center, New Haven, Connecticut; Laurie M. Anderson,
PhD, Coordinating Center for Health Information and Services, CDC, Atlanta, Georgia. Consultants were Kelly Brownell, PhD, Department of Psychology,
Yale University, New Haven, Connecticut; Michael Bracken, PhD, Yale University School of Medicine, New Haven, Connecticut; Deanna Hoelscher,
PhD, University of Texas--Houston School of Public Health, Texas; Anjali Jain, MD, Department of Pediatrics, University of Chicago Children's Hospital,
Illinois; Neal Kohatsu, MD, California Department of Public Health, Sacramento; Nancy Berger, MPH, Connecticut Department of Public Health, Hartford.
Task Force on Community Preventive Services
September 1, 2005
Chairman: Jonathan E. Fielding, MD, Los Angeles Department of Health Services, California.
Vice-Chairman: Barbara K. Rimer, DrPH; University of North Carolina at Chapel Hill, North Carolina.
Members: John Clymer, Partnership for Prevention, Washington, DC; Kay Dickersin, PhD, Johns Hopkins University, Baltimore, Maryland; Alan
R. Hinman, MD, Task Force for Child Survival and Development, Atlanta, Georgia; Robert L. Johnson, MD, New Jersey Medical School, Newark,
New Jersey; Patricia A. Nolan, MD, Rhode Island Department of Health, Providence; Alonzo L. Plough, PhD, Public Health--Seattle and King
County, Washington; Nicolaas P. Pronk, PhD, HealthPartners Center for Health Promotion, Minneapolis, Minnesota; Dennis L. Richling, MD,
Midwest Business Group on Health, Chicago, Illinois; Steven M. Teutsch, MD, Merck and Co., Inc., West Point, Pennsylvania.
Consultants: Robert S. Lawrence, MD, Bloomberg School of Public Health, Johns Hopkins University, Baltimore, Maryland; J. Michael
McGinnis, MD, Robert Wood Johnson Foundation, Princeton, New Jersey; Lloyd F. Novick, MD, Onondaga County Department of Health, Syracuse, New York.
Former Members
Chairman: Caswell A. Evans, Jr., DDS, National Oral Health Initiative, Office of the U.S. Surgeon General, Rockville, Maryland.
Members: Patricia A. Buffler, PhD, University of California, Berkeley; Ross Brownson, PhD, St. Louis University School of Public Health,
Missouri; Noreen Morrison Clark, PhD, University of Michigan School of Public Health, Ann Arbor; Mary Jane England, MD, Regis College,
Weston, Massachusetts; David W. Fleming, MD, CDC, Atlanta, Georgia; Mindy Thompson Fullilove, MD, New York State Psychiatric Institute and
Columbia University, New York; Fernando A. Guerra, MD, San Antonio Metropolitan Health District, Texas; George J. Isham, MD, HealthPartners,
Minneapolis, Minnesota; Garland H. Land, MPH, Center for Health Information Management and Epidemiology, Missouri Department of Health, Jefferson
City; Charles S. Mahan, MD, University of South Florida, Tampa; Patricia Dolan Mullen, DrPH, University of Texas--Houston School of Public
Health, Houston; Susan C. Scrimshaw, PhD, University of Illinois School of Public Health, Chicago; Robert S. Thompson, MD, Group Health Cooperative
of Puget Sound, Seattle, Washington, also served on the Task Force while the recommendations were being developed.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
Disclaimer
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.