FIGURE. Annual rate* of tetanus cases and tetanus deaths --- National Notifiable Diseases Surveillance System, United States, 1947--2008
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Tetanus Surveillance --- United States, 2001--2008
Tetanus is a life-threatening but preventable disease caused by the toxin of Clostridium tetani, a ubiquitous, spore-forming, gram-positive bacillus found in high concentrations in soil and animal excrement. Reported tetanus cases have declined >95%, and deaths from tetanus have declined >99% in the United States since 1947, when the disease became reportable nationally. To update a previous report (1) and to determine the populations at greatest risk for the disease, CDC analyzed cases reported to the National Notifiable Diseases Surveillance System (NNDSS) during 2001--2008. This report summarizes the results of that analysis, which found that 233 tetanus cases were reported during 2001--2008; among the 197 cases with known outcomes, the case-fatality rate was 13.2%. Average annual incidence during that period was 0.10 per 1 million population overall and 0.23 among persons aged ≥65 years. Incidence among Hispanics was nearly twice that among non-Hispanics, a difference accounted for by 16 cases among Hispanic injection drug users (IDUs). Among the 92 patients for whom tetanus toxoid-containing (TT) vaccination status was available, 37 (40.2%) had received no doses of TT vaccine. Thirty (15.4%) of 195 patients had diabetes, and 27 (15.3%) of 176 were IDUs. Of 51 patients with an acute wound and a surveillance report complete enough to evaluate tetanus prophylaxis, 49 (96.1%) had not received appropriate prophylaxis. Tetanus remains a rare but life-threatening disease in the United States. Health-care providers should ensure up-to-date TT vaccination of all their patients, especially persons aged ≥65 years, persons with diabetes, and injection drug users.
From 1947 to 2008, the number of tetanus cases reported each year, which already had decreased greatly since 1900, continued to decline (Figure), in part because of continued use of tetanus antitoxin for wound management and introduction of TT vaccines in the 1930s and 1940s, which led to universal childhood immunization and the addition of decennial TT boosters for adults (2,3). A major contributor to the decline in morbidity was the near elimination of neonatal tetanus, a result attributable to improved childbirth practices and to increased levels of maternal immunity resulting from universal childhood vaccination (1). Sporadic cases of tetanus continue to occur in adults, especially in persons who were not vaccinated in childhood; during 1998--2000, a tetanus cluster was reported among IDUs in California (1). National surveillance for tetanus is conducted to monitor trends in incidence and identify populations at increased risk.
NNDSS is a passive surveillance system that relies on physicians to report cases of tetanus to state and local health departments. Because no laboratory test provides definitive confirmation of tetanus, the diagnosis is based on the clinical judgment of attending physicians and the exclusion of other causes of disease. For reporting cases to NNDSS, health-care providers use the following definition adopted by the Council of State and Territorial Epidemiologists and CDC in 1990: a confirmed case is an acute onset of hypertonia and/or painful muscular contractions (usually of the muscles of the jaw and neck) and generalized muscle spasms without other apparent medical cause, as reported by a health professional.
Tetanus case reports, including supplemental information (e.g., clinical history, patient vaccination status, wound care, clinical management, and outcome) and epidemiologic information are verified by health departments and transmitted electronically to CDC. Vaccination histories of patients are not validated by CDC. Tetanus rates by age and race/ethnicity were calculated using mid-year postcensal population estimates for the years 2001--2008. Risk factors for death resulting from tetanus were assessed by univariate analyses followed by multivariate modeling.
During 2001--2008, a total of 233 cases were reported from 45 states; 26 (13.2%) of 197 cases for which outcome was reported were fatal. A total of 120 cases (51.5%) were reported from five states: California (60), Florida (25), Texas (12), New York (12), and Pennsylvania (11). An average of 29 cases was reported each year (range: 19--40). The average annual incidence was 0.10 per 1 million population (Table 1) and showed a slightly declining trend (Figure).
Sex and age were reported for all 233 cases. A total of 138 (59.2%) patients were male; median age was 49 years (range: 5--94 years), excluding one nonfatal neonatal case.* Average annual incidence was higher among those aged ≥65 years (0.23 cases per 1 million population) than among those aged 5--64 years (0.08 per 1 million population) (Table 1). Data on race were available for 179 (76.8%) cases; incidence was similar by race: white (0.08 per 1 million population), black (0.07), American Indian/Alaska Native (0.09), Asian/Pacific Islander (0.07), and other race (0.02). Data on Hispanic ethnicity were available for 185 (79.4%) cases. The incidence among Hispanics was almost twice that among non-Hispanics (0.13 versus 0.07 cases per 1 million population); however, when IDUs were excluded, the incidence was almost the same among Hispanics (0.08) compared with non-Hispanics (0.07).
TT vaccination status was reported for 92 (39.5%) of the 233 patients. A total of 37 patients (40.7%) received no TT doses, 26 (28.3%) received 1 dose, five (5.4%) received 3 doses, and 24 (26.1%) received ≥4 doses (Table 2). Among the 36 patients aged ≥50 years, five (13.9%) reported completing the primary 3-dose TT series, compared with 24 (42.9%) of the 56 aged <50 years. Seven (24.1%) of 29 patients with ≥3 doses of TT had received their last dose within 10 years, 18 (62.1%) from 10 to 54 years previously, and four (13.8%) reported an unknown interval since their last dose.
Among 195 patients whose medical history was known, 30 (15.4%) were reported to have diabetes. Twenty-seven (15.3%) of 176 patients whose status was known were IDUs, of whom 16 (59.3%) were Hispanic. Three (11.1%) of 27 patients with diabetes and known drug use status were IDUs. An acute wound preceded disease onset in 167 (71.7%) patients. Of those patient wounds, 132 (79.0%) were punctures, or contaminated, infected, or devitalized wounds considered tetanus-prone and eligible to receive tetanus immune globulin (TIG) (4). Sixty-one (36.5%) of the 167 patients with acute wounds sought medical care. Case reports for 51 (83.6%) of those who sought care were sufficiently complete to evaluate prophylaxis received; 49 (96.1%) did not receive appropriate TT prophylaxis or TT plus TIG as is currently recommended (4). Among all 233 patients, 31 (13.3%) reported a chronic wound or infection before disease onset, including diabetic ulcers and dental abscesses. Twenty-two (9.4%) reported no wounds or infections; of these, 14 were IDUs.
Among all persons with reported tetanus, the risk for fatal disease was greater among those aged ≥65 years than those aged <65 years (relative risk [RR] = 5.1; 95% confidence interval [CI] = 2.1--12.2), among those with diabetes than those without diabetes (RR = 2.4; CI = 1.2--4.8), and among those with no TT vaccination compared with those with ≥1 doses of TT (RR = 4.0; CI = 1.2--14.1). However, in the multivariable model, comparing age ≥65 years versus <65 years, diabetes versus no diabetes, and no doses of vaccination versus 1 dose, neither diabetes (odds ratio [OR] = 1.3; CI = 0.2--7.2) nor vaccination (OR = 3.1; CI = 0.7--15.1) were statistically significant. Age ≥65 years remained a factor for greater risk for fatal tetanus (OR = 9.6 ; CI = 3.6--25.0) in a final parsimonious model including only age. Sex, injection drug use, Hispanic ethnicity, unknown vaccination history, and acute injuries (versus chronic wounds) were not associated with increased risk for fatal disease in either univariate or multivariable analyses.
Reported by
T Tiwari, MD,* TA Clark, MD, NE Messonnier, MD, Div of Bacterial Diseases, National Center for Immunization and Respiratory Diseases; CG Thomas, DVM, EIS Officer, CDC. *Corresponding contributor: Tejpratap Tiwari, Div of Bacterial Diseases, National Center for Immunization and Respiratory Diseases, CDC, 404-639-8765, ttiwari@cdc.gov.
Editorial Note
Inadequate TT vaccination and inadequate wound prophylaxis remain the most important factors associated with tetanus. The findings in this report indicate that older adults are at greater risk for tetanus than younger persons, and the risk for fatal disease is higher among patients aged ≥65 years. This increased risk likely results from inadequate vaccination rather than inadequate response to vaccination, because tetanus toxoid is sufficiently immunogenic in older adults (5). In this analysis, only one patient aged ≥50 years reported having received a complete primary series and up-to-date boosters. Surveys of adults have shown declining TT vaccination coverage with increasing age, with coverage of <50% observed among persons aged ≥65 years in 2007 (6). Missed opportunities to vaccinate adult women and older adults in primary-care settings are common (7,8). Providers should review vaccination status during adult health-care visits to ensure that persons with inadequate vaccination complete the primary tetanus series and are up-to-date with booster doses.
In this analysis, approximately one third of patients with acute wounds sought medical care, and among those who sought care and had sufficient case data, fewer than 4% received appropriate TT prophylaxis or TT plus TIG as recommended (4). Patients might not receive optimal tetanus prophylaxis as part of wound management because of the trivial appearance of many wounds and the failure of health-care providers to obtain a vaccination history, particularly from those who are not up to date with their TT vaccination (9).
Populations considered at increased risk for tetanus include persons with tetanus-prone wounds, IDUs, and those with diabetes and chronic wounds. The prevalence of diabetes among patients in this analysis was 15%, nearly three times the average estimated prevalence of diabetes in the United States during 2001--2008 (10). Although the mechanism for increased risk is unclear, one possible explanation is that health-care providers might not suspect tetanus early in persons with chronic wounds and diabetes; approximately 13% of tetanus patients reported a chronic wound or infection before onset. Health-care providers should incorporate up-to-date decennial TT vaccination into routine diabetes management to prevent tetanus (6). Of those who reported no wound or infections, the majority were IDUs. The mechanism for the greater tetanus risk among IDUs likely is introduction of tetanus spores through contaminated heroin or injection needles.
During 2001--2008, 71.7% of tetanus patients had acute wounds, but only 36.5% sought immediate medical care, thus limiting the effectiveness of secondary prevention strategies. This finding was nearly identical to that of a previous report for the period 1982--2000 (1). These data also support previous studies indicating that provision of prophylaxis is not always optimal, at least in part because tetanus can result from seemingly trivial wounds that would not trigger suspicion of tetanus risk; clinical determination of tetanus-prone wounds is not exact (4,9). In addition, this report indicates that, during 2001--2008, 13% of patients reported experiencing chronic wounds or conditions that were considered the source of tetanus infection. Many of these were not considered classic tetanus-prone wounds, according to treatment guidelines.
The findings in this report are subject to at least two limitations. First, surveillance for tetanus is passive and likely to be limited by underreporting and potential misclassification of disease. Second, because not all tetanus case reports were complete, missing data regarding outcome, risk factors, and other patient characteristics might affect the accuracy of the case-fatality ratio and certain other calculations.
Because C. tetani is ubiquitous in the environment, thorough assessment and management of wounds are especially important to the prevention of tetanus. Health-care providers should assess their patients' TT vaccination status with particular emphasis on up-to-date vaccination, especially if the patients are older adults, IDUs, persons with diabetes, and persons with chronic wounds.
Acknowledgments
This report is based, in part, on contributions by T Pondo, MS, CE Rose Jr, PhD, Div of Bacterial Diseases, K Brown, MPH, Global Immunization Div, National Center for Immunization and Respiratory Diseases; P Srivastava , MS, Office of the Director, Office of Infectious Diseases; S Shah, MS, Div of HIV/AIDS Prevention Surveillance and Epidemiology, National Center for HIV, Viral Hepatitis, STD, and TB Prevention, CDC.
References
- CDC. Tetanus surveillance---United States, 1998--2000. MMWR 2003;52(No. SS-3).
- CDC. National, state, and local area vaccination coverage among children aged 19--35 months---United States, 2008. MMWR 2009;58:921--6.
- CDC. National, state, and local area vaccination coverage among adolescents aged 13--17 years---United States, 2008. MMWR 2009;58:997--1001.
- CDC. Preventing tetanus, diphtheria, and pertussis among adults: use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine (Tdap). Recommendations of the Advisory Committee on Immunization Practices (ACIP) and recommendations of ACIP, supported by the Healthcare Infection Control Practices Advisory Committee (HICPAC), for use of Tdap among health-care personnel. MMWR 2006;55(No. RR-17).
- Topinkova E, Maresova V. Tetanus and pertussis vaccines: their usefulness in the aging population. Aging Clin Exp Res 2009;21:229--35.
- CDC. Vaccination coverage among U.S. adults, National Immunization Survey---adult, 2007. Atlanta, GA: US Department of Health and Human Services, CDC; 2008. Available at http://www.cdc.gov/vaccines/stats-surv/nis/downloads/nis-adult-summer-2007.pdf. Accessed March 28, 2011.
- Backer EL, Gregory P, Jaén CR, Crabtree BF. A closer look at adult female health care maintenance visits. Fam Med 2006;38:355--60.
- Nowalk MP, Zimmerman RK, Cleary SM, Bruehlman RD. Missed opportunities to vaccinate older adults in primary care. J Am Board Fam Pract 2005;18:20--7.
- Talan DA, Abrahamian FM, Moran GJ, et al. Tetanus immunity and physician compliance with tetanus prophylaxis practices among emergency department patients presenting with wounds. Ann Emerg Med 2004;43:305--14.
- CDC. Crude and age-adjusted percentage of the civilian, noninstitutionalized population with diagnosed diabetes, United States, 1980--2007. Atlanta, GA: US Department of Health and Human Services, CDC; 2010. Available at http://www.cdc.gov/diabetes/statistics/prev/national/figage.htm. Accessed March 28, 2011.
* The patient was a premature male who was delivered at home and developed tetanus 11 days after birth. His mother was an immigrant with an unknown vaccination history.
What is already known on this topic?
In 1947, the first year that tetanus became reportable nationally in the United States, the rate of reported cases was 3.9 per 1 million population. Since then, cases have declined >95% with universal childhood vaccination with tetanus toxoid--containing (TT) vaccines, decennial TT boosters, improved wound management with tetanus antitoxin, and improved childbirth practices; however, sporadic cases in adults still occur, especially in those not vaccinated during childhood.
What is added by this report?
During 2001--2008, the average annual incidence of tetanus in the United States was 0.10 cases overall per 1 million population and 0.23 among persons aged ≥65 years; the case-fatality rate was 13.2% overall but 31.3% among persons aged ≥65 years.
What are the implications for public health practice?
Health-care providers should periodically assess their patients' TT vaccination status, with particular emphasis on up-to-date vaccination for those likely to be vaccinated inadequately or at increased risk for disease, such as persons aged ≥65 years, those with diabetes, and injection drug users.
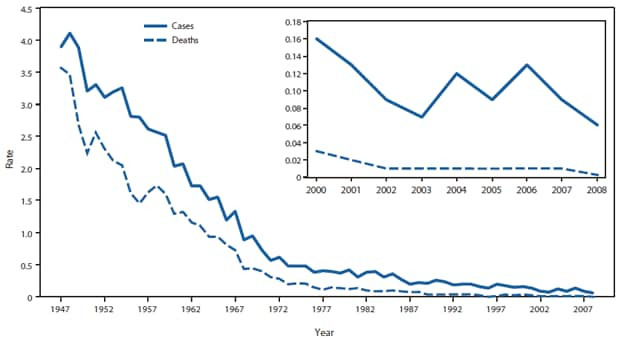
* Per 1 million population.
Alternate Text: The figure above shows the annual rate of tetanus cases and tetanus deaths in the United States during 1947-2008, according to the National Notifiable Diseases Surveillance System. From 1947 to 2008, the number of tetanus cases reported each year, which already had decreased greatly since 1900, continued to decline
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
