FIGURE 1. Number of laboratory-confirmed cases of 2009 pandemic influenza A (H1N1)* per 100,000 population, by administrative periphery --- Greece, May 18, 2009--February 28, 2010
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Deaths and Hospitalizations Related to 2009 Pandemic Influenza A (H1N1) --- Greece, May 2009--February 2010
![]()
The first laboratory-confirmed case of 2009 pandemic influenza A (H1N1) in Greece was reported on May 18, 2009. During July--August, Greece experienced a moderate wave of transmission of 2009 H1N1; a stronger wave began in October, and a peak in incidence occurred during November 23--29. To conduct surveillance in Greece for 2009 H1N1, the Hellenic Centre for Diseases Control and Prevention (HCDCP), in collaboration with the National Health Operations Centre (NaHOC) of the Ministry of Health and Social Solidarity, collected and analyzed data regarding 1) laboratory-confirmed 2009 H1N1 cases, 2) influenza-like illness (ILI) visits to hospital emergency departments (EDs), 3) ILI hospitalizations, 4) confirmed 2009 H1N1 admissions to intensive-care units (ICUs), and 5) confirmed 2009 H1N1 deaths in hospitals. This report summarizes the findings in Greece during May 18, 2009--February 28, 2010, when 18,075 laboratory-confirmed 2009 H1N1 cases, 294 ICU admissions, and 140 deaths were reported. The majority of severe 2009 H1N1 cases were associated with underlying medical conditions (68.4% of ICU admissions and 82.1% of deaths), including pregnancy. In Greece, where 2009 H1N1 vaccination coverage was limited and a large proportion of the population likely remains susceptible (1), continued surveillance and effective vaccination programs will be needed this winter to combat 2009 H1N1 and any other circulating influenza virus.
The first case of 2009 H1N1 in Greece was reported on May 18, 2009, approximately 4 weeks after the first reports of novel influenza A cases in Mexico and the United States (2,3). An enhanced surveillance system for 2009 H1N1 was implemented in Greece during April 30--July 14, 2009. During this period, clinicians collected respiratory specimens for laboratory testing by real-time reverse transcription--polymerase chain reaction (rRT-PCR) from persons who met the European Union definition for a 2009 H1N1 case under investigation: temperature >100.4oF (>38oC) plus symptoms of acute respiratory infection and, in the week preceding onset of symptoms, history of travel to an affected area or history of close contact with a patient with confirmed 2009 H1N1 illness during that patient's illness (4). Most laboratory-confirmed cases identified during this period were travel associated. On July 15, 2009, contact tracing was discontinued, and criteria for laboratory testing were tightened to severe cases requiring hospitalization, selected cases from clusters of ILI, and special situations according to clinical judgment.
For this analysis, a confirmed case was defined as a positive test result for the 2009 H1N1 virus by rRT-PCR during May 18, 2009--February 28, 2010. Nasopharyngeal swabs were collected by hospitals and general practitioners participating in a sentinel surveillance network and were sent for testing to designated reference laboratories. ILI was defined in accordance with European Union directive 2008/426/EC as a sudden onset of illness with 1) at least one of the following: fever or feverishness, malaise, headache, or myalgia, plus 2) at least one of the following: cough, sore throat, or shortness of breath. Surveillance data on laboratory-confirmed 2009 H1N1 cases, ILI visits to hospital emergency departments, ILI hospitalizations, and laboratory-confirmed cases in persons admitted to ICUs, were collected by HCDCP and NaHOC. Surveillance for deaths among persons with laboratory-confirmed 2009 H1N1 in hospital settings was performed by HCDCP in collaboration with NaHOC.
All hospital administrators in Greece were asked to report daily to NaHOC, via standardized forms, the number of patients who visited their ED with ILI symptoms and the number of new admissions for ILI. In addition, hospitals were asked to report, three times weekly, all patients admitted with laboratory-confirmed 2009 H1N1, along with the admission diagnosis and current patient status. On a daily basis, investigators made follow-up telephone calls to the physicians of all patients with confirmed cases of 2009 H1N1 who were admitted to an ICU. Data on hospital morbidity were collected by NaHOC from a network that included all state and private hospitals in the seven semiautonomous regional health authorities of Greece.
A total of 114 public general hospitals, 172 private hospitals, and 12 military hospitals in Greece were eligible for participation. Of the eligible hospitals, 70.2% participated in data collection for both ILI visits to EDs and ILI hospitalizations, accounting for 79.4% of the total patient capacity of Greek public hospitals. Hospitals that did not participate in data collection had lower bed capacity (182 mean bed capacity versus 299) and were more likely to be located on Greek islands (41.1%) than the participating hospitals (11.3%). Age-specific 2009 H1N1 admission to ICUs and mortality rates were calculated using the estimated age-specific population of Greece for 2009 (as provided by the General Secretariat of the National Statistical Service of Greece). The rates were calculated for May 18, 2009--February 28, 2010.
During May 18, 2009--February 28, 2010, a total of 18,075 laboratory-confirmed 2009 H1N1 cases were reported. Laboratory-confirmed illness rates per 100,000 population varied among the 13 administrative peripheries of Greece (Figure 1). Two waves of 2009 H1N1 transmission were observed. A moderate wave occurred during July--August and was followed by a decrease in cases through mid-October, when incidence accelerated rapidly, peaked during November 23--29, and then declined steadily (Figure 2). During May 18, 2009--February 28, 2010, a total of 88,244 ILI visits to EDs and 10,040 ILI hospitalizations also were reported (Figure 2).
A total of 294 ICU admissions and 140 deaths related to 2009 H1N1 were reported during May 18, 2009--February 28, 2010 (Figure 3). Of the 294 ICU admissions, 241 patients (82.0%) required mechanical ventilation, and 201 (68.4%) had an underlying medical condition (e.g., chronic respiratory, cardiovascular, renal, or hepatic disease; chronic metabolic disorder; or immunosuppression); 13 patients were pregnant. The most commonly reported underlying medical conditions among those admitted to an ICU were obesity (26.2%) and cardiovascular disease (16.3%). The most commonly reported underlying conditions among persons aged ≤19 years were neurologic disorders (31.3%), whereas obesity was the most commonly reported condition among persons aged 20--60 years (31.5%). Among persons aged >60 years, the most commonly reported condition was cardiovascular disease (37.3%).
Of the 140 patients whose deaths were related to 2009 H1N1, 115 (82.1%) had at least one underlying medical condition. The most commonly reported underlying medical conditions among those who died were obesity (25.5%), diabetes (24.8%), and cardiovascular disease (22.7%). One of the deceased was pregnant and had underlying cardiovascular disease. Of the 140 patients who died, 89 (63.5%) were aged <60 years, including eight (5.7%) who were aged <19 years.
During May 18, 2009--February 28, 2010, the rate for ICU admission with 2009 H1N1 was estimated at 2.6 cases per 100,000 population (95% confidence interval [CI] = 2.3--2.9), and the death rate related to 2009 H1N1 was estimated at 1.2 deaths per 100,000 population (CI = 1.1--1.5). The rate for ICU admission was highest among persons aged 40--59 years (3.9 per 100,000 population). Death rates ranged from 0.4 to 0.7 per 100,000 population among groups aged ≤39 years, and the rate was higher (1.8 per 100,000 population) among persons aged ≥40 years.
Reported by
P Efstathiou, MD, DSc, M Tseroni, A Baka, MD, Z Manolidou, K Karageorgou, MD, National Health Operations Centre, Ministry of Health and Social Solidarity; V Sypsa, PhD, A Hatzakis, PhD, Univ of Athens, Greece.
Editorial Note
This is the first report to summarize the epidemiology of 2009 H1N1 in Greece. During July--August 2009, Greece experienced a moderate wave of transmission, followed by a stronger wave beginning in October and peaking during November 23--29. In Greece, the first 2009 H1N1 cases were associated with imported transmission (e.g., students returning to Greece from abroad and foreign tourists) (5). On July 15, 2009, contact tracing was discontinued, and criteria for laboratory testing were tightened sharply. Because of these restrictions on testing and because many persons with influenza might not have sought medical care, the number of laboratory-confirmed 2009 H1N1 cases noted in this report likely is a substantial underestimate of the actual number that occurred during May 18, 2009--February 28, 2010.
The estimated 2009 H1N1-related ICU admission and death rates in Greece (2.6 and 1.2 per 100,000 population, respectively) were within the range of estimates reported by countries in the southern hemisphere for their winter months (June--August 2009) (6,7). Despite a sharp decrease in the number of ILI visits to EDs and laboratory-confirmed 2009 H1N1 cases after transmission peaked during November 23--29, the weekly numbers of 2009 H1N1 admissions to an ICU, and particularly deaths, declined more gradually. Corresponding data from the United States were similar; U.S. laboratory confirmations of influenza peaked during the week of October 24, 2009, but reports of deaths declined more slowly (8). Consistent with findings in other countries, obesity appeared to be a risk factor in Greece for 2009 H1N1--related admission to an ICU or death; however, additional analysis is needed.
The findings in this report are subject to at least three limitations. First, although participation in the surveillance network was high, because participating hospitals accounted for 79.4% of the total patient capacity of Greek public hospitals, data on ILI visits to EDs and hospitalizations are not complete. In contrast, because of daily communication between HCDCP and NaHOC and participating hospitals, data on 2009 H1N1 ICU admissions and deaths within the hospital setting are thought to be nearly complete. Second, substantial underestimation of 2009 H1N1 cases likely occurred, largely because of restrictions on confirmatory laboratory testing. Finally, the number of deaths related to 2009 H1N1 might have been underestimated because deaths that occurred outside the hospital setting might not have been identified and testing that was performed on hospital patients might not have been sensitive to influenza or might have been performed later in the course of illness, when influenza shedding had declined substantially or ceased.
Vaccination against 2009 H1N1 in Greece was initiated at the end of November 2009, with the intent ultimately to administer the vaccine, at no charge, to anyone who wished to receive it. Vaccination initially was offered to health-care workers, then to persons aged ≥6 months at high risk for complications from influenza, then to healthy persons aged 6 months--49 years, and finally to healthy adults aged >49 years. Although the goal was widespread coverage, as of February 28, 2010, only 3.2% of the Greek population had been vaccinated for 2009 H1N1 (1). In contrast, among U.S. states and territories, an estimated 23.9% of persons aged ≥6 months had been vaccinated through January 2010 (9). According to the results of one survey, the main reason that residents of Greece chose not to receive the 2009 H1N1 vaccine was a belief that the vaccine might not be safe (10).
Acknowledgments
The findings in this report are based, in part, on contributions by S Bonovas and T Panagiotopoulos, Dept of Epidemiological Surveillance and Intervention, Hellenic Centre for Infectious Diseases Control and Prevention, Greece; and A Papagiannopoulou, M Lekka, A Vilaeti, S Papadogiannopoulos, I Agrafa, and C Skafidas.
References
- Tsiodras S, Sypsa V, Hatzakis A. The vaccination campaign against 2009 pandemic influenza A (H1N1) and its continued importance in view of the uncertainty surrounding the risk associated with the pandemic [Letter]. Euro Surveill 2010;15:pii = 19468.
- CDC. Swine influenza A (H1N1) infection in two children---southern California, March--April 2009. MMWR 2009;58:400--2.
- CDC. Outbreak of swine-origin influenza A (H1N1) virus infection---Mexico, March--April 2009. MMWR 2009;58:467--70.
- Official Journal of the European Union. Commission decision of 30 April 2009. Available at http://eurlex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2009:110:0058:0059:EN:PDF. Accessed June 4, 2010.
- Lytras T, Theocharopoulos G, Tsiodras S, Mentis A, Panagiotopoulos T, Bonovas S; influenza surveillance report group. Enhanced surveillance of influenza A (H1N1)v in Greece during the containment phase. Euro Surveill 2009;14:pii = 19275.
- ANZIC Influenza Investigators. Critical care services and 2009 H1N1 influenza in Australia and New Zealand. N Engl J Med 2009;361:1925--34.
- Baker MG, Kelly H, Wilson N. Pandemic H1N1 influenza lessons from the southern hemisphere. Euro Surveill 2009;14:pii = 19370.
- CDC. FluView. 2009--2010 influenza season week 14 ending April 10, 2010. Available at http://www.cdc.gov/flu/weekly/weeklyarchives2009-2010/weekly14.htm. Accessed June 4, 2010.
- CDC. Interim results: state-specific influenza A (H1N1) 2009 monovalent vaccination coverage---United States, October 2009--January 2010. MMWR 2010;59:363--8.
- Sypsa V, Livanios T, Psichogiou M, et al. Public perceptions in relation to intention to receive pandemic influenza vaccination in a random population sample: evidence from a cross-sectional telephone survey. Euro Surveill 2009;14:pii = 19437.
What is already known on this topic?
The incidence of 2009 pandemic Influenza A (H1N1) peaked in November 2009 in Europe.
What is added by this report?
Greece experienced two waves of 2009 H1N1 transmission, a moderate one during the summer and a stronger one that peaked at the end of November 2009; the intensive-care unit admission rate and death rate among hospitalized patients from May 2009 to February 2010 were 2.6 cases and 1.2 deaths per 100,000 population, respectively.
What are the implications for public health practice?
Continued surveillance and effective vaccination programs will be needed to combat 2009 H1N1 and any other circulating influenza viruses in the coming winter months.
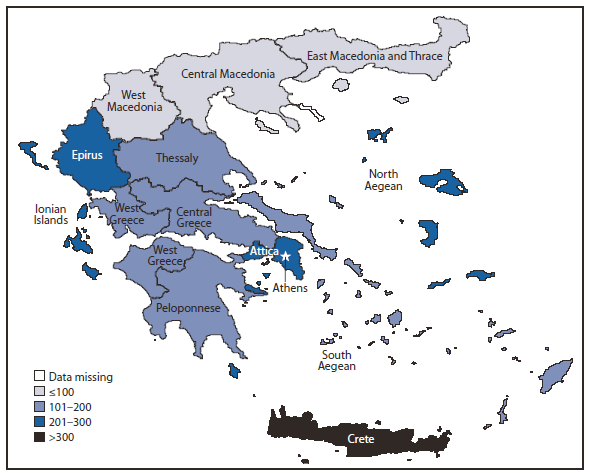
* N = 18,075.
Alternate Text: The figure above shows the number of laboratory-confirmed cases of 2009 pandemic influenza A (H1N1) per 100,000 population, by administrative periphery in Greece from May 18, 2009-February 28, 2010. During May 18, 2009-February 28, 2010, a total of 18,075 laboratory-confirmed 2009 H1N1 cases were reported. Laboratory-confirmed illness rates per 100,000 population varied among the 13 administrative peripheries of Greece.
FIGURE 2. Number of laboratory-confirmed 2009 pandemic influenza A (H1N1) cases,* influenza-like illness (ILI) visits to emergency departments (ED),† and ILI hospitalizations§ --- Greece, May 18, 2009--February 28, 2010
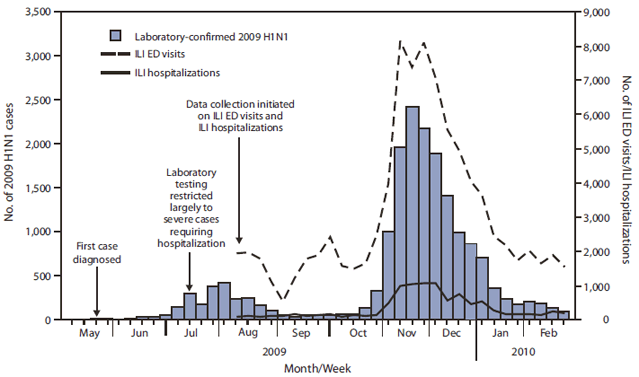
* By week of diagnosis (N = 18,075).
† By week of visit (N = 88,244).
§ By week of admission (N = 10,040).
Alternate Text: The figure above shows the number of laboratory-confirmed 2009 pandemic influenza A (H1N1) cases, influenza-like illness (ILI) visits to emergency departments, and ILI hospitalizations in Greece, May 18, 2009-February 28, 2010. A moderate wave occurred during July-August and was followed by a decrease in cases through mid-October, when incidence accelerated rapidly, peaked during November 23-29, and then declined steadily.
FIGURE 3. Number of admissions to an intensive-care unit (ICU)* for laboratory-confirmed 2009 pandemic influenza A (H1N1) and number of deaths --- Greece, May 18, 2009--February 28, 2010
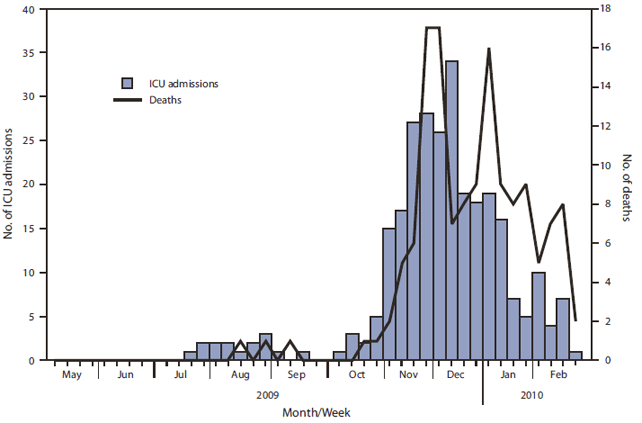
* By week of admission (N = 294).
† By week of death (N = 140).
Alternate Text: The figure above shows the number of admissions to an intensive-care unit (ICU) for laboratory-confirmed 2009 pandemic influenza A (H1N1) and number of deaths in Greece, during May 18, 2009-February 28, 2010. A total of 294 ICU admissions and 140 deaths related to 2009 H1N1 were reported during May 18, 2009-February 28, 2010.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
