|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
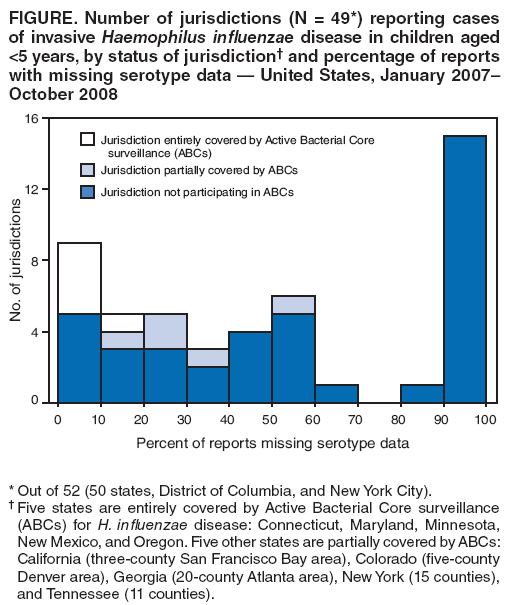
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Continued Shortage of Haemophilus influenzae Type b (Hib) Conjugate Vaccines and Potential Implications for Hib Surveillance --- United States, 2008In December 2007, Merck & Co., Inc. (West Point, Pennsylvania) announced a voluntary recall of certain lots of two Haemophilus influenzae type b (Hib) conjugate vaccines, PedvaxHIB® (monovalent Hib vaccine) and Comvax® (Hib-HepB vaccine) and suspended production of both vaccines, disrupting the U.S. supply of Hib vaccine (1). When the recall was announced, Merck projected restoration of these vaccines to the U.S. market in late 2008. To ensure that enough vaccine would be available for all U.S. children to complete the primary Hib vaccination series, on December 18, 2007, CDC recommended that providers defer the booster dose of Hib vaccine (scheduled for administration at age 12--15 months) for all children except those at increased risk for invasive Hib disease (1). On October 17, 2008, Merck announced that restoration of the two vaccines to the market would be delayed until mid-2009. Because the continued delay might result in an increase in Hib disease, national surveillance for invasive Hib disease has become particularly important. To assess the current status of surveillance for Hib nationally, CDC reviewed 4,657 cases of invasive H. influenzae infection reported during January 2007--October 2008, including 748 cases among children aged <5 years. Of those 748 cases, 45 (6.0%) were Hib (serotype b), and 278 (37.2%) were missing serotype information. The continued vaccine shortage heightens the need for timely reporting and investigation of H. influenzae cases and accurate serotyping of all invasive H. influenzae isolates in children aged <5 years. H. influenzae disease can be caused by any of six H. influenzae serotypes (a, b, c, d, e, and f) or by nontypeables. Until 1988, when Hib vaccine was introduced, serotype b caused approximately 95% of cases of H. influenzae invasive disease among children aged <5 years (2); after introduction of the vaccine, during 1989--1995, the incidence of Hib disease decreased 95% among children in that age group (3). Cases of invasive H. influenzae are reported to CDC weekly from all 50 states, the District of Columbia (DC), and New York City, through the National Notifiable Diseases Surveillance System (NNDSS). All 50 states require reporting of Hib cases (defined in NNDSS as isolation of Hib from a normally sterile site) in children aged <5 years; however, reporting requirements vary for other serotypes of H. influenzae and for Hib in other age groups. CDC also coordinates the Active Bacterial Core surveillance (ABCs) system, which provides active, population-based, laboratory-based surveillance for invasive bacterial diseases, including H. influenzae (4). ABCs conducts surveillance in all or parts of 10 states,* accounting for 12% of the United States population. For ABCs, a case of H. influenzae disease is defined as isolation of H. influenzae from a normally sterile site in a resident of the surveillance area. For this analysis, cases of H. influenzae disease reported to NNDSS during January 2007--October 2008 were combined with cases reported through ABCs; cases were matched by date of birth and county of residence, and duplicates were excluded. Completeness of serotype reporting was assessed for all of the H. influenzae reports. Isolates were classified as b, non-b (other serotypes and nontypeables), or as having missing serotype information. Serotype reporting was assessed for patients of all ages and for those patients aged <5 years. During January 2007--October 2008, a total of 4,657 cases of invasive H. influenzae disease were reported to CDC; 127 cases (2.7%) were type b, 2,267 (48.7%) were non-b, and 2,263 (48.6%) were missing serotype information. Among children aged <5 years, 748 H. influenzae cases were reported; 45 (6.0%) were type b, 425 (56.8%) were non-b, and 278 (37.2%) were missing serotype information. Based on the merged NNDSS/ABCs data, the average annual rate of invasive Hib disease reported in children aged <5 years, during January 2007--October 2008, was 0.12 cases per 100,000 children per year. During 2007, the annual rate was 0.11 cases per 100,000 children aged <5 years, and during January--October 2008, the annual rate was 0.13 cases per 100,000. Overall, 49 of 52 jurisdictions (50 states, DC, and New York City) reported at least one case of H. influenzae to NNDSS or ABCs in a child aged <5 years. Of the 49 jurisdictions, a total of 19 (38.8%) were missing serotype data for >50% of reported cases, 16 (32.7%) were missing serotype data for >75% of reported cases, and 14 (28.6%) were missing serotype data for all reported cases (Figure). Among the five jurisdictions entirely covered by ABCs, four had no reported cases with missing serotype data. Among the five jurisdictions partially covered by ABCs, the median percentage of cases with missing data was 21.7%; among the 39 remaining jurisdictions not participating in ABCs, the median was 50.0% (Figure). Reported by: F Coronado, MD, K Brown, MPH, A Cohn, MD, N Messonnier, MD, TA Clark, MD, National Center for Immunization and Respiratory Diseases; M Jackson, PhD, EIS Officer, CDC. Editorial Note:The primary Hib vaccine series protects infants against invasive Hib disease. However, serum antibody levels decrease by age 12--15 months in children who have completed the primary series (5), and the Advisory Committee on Immunization Practices recommends that children receive a booster dose at that age (6). Higher concentrations of serum antibodies might be required to interrupt Hib transmission and colonization of the upper respiratory tract than to protect against invasive Hib disease (7). Thus, the booster dose can be of particular importance for indirect protection and promotion of herd immunity against Hib disease. In December 2007, Merck recalled certain lots of PedvaxHIB and Comvax and suspended production of these vaccines because the company was unable to assure the sterility of equipment used during manufacture of those lots (1). Interim Hib vaccine recommendations by CDC, in consultation with other organizations, stipulated that vaccination providers defer administering the booster vaccine dose to children not at increased risk for Hib disease until vaccine supply is restored (1). Those at increased risk include American Indian/Alaska Native (AI/AN) children and children with certain immunosuppressive conditions (1). The recommendations stated that providers should register and track children for whom the booster was deferred to facilitate recalling them for vaccination once supply problems are resolved. In October 2008, Merck announced that the company had identified the need for an additional manufacturing change and associated regulatory approval and did not expect to restore availability of these vaccines until mid-2009. Sufficient vaccine exists in the United States to provide the primary series and booster dose for AI/AN children and others at increased risk through at least mid-2009. However, the continued delay in restoring these vaccines to the market means continuing the interim recommendations for deferral of Hib booster vaccines for children not at increased risk. What effect continued deferral of the Hib booster might have on the incidence of invasive Hib disease in young children in the United States is unknown. In this analysis, the annual rate of invasive Hib disease in children aged <5 years was 0.13 per 100,000 during January--October 2008, compared with 0.11 per 100,000 children in 2007 and an average of 0.3 cases per 100,000 per year during 1998--2000, the period of the last published analysis of Hib using NNDSS/ABCs data (8). This analysis has not shown an increase in invasive Hib disease in children aged <5 years since the December 2007 vaccine recall. However, the history of Hib disease in the United Kingdom suggests that prolonged deferral of the Hib booster dose might yet lead to changes in the epidemiology of Hib disease in the United States. In the United Kingdom, Hib conjugate vaccines were introduced in 1992 as a 3-dose primary series without a booster dose, along with a 1-dose catch-up campaign for children aged >4 years. The rate of invasive Hib disease decreased from 22.9 cases per 100,000 children aged <5 years in 1990 to 0.65 cases per 100,000 in 1997. But beginning in 1999, the rate of Hib disease increased again, to 4.6 cases per 100,000 children aged <5 years in 2002 (9). One factor likely contributing to this increase was insufficient direct protection and herd immunity because of waning immunity in the absence of a routine Hib booster dose, prompting the United Kingdom to recommend a booster dose in 2003. Based on the United Kingdom experience, prolonged deferral of the Hib booster in the United States might lead to an increase in Hib colonization and disease. Continued surveillance for invasive H. influenzae disease enables monitoring of vaccine failures and potential changes in the epidemiology of non-b H. influenzae serotypes. CDC currently uses surveillance data to 1) monitor rates of Hib disease, 2) evaluate the impact of deferring the age 12--15 month Hib vaccine booster dose, and 3) inform other vaccination recommendations. With continuation of the vaccine shortage, H. influenzae surveillance takes on increased importance because the shortage might lead to increased Hib colonization, transmission, and eventually Hib disease. However, as the analysis in this report indicates, national surveillance is hampered by incomplete serotype reporting. For children aged <5 years, serotype data are missing for nearly 40% of cases reported to CDC. Although serotype data are more complete from jurisdictions participating in ABCs, the data from that system represent only 12% of the U.S. population. Because changes in the epidemiology of Hib disease resulting from the vaccine shortage might by unevenly distributed on a national level, more complete reporting of H. influenzae serotypes is needed for effective surveillance. National reporting of H. influenzae serotypes requires obtaining appropriate clinical specimens for confirmation of suspected H. influenzae, sending isolates to a laboratory capable of serotyping using standard procedures (10), reporting cases to local health departments, and successfully transmitting data through NNDSS. In 2006, after CDC follow-up with state health departments, the percentage of case reports transmitted through NNDSS with missing serotype data was reduced from 48.6% to 38.0% (K. Brown, CDC, personal communication, 2008). Coupled with the observation that jurisdictions participating in ABCs had fewer case reports with missing serotype data than jurisdictions not participating in ABCs, the follow-up results suggest that enhanced surveillance efforts can improve serotype reporting. To improve Hib surveillance, CDC will contact state health departments reporting H. influenzae disease cases in children aged <5 years during the next several months to solicit serotype information and vaccination history. Health-care providers should contact the local health department when invasive H. influenzae is suspected. Health departments and state and hospital laboratories should increase efforts for timely serotyping and reporting of all cases of invasive H. influenzae disease in children aged <5 years. Acknowledgment The findings in this report are based, in part, on data contributed by state and local health departments and the Active Bacterial Core surveillance team. References
* Five states are entirely covered by ABCs for H. influenzae disease: Connecticut, Maryland, Minnesota, New Mexico, and Oregon. Five other states are partially covered by ABCs: California (three-county San Francisco Bay area), Colorado (five-county Denver area), Georgia (20-county Atlanta area), New York (15 counties), and Tennessee (11 counties).
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 11/20/2008 |
|||||||||
|