|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
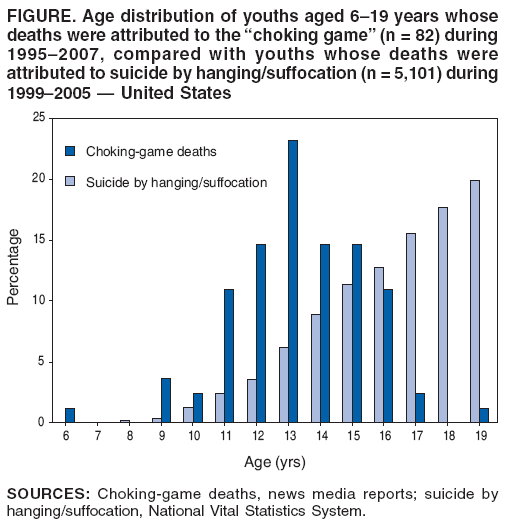
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Unintentional Strangulation Deaths from the "Choking Game" Among Youths Aged 6--19 Years --- United States, 1995--2007The "choking game" is defined as self-strangulation or strangulation by another person with the hands or a noose to achieve a brief euphoric state caused by cerebral hypoxia. Participants in this activity typically are youths (1). Serious neurologic injury or death can result if strangulation is prolonged. In recent years, news media reports have described numerous deaths among youths attributed to the choking game. Because no traditional public health dataset collects mortality data on this practice, CDC used news media reports to estimate the incidence of deaths from the choking game. This report describes the results of that analysis, which identified 82 probable choking-game deaths among youths aged 6--19 years, during 1995--2007. Seventy-one (86.6%) of the decedents were male, and the mean age was 13.3 years. Parents, educators, and health-care providers should become familiar with warning signs that youths are playing the choking game (2). Death certificates lack the detail necessary to distinguish choking-game deaths from other unintentional strangulation deaths. Therefore, CDC identified probable choking-game deaths from 1) a LexisNexis* search in November 2007 of newspaper reports since the 1970s and 2) reports on two choking-game--awareness websites,† which were created in 2005 and 2006. Deaths of children listed on the two websites but not matched by LexisNexis newspaper reports were included in the assessment only if subsequent Internet searches located news media reports (e.g., from television stations) of the incidents confirming that the deaths met the case definition. For consistency, case characteristics were obtained only from news media reports. A case was defined as a death, described in a news report, resulting from self-strangulation or strangulation by another person as part of an activity with elements of the choking game (also known as the "blackout game," "pass-out game," "scarf game," "space monkey," and by other names). Deaths were excluded if reports included any mention of autoerotic asphyxiation, a practice of choking oneself during sexual stimulation that is usually engaged in by teen-aged or adult males (1). Deaths also were excluded if reports noted that the medical examiner ruled the death was a suicide or of undetermined intent coupled with no mention of elements of the choking game, or if the age of the decedent was missing from news reports. Cases were restricted to youths aged <20 years who were residents of the United States. Following are two examples of cases of choking-game deaths. Case 1. In February 2006, an adolescent boy aged 13 years came home from school in a good mood and had dinner with his family. He then went to his bedroom to do his homework. Approximately 1 hour later, his mother went to check on him and discovered him slumped in a corner with a belt around his neck. His face was blue. The mother began cardiopulmonary resuscitation while one of the other children called an ambulance. The boy died at a local hospital 1 hour later. No suicide note was found. The county medical examiner ruled that the death resulted from accidental asphyxiation by hanging. In the weeks following his death, multiple teens told the director of a local counseling agency that the choking game had been played at local parties. Case 2. In April 2005, an adolescent girl aged 13 years was found dead, hanging from a belt and shoelace made into a noose on the door of her bedroom closet, after her brother went to her room to see why she had not come down for breakfast. No suicide note was found. The medical examiner determined that the teen had died at 9:30 p.m. the previous night. After the teen's death, the family learned that the girl had confided in a cousin that she recently had played the choking game in the locker room at school and that a group of girls at her school had been suspended for playing the choking game. The LexisNexis search and follow-up Internet searches for confirmatory news reports on deaths from the two choking-game websites produced 106 deaths that referred to the choking game. A total of 24 of the deaths were excluded: 20 because news reports either provided no evidence of the choking game or because the medical examiner ruled the death was of undetermined intent, three because the death circumstances had autoerotic elements, and one because no age of the decedent was reported. Among the remaining 82 deaths, 49 (59.8%) were identified via LexisNexis, and 72 (87.8%) were collected from the choking-game websites. LexisNexis was the sole source for 10 (12.2%) of the deaths, and the websites were the sole initial source for 33 (40.2%) of the deaths; 39 (47.6%) deaths were identified by both sources. The median period between the date of death and the news media report was 33.5 days (range: 2 days--6 years). The earliest choking-game death was identified as occurring in 1995. Three or fewer deaths occurred annually during 1995--2004; however, 22 deaths occurred in 2005, 35 in 2006, and nine in 2007. Seventy-one (86.6%) of the 82 decedents were male, and the age range of decedents was 6--19 years, with a mean age of 13.3 years (standard deviation = 2.1) and a median age of 13 years. Age distribution of the 82 choking-game decedents during 1995--2007 differed from that of the 5,101 youths aged 6--19 years whose deaths were attributed to suicide by hanging/suffocation during 1999--2005§ (Figure). Among the 70 deaths for which sufficient detail was reported, 67 (95.7%) occurred while the decedent was alone. Among the 42 deaths for which sufficient detail was reported, 39 (92.9%) parents of decedents said they were not aware of the choking game until the death of their child. Choking-game deaths occurred in 31 states; no geographic clustering was evident. Deaths did not vary significantly by season or by day of the week. No information regarding decedent drug use, race/ethnicity, or socioeconomic status was available. Reported by: P Russell, MD, MultiCare Health System, Tacoma, Washington. L Paulozzi, MD, J Gilchrist, MD, Div of Unintentional Injury Prevention, National Center for Injury Prevention and Control; R Toblin, PhD, EIS Officer, CDC. Editorial Note:This report describes the first attempt to assess the national incidence of deaths among youths resulting from the choking game. Although asphyxial games might have been played by youths for generations, the use of a ligature while playing alone appears to be a new practice that can be fatal (1). A search of medical literature produced no mention of the choking game until 2000. Information on the prevalence of this behavior is limited to the results of the 2006 Williams County (Ohio) Youth Health Risk Behavioral Survey, which included a question on the choking game. In that survey, 11% of youths aged 12--18 years, and 19% of youths aged 17--18 years reported ever playing the choking game (3). In this analysis, most decedents were males aged 11--16 years. These demographics are consistent with greater risk-taking behavior among boys than girls, beginning before adolescence (4). The data also are consistent with previous case studies (2,5--7) and with the sex and age distribution for decedents aged 6--19 years whose deaths are attributed to all types of unintentional choking/suffocation. However, the age distribution differs from the distribution for suicides by hanging/suffocation. The age distribution for choking-game deaths among youths aged 6--19 years followed a normal distribution with a peak at age 13 years; deaths from suicide by hanging/suffocation among those aged 6--19 years increased steadily through age 19 years. Whether choking-game incidence has changed in recent years is uncertain (1). The increases in news media reports of choking-game deaths from three or fewer reports during 1995--2004 to 22 in 2005 and 35 in 2006 might indicate an increase in choking-game activity; however, the increase in reports also might indicate greater interest by the news media after the choking game was featured on national television (1). Conversely, the decrease to nine news media reports of choking-game deaths in 2007 might indicate a decrease in choking-game activity or waning news media attention. The findings in this report are subject to at least two limitations. First, the use of news media reports for mortality surveillance incurs the risk of low sensitivity and specificity. LexisNexis does not include all newspapers and does not include most (e.g., local) television news reports. In this assessment, a LexisNexis search identified only 59.8% of decedents, compared with 87.8% of decedents identified on the two choking-game awareness websites. Even when all newspapers in an area are examined, their sensitivity for unintentional injury surveillance has ranged from 59% for drowning deaths (8) to 96% for deaths from fires (9) and has been reported as low as 13% for homicides (10). Further, this approach cannot be used to assess or characterize nonfatal injuries resulting from the choking game (2,6,7). Additionally, newspaper reports might attribute deaths to causes or intents that differ from those recorded on death certificates (8). In the design used in this study, information from news media reports could not be subjected to independent verification. Second, news media reports usually did not provide information on characteristics such as race/ethnicity, education, income, or the role of influence by peers or the media/Internet; therefore, analysis of these characteristics was not possible. In this study, few of the parents of children who died had been familiar with the choking game. Parents, educators, and health-care providers should learn about the choking game and be able to recognize any of the following warning signs in youths: mention of the choking game (or the game by its other names); bloodshot eyes; marks on the neck; frequent, severe headaches; disorientation after spending time alone; and ropes, scarves, and belts tied to bedroom furniture or doorknobs or found knotted on the floor (2). Medical examiners and coroners should be aware of the choking game as a possible explanation for deaths from self-inflicted strangulation in this age group that otherwise might be miscategorized as suicides (1,2). In addition, better mortality surveillance is needed, and more research should be conducted (e.g., questions on youth-behavior surveys regarding awareness of and involvement in the choking game) to determine prevalence, risk factors, and protective factors that will lead to effective interventions aimed at reducing or eliminating choking-game participation and deaths. References
* Available at http://www.lexisnexis.com. † Available at http://www.chokinggame.net and http://www.stop-the-choking-game.com. § National Vital Statistics System data obtained via the Web-based Injury Statistics Query and Reporting System at http://www.cdc.gov/ncipc/wisqars/default.htm. The 1999--2005 period was chosen because 2005 was the most recent year of data available and 1999 was the first year of mortality coding by the International Classification of Diseases, Tenth Revision.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 2/14/2008 |
|||||||||
|