|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
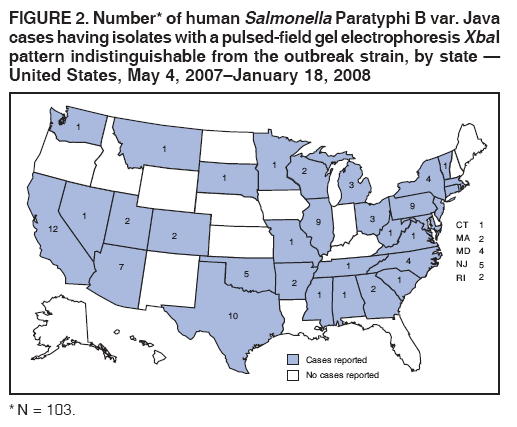
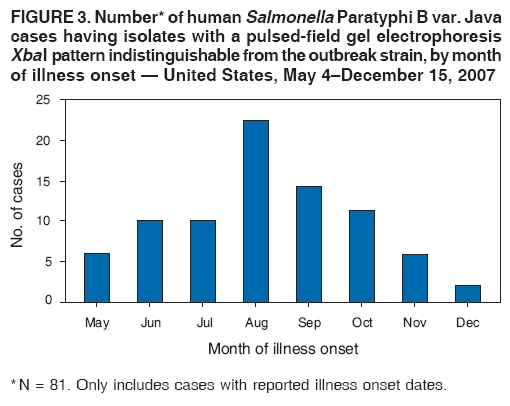
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Multistate Outbreak of Human Salmonella Infections Associated with Exposure to Turtles --- United States, 2007--2008Turtles and other reptiles have long been recognized as a source of human Salmonella infections (1). To prevent turtle-associated Salmonella infections in humans, the sale and distribution of small turtles (i.e., those with a carapace length of less than 4 inches) (Figure 1) has been prohibited in the United States since 1975.* Despite this prohibition, small turtles remain available to the public from various sources, including pet shops, flea markets, street vendors, and Internet websites (2,3). In October 2007, the North Carolina Division of Public Health (NCDPH) notified CDC of human infections caused by Salmonella serotype Paratyphi B L (+) tartrate (+) (Salmonella Paratyphi B var. Java) in several states. Salmonella Paratyphi B var. Java is a nontyphoidal strain of Salmonella that causes gastroenteritis. This report describes the results of the epidemiologic and laboratory investigation conducted by CDC and state and local health departments during October 2007--January 2008. The findings document an ongoing, multistate outbreak of Salmonella Paratyphi B var. Java infections, with the first reported illness onset occurring on May 4, 2007. Many of these infections have occurred in young children and have been associated with exposure to small turtles. Prohibiting the sale and distribution of small turtles likely remains the most effective public health action to prevent turtle-associated salmonellosis. Detection of the OutbreakOn August 31, 2007, a girl aged 13 years visited a South Carolina hospital emergency department, where she reported a 5-day history of bloody diarrhea, abdominal cramps, fever, and vomiting. She was treated with trimethoprim-sulfamethoxazole and intravenous fluids but was not hospitalized. Her illness resolved in 7 days. A stool specimen yielded Salmonella Paratyphi B var. Java. Also on August 31, a girl aged 15 years was admitted to a North Carolina hospital with acute renal failure and a 4-day history of bloody diarrhea, abdominal cramps, fever, and vomiting. She was hospitalized for 8 days and recovered fully. A joint investigation by NCDPH and the South Carolina Department of Health and Environmental Control revealed that, on August 24, the two girls had swum in an unchlorinated, in-ground swimming pool belonging to the family of the older girl. Two pet turtles belonging to the family also were permitted to swim in the pool. The turtles, both of which had carapace lengths of less than 4 inches, had been purchased recently from a pet shop in South Carolina. A water sample collected from the turtle habitat yielded Salmonella Paratyphi B var. Java with an XbaI pattern indistinguishable by pulsed-field gel electrophoresis (PFGE) from the isolates of the younger girl. Stool specimens were not collected from the older girl. On October 5, NCDPH informed PulseNet† that tests of isolates from three other persons revealed Salmonella Paratyphi B var. Java with an XbaI pattern indistinguishable from the isolates of the younger girl and the turtle habitat (defined as the outbreak strain). On October 5, in response to a request issued by NCDPH through PulseNet, several other state health departments reported human Salmonella Paratyphi B var. Java isolates with an XbaI pattern indistinguishable from the outbreak strain. The Ohio Department of Health provided further evidence of a turtle-associated outbreak by reporting that isolates indistinguishable from the outbreak strain had been obtained from a patient with exposure to a small turtle during the week before illness onset, from that patient's pet turtle, and from water collected from the turtle's habitat. Multistate InvestigationAfter NCDPH contacted CDC on October 23 about the possible cluster of turtle-associated Salmonella Paratyphi B var. Java infections, CDC and state and local health departments initiated a multistate investigation to determine the extent of the outbreak and the sources of infection. A case was defined as a diarrheal illness with onset after May 1, 2007, in a person from whom a clinical specimen yielded Salmonella Paratyphi B var. Java with a PFGE XbaI pattern indistinguishable from the outbreak strain; cases were identified by a review of all PFGE-typed isolates in the PulseNet database. As of January 18, 2008, a total of 103 cases with isolates indistinguishable from the outbreak strain had been reported to CDC from 33 states (Figure 2). Information initially was collected from general enteric disease questionnaires administered by state and local health departments. Of the 100 patients for whom age information was available (median age: 7.5 years; range: <1--87 years), 56 (56%) were aged <10 years. Fifty-two (51%) of the 101 patients for whom the sex was known were female. Illness onset dates ranged from May 4, 2007, to December 15, 2007 (Figure 3). Among the 78 patients for whom clinical information was available, 51 (65%) reported bloody diarrhea, with a median duration of illness of 7 days; 24 (30%) of the 80 patients for whom hospitalization status was known were hospitalized for their illnesses, with a median duration of 4 days. Among the 80 patients questioned about turtle exposure, 47 (59%) reported turtle exposure during the 7 days before illness onset. No deaths were reported. A case-control study was conducted during November 15--December 5 using age- and neighborhood-matched controls (age groups: <1 year, 1--9 years, 10--19 years, 20--49 years, >50 years; reverse-digit dialing was used to match cases to controls by neighborhood). A telephone questionnaire was used to determine whether the case-patient or control had exposure to turtles, other reptiles, or aquariums containing tropical fish during a 7-day exposure period (7 days before illness onset in the case-patient, for both cases and matched controls). Participants who reported exposure to turtles were asked about the nature of the exposure, including whether the patient had touched or held the turtle, kissed the turtle or put the turtle in his or her mouth, or come into contact with the turtle's habitat, such as by changing the water or cleaning the cage. Participants who reported exposure to turtles also were asked about turtle size, type, and source. All participants were asked about their awareness of the association between contact with reptiles and Salmonella infection. Seventy case-patients and 45 matched controls were enrolled in the study. Among the 70 case-patients interviewed, 44 (63%) reported exposure to a turtle during the 7 days before illness onset, compared with two (4%) of 45 controls (matched odds ratio [mOR] = 40.9; 95% confidence interval [CI] = 7.0--unbounded). Two (3%) case-patients and four (9%) controls reported exposure to a reptile other than a turtle during the 7 days before illness onset. No other single characteristic for which data were collected has been implicated in this outbreak. Twelve (20%) of the 60 case-patients for whom such information was available and 13 (29%) of the 45 controls reported awareness of the association between contact with reptiles and Salmonella infection (mOR = 0.66; CI = 0.27--1.6). Among the 44 case-patients exposed to a turtle, 34 (77%) were exposed at home, and nine (20%) were exposed at the home of a friend or relative; one (2%) was exposed outdoors. Of the 43 case-patients exposed at home or at the home of a friend or relative, three were siblings exposed to turtles at the home of their babysitter, and two were a husband and wife exposed to a turtle in their own home; the remaining exposures occurred in households independent of one another. Of 34 case-patients exposed to turtles at home, 12 (35%) still owned the turtle at the time of interview. Of the 42 case-patients for whom the details of the turtle exposure were known, 28 (67%) reported holding or touching the turtle, 24 (57%) reported feeding the turtle, and 29 (69%) reported contact with the turtle's habitat. Four (10%) case-patients reported kissing the turtle or having put the turtle in his or her mouth. Thirty-seven (86%) of the 43 case-patients who were exposed to a turtle and for whom turtle size information was available reported that the turtle had a carapace length of less than 4 inches; the remaining turtles involved in these exposures were reported to have carapace lengths of 4 inches or more. Forty-two case-patients with turtle exposure reported details about the turtle source. Fifteen (36%) reported that the turtle was purchased at a pet shop, 10 (24%) reported that the turtle had been a gift, eight (19%) reported that the turtle was purchased at a flea market, five (12%) reported that the turtle was purchased from a street vendor, and one each (2%, respectively) reported that the turtle was purchased on an Internet website, acquired from the wild, hatched from an egg given by a relative, or purchased at a conference center event. Salmonella Paratyphi B var. Java matching the outbreak strain was isolated from six turtles or the water from their habitats in the homes of case-patients in California, North Carolina, Ohio, and Wisconsin. Investigations are ongoing to determine whether the turtles have a common distributor or farm of origin. Reported by: D Bergmire-Sweat, MPH, North Carolina Div of Public Health. J Schlegel, MSP, C Marin, South Carolina Dept of Health and Environmental Control. K Winpisinger, MS, Ohio Dept of Health. C Perry, M Sotir, PhD, Div of Foodborne, Bacterial, and Mycotic Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases; J Harris, PhD, EIS Officer, CDC. Editorial Note:This ongoing, multistate outbreak of salmonellosis is associated with small turtles purchased at pet stores, flea markets, and other outlets, despite a federal prohibition on the sale of turtles with carapace lengths of less than 4 inches. These turtles are a risk to the public and especially to young children. Other outbreaks of turtle-associated Salmonella infections have been reported (2,3). The prohibition on the sale and distribution of small turtles was enacted in 1975, after public health investigations demonstrated that small turtles were a major source of human Salmonella infections, particularly in children. In 1972, a study in New Jersey indicated that small pet turtles accounted for approximately 23% of Salmonella infections in children (4). In 1980, the 1975 prohibition was estimated to have prevented 100,000 Salmonella infections in U.S. children each year since going into effect (5). However, this prohibition has an exception: small turtles may be sold legally for scientific, educational or exhibition purposes. During 2001--2006, the number of turtles kept as pets in the United States increased 86% to nearly 2 million turtles (6), suggesting that this exception might provide a mechanism by which small turtles become household pets. Turtles, like other reptiles, commonly carry Salmonella, and fecal carriage rates can be as high as 90% (1). Small turtles sold as pets frequently come from breeding farms, where turtles are housed in crowded ponds and nesting areas in a way that promotes Salmonella transmission (7). Attempts to treat turtles, turtle eggs, and turtle breeding ponds with antibiotics to eliminate Salmonella have not been successful and have resulted in a high prevalence of antibiotic resistance (7,8). Other treatments reduce but do not eliminate Salmonella shedding from turtles (8), and the turtles that continue to shed Salmonella might recontaminate other turtles during rearing or shipment. Because Salmonella shedding might be intermittent and stress related, determining whether turtles are free of the bacteria is difficult (1). Direct or indirect contact with a reptile is associated with an estimated 6% of human Salmonella infections in the United States (9). Persons coming into contact with reptiles, reptile habitats, or surfaces contaminated with reptile fecal matter risk infection from salmonellae shed by the reptile (10). Although most reptiles carry Salmonella, small turtles are likely to be handled differently than other reptiles and thus carry a greater risk of transmitting Salmonella to children. In contrast to the obvious risk for a bite or scratch, for example, from a snake or an iguana, a small turtle is likely to be perceived as safe, and thus might be given directly to small children to play with. In addition, a young child placed in charge of caring for a turtle has direct contact with water in the turtle habitat, where Salmonella are likely to multiply to high numbers. Although approximately half of the infections associated with this outbreak occurred in young children, who are at greater risk for severe illness from Salmonella infection (2,10), several illnesses occurred in adults with turtle exposure, demonstrating that turtle-associated Salmonella infection is not unique to children. Additionally, only 20% of case-patients interviewed reported awareness of the link between Salmonella and contact with reptiles, indicating that measures to educate the public about this link have not been successful. CDC has provided recommendations to prevent reptile-associated salmonellosis in humans (2). However, because of the particular hazard associated with small turtles, prohibiting the sale and distribution of small turtles likely remains the most effective public health action to prevent turtle-associated salmonellosis. Acknowledgments The findings in this report are based, in part, on contributions from R Reporter, MD, R Bagby, Los Angeles County Dept of Public Health, A Kao, PhD, San Diego Health and Human Svcs Agency, E Cox, MPH, Long Beach Dept of Health and Human Svcs, P Cast, San Bernardino County Dept of Public Health, A Norman, Sacramento Dept of Health and Human Svcs, A Kimura, MD, California Dept of Health; D Raccasi, T L'Estrange, Weber-Morgan Health Dept, Utah Dept of Health; Missouri Dept of Health and Senior Svcs; C Prunty, Summit County Health Dept, P Pflum, Henry Country Health Dept, Ohio; J Tait, J Baney, CR Cook, CH Sandt, PhD, Pennsylvania Bur of Laboratories, K Warren, MPH, Pennsylvania Dept of Health; Y Khachadourian, T Quinlan, Wadsworth Center Laboratory, New York, T Fitzgerald, New York City Bur of Health, E Villamil, MPH, Perry Smith, MD, New York State Dept of Health; M Cumming, MS, B Bolstorff, MPH, Massachussetts Dept of Public Health; S Bidol, MPH, Michigan Dept of Community Health; and L Schaefer, South Dakota Dept of Health. References
* Food and Drug Administration. Human health hazards associated with turtles: information for regulators and public health educators. Available at http://www.fda.gov/cvm/turtlereg.htm. †
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 1/24/2008 |
|||||||||
|